Optical Coherence Tomography Parameters as Predictors of Treatment Response to Eplerenone in Central Serous Chorioretinopathy

 , ,
, , 
Abstract
:1. Introduction
2. Methods
2.1. Study Participants
2.2. Imaging Protocol
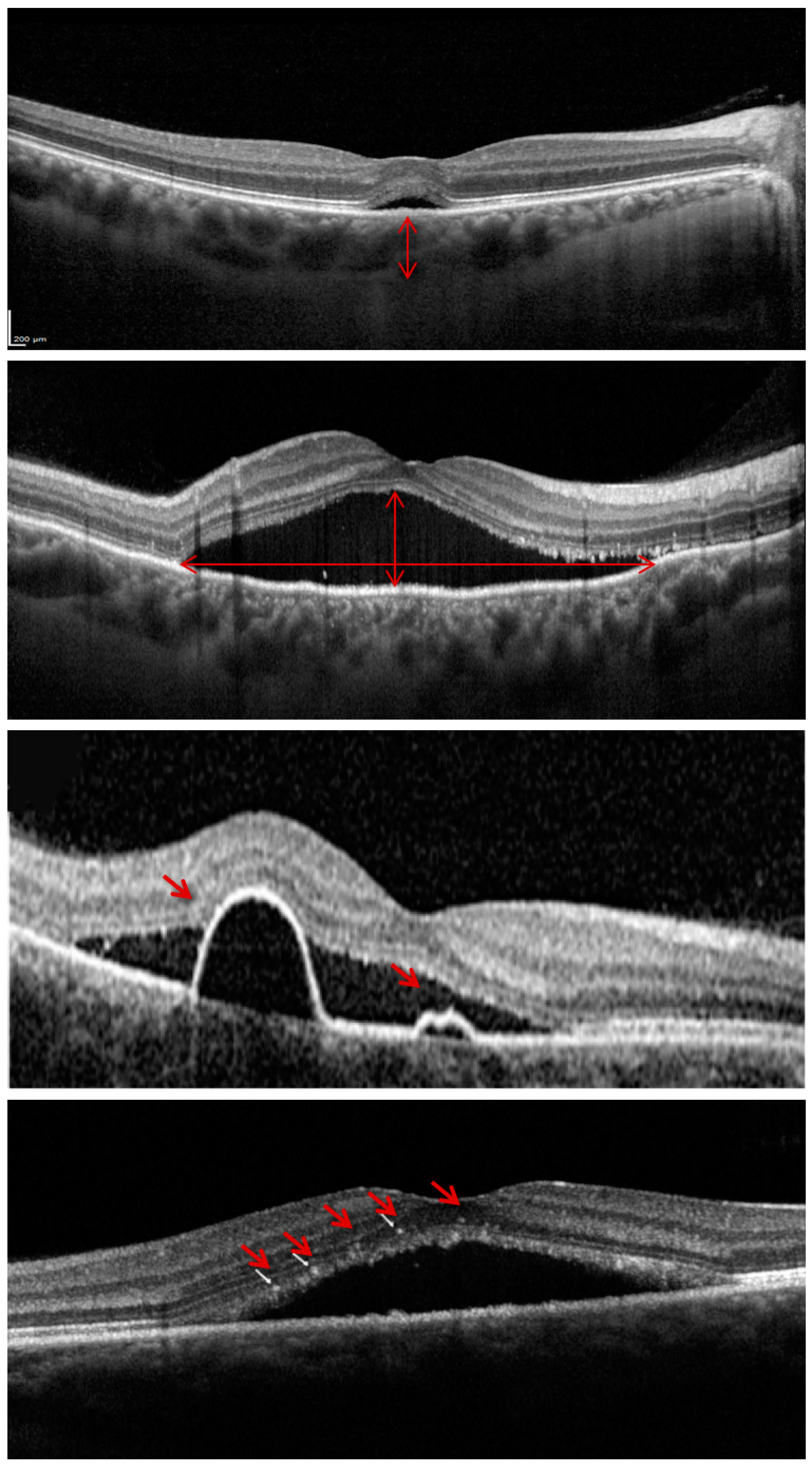
2.3. OCT Analysis
2.4. Statistical Analysis
3. Results
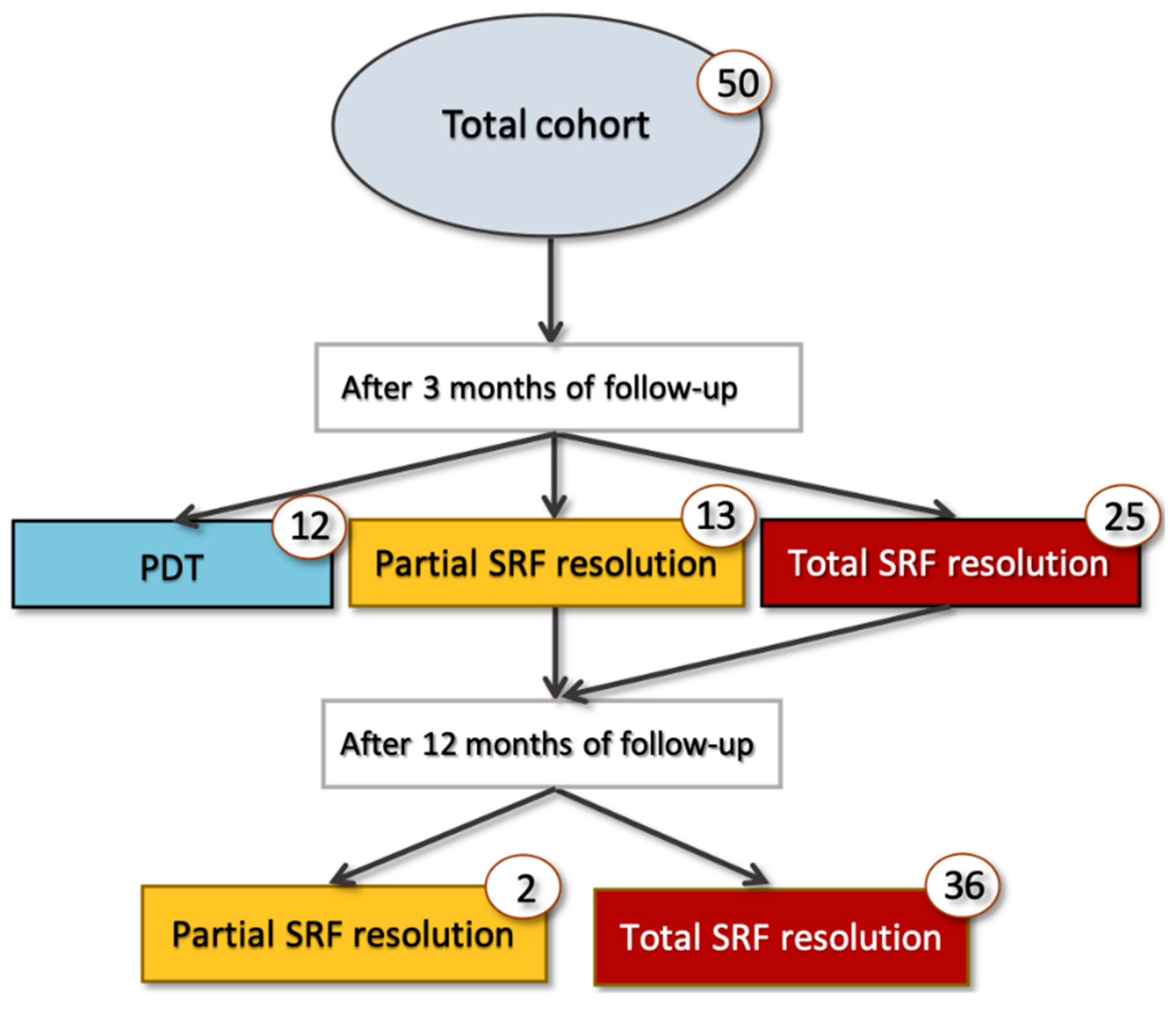
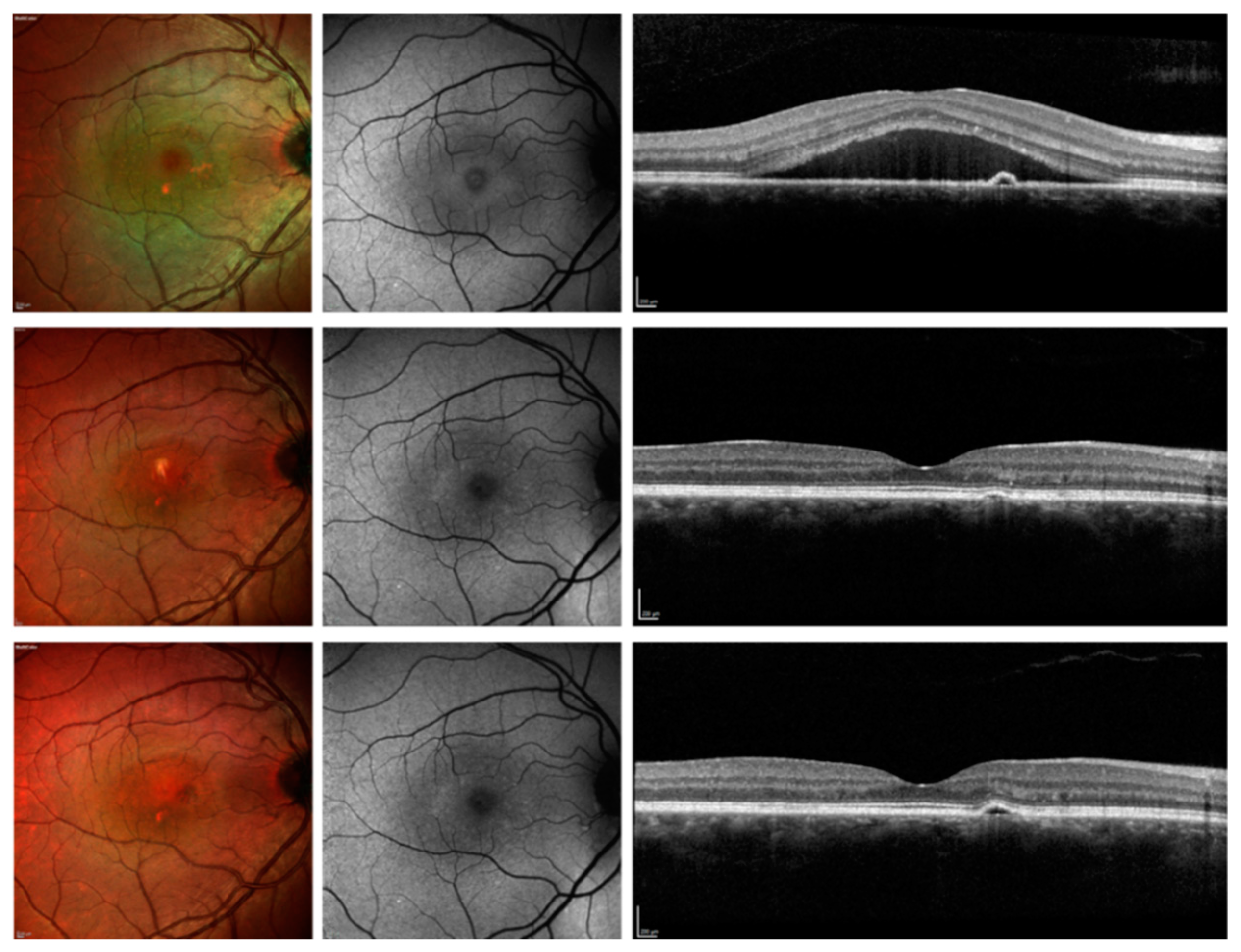
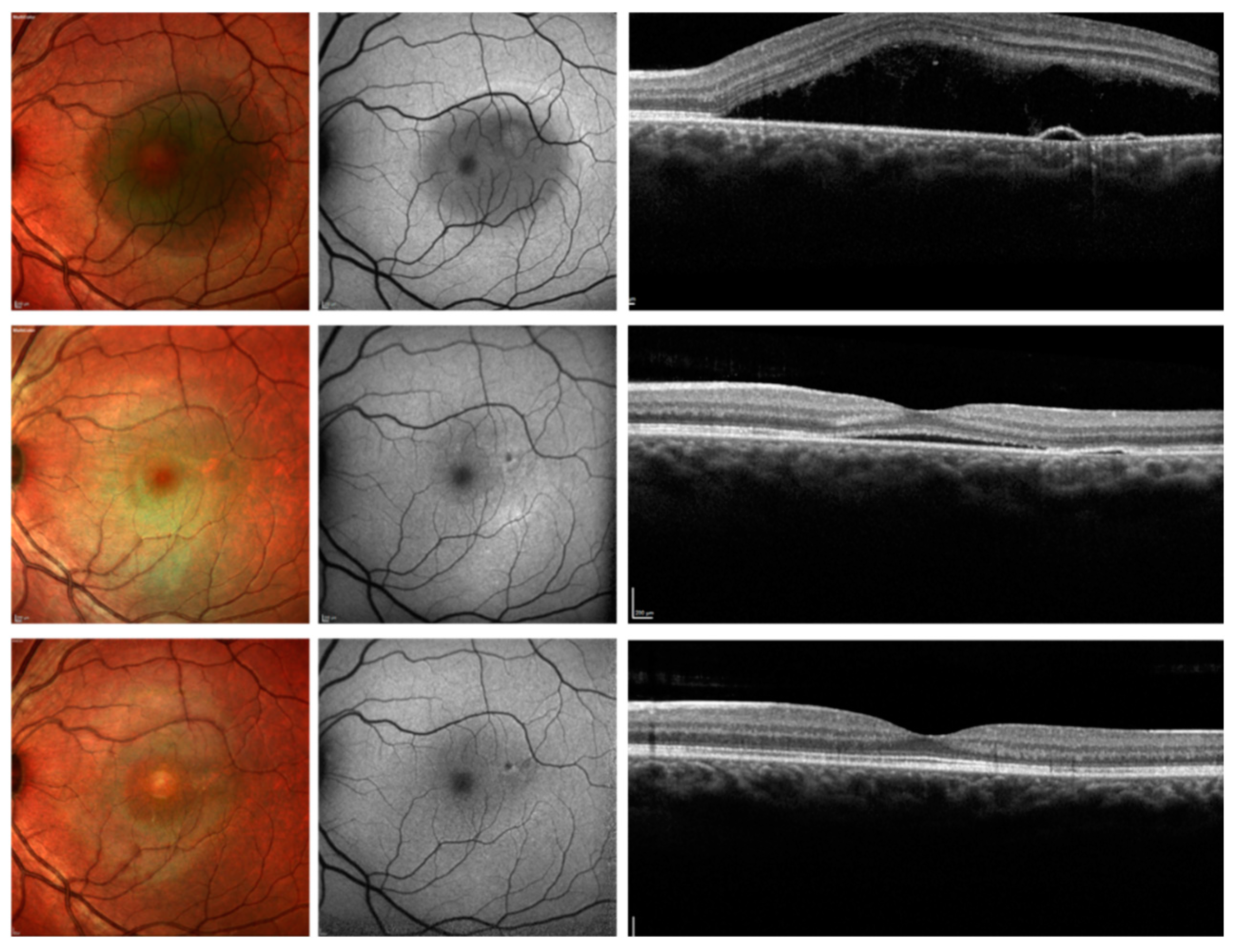
3.1. Clinical Changes During Follow-up
3.2. Logistic Regression Analysis
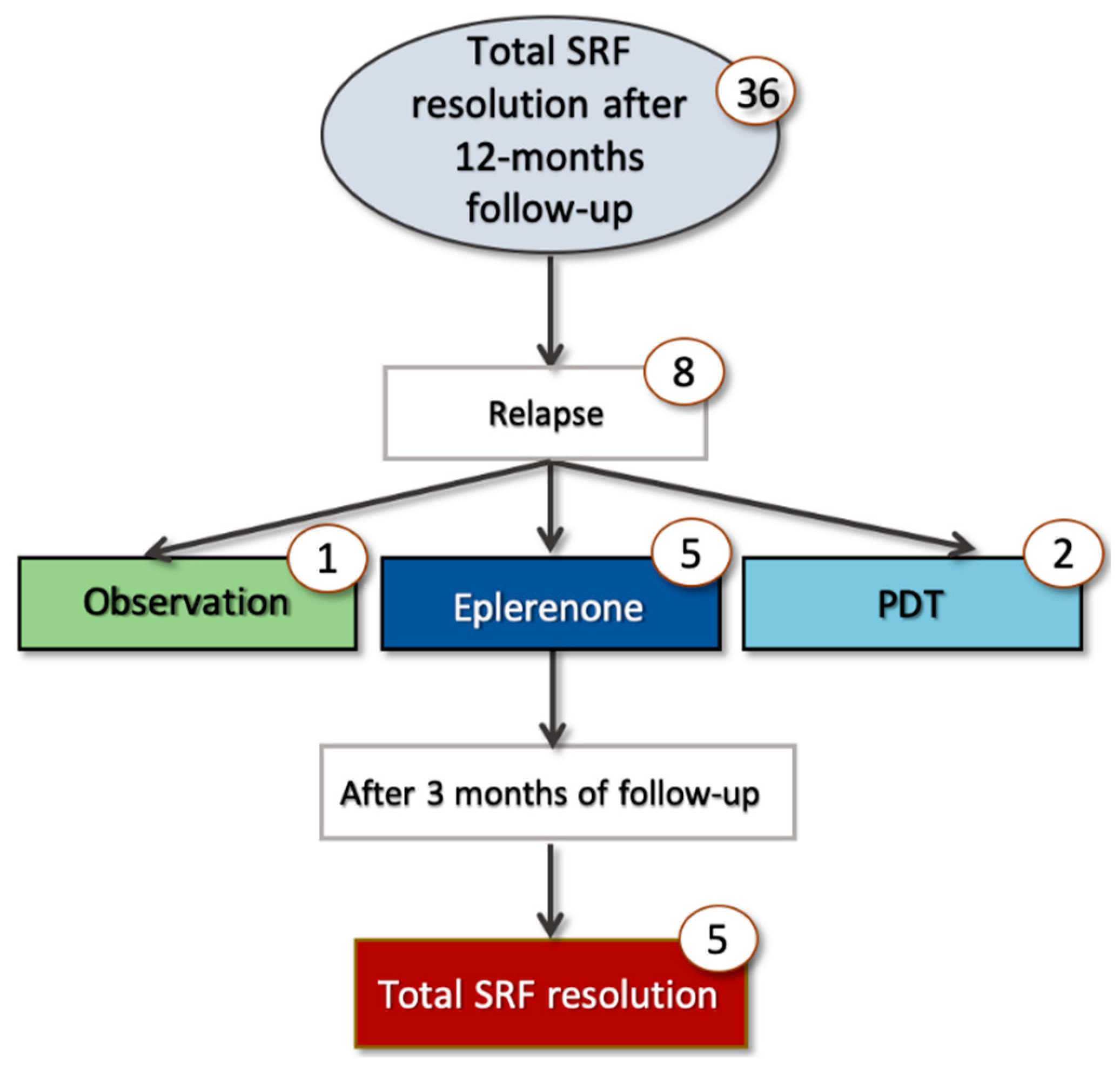
3.3. Subanalysis in Relapsing Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kitzmann, A.S.; Pulido, J.S.; Diehl, N.N.; Hodge, D.O.; Burke, J.P. The Incidence of Central Serous Chorioretinopathy in Olmsted County, Minnesota, 1980–2002. Ophthalmology 2008, 115, 169–173. [Google Scholar] [CrossRef] [PubMed]
- Quin, G.; Liew, G.; Ho, I.-V.; Gillies, M.; Fraser-Bell, S. Diagnosis and interventions for central serous chorioretinopathy: Review and update. Clin. Exp. Ophthalmol. 2013, 41, 187–200. [Google Scholar] [CrossRef] [PubMed]
- Loo, R.H.; Scott, I.U.; Flynn, H.W.; Gass, J.D.M.; Murray, T.G.; Lewis, M.L.; Rosenfeld, P.J.; Smiddy, W.E. Factors associated with reduced visual acuity during long-term follow-up of patients with idiopathic central serous chorioretinopathy. Retina 2002, 22, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M.; Célérier, I.; Bousquet, E.; Jeanny, J.-C.; Jonet, L.; Savoldelli, M.; Offret, O.; Curan, A.; Farman, N.; Jaisser, F.; et al. Mineralocorticoid receptor is involved in rat and human ocular chorioretinopathy. J. Clin. Investig. 2012, 122, 2672–2679. [Google Scholar] [CrossRef] [PubMed]
- Van Dijk, E.H.C.; Schellevis, R.L.; Van Bergen, M.G.J.M.; Breukink, M.B.; Altay, L.; Scholz, P.; Fauser, S.; Meijer, O.C.; Hoyng, C.B.; Hollander, A.I.D.; et al. Association of a Haplotype in the NR3C2 Gene, Encoding the Mineralocorticoid Receptor, with Chronic Central Serous Chorioretinopathy. JAMA Ophthalmol. 2017, 135, 446–451. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, R.; Habot-Wilner, Z.; Martinez, M.R.; Nutman, A.; Goldenberg, D.; Cohen, S.; Shulman, S.; Guzner-Gur, H.; Loewenstein, A.; Goldstein, M. Eplerenone for chronic central serous chorioretinopathy—A randomized controlled prospective study. Acta Ophthalmol. 2017, 95, e610–e618. [Google Scholar] [CrossRef] [PubMed]
- Bousquet, E.; Beydoun, T.; Rothschild, P.R.; Bergin, C.; Zhao, M.; Batista, R.; Brandely, M.L.; Couraud, B.; Farman, N.; Gaudric, A.; et al. Spironolactone for nonresolving central serous chorioretinopathy a randomized controlled crossover study. Retina 2015, 35, 2505–2515. [Google Scholar] [CrossRef] [PubMed]
- Zucchiatti, I.; Sacconi, R.; Parravano, M.C.; Costanzo, E.; Querques, L.; Montorio, D.; Bandello, F.; Querques, G. Eplerenone Versus Observation in the Treatment of Acute Central Serous Chorioretinopathy: A Retrospective Controlled Study. Ophthalmol. Ther. 2018, 7, 109–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Breukink, M.B.; Hollander, A.I.D.; Keunen, J.E.; Boon, C.J.; Hoyng, C.B. The use of eplerenone in therapy-resistant chronic central serous chorioretinopathy. Acta Ophthalmol. 2014, 92, e488–e490. [Google Scholar] [CrossRef]
- Montorio, D.; Carnevali, A.; Sacconi, R.; Capuano, V.; Giuffrè, C.; Rabiolo, A.; De Vitis, L.A.; Querques, L.; Bandello, F.; Querques, G. Mineralocorticoid receptor antagonists in the treatment of central serous chorioretinopathy. Expert Rev. Ophthalmol. 2017, 12, 21–25. [Google Scholar] [CrossRef]
- Ghadiali, Q.; Jung, J.J.; Yu, S.; Patel, S.N.; Yannuzzi, L.A. Central Serous Chorioretinopathy Treated With Mineralocorticoid Antagonists: A One-Year Pilot Study. Retina 2015, 36, 611–618. [Google Scholar] [CrossRef] [PubMed]
- Zola, M.; Daruich, A.; Matet, A.; Mantel, I.; Behar-Cohen, F. Two-year follow-up of mineralocorticoid receptor antagonists for chronic central serous chorioretinopathy. Br. J. Ophthalmol. 2018, 103, 1184–1189. [Google Scholar] [CrossRef] [PubMed]
- Van Rijssen, T.J.; Van Dijk, E.H.; Yzer, S.; Ohno-Matsui, K.; Keunen, J.E.; Schlingemann, R.O.; Sivaprasad, S.; Querques, G.; Downes, S.M.; Fauser, S.; et al. Central serous chorioretinopathy: Towards an evidence-based treatment guideline. Prog. Retin. Eye Res. 2019. [Google Scholar] [CrossRef] [PubMed]
- Lainscak, M.; Pelliccia, F.; Rosano, G.; Vitale, C.; Schiariti, M.S.M.; Greco, C.; Speziale, G.; Gaudio, C. Safety profile of mineralocorticoid receptor antagonists: Spironolactone and eplerenone. Int. J. Cardiol. 2015, 200, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Sacconi, R.; Baldin, G.; Carnevali, A.; Querques, L.; Rabiolo, A.; Marchini, G.; Bandello, F.; Querques, G. Response of central serous chorioretinopathy evaluated by multimodal retinal imaging. Eye 2018, 32, 734–742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bousquet, E.; Dhundass, M.; Lejoyeux, R.; Shinojima, A.; Krivosic, V.; Mrejen, S.; Gaudric, A.; Tadayoni, R. Predictive Factors of Response to Mineralocorticoid Receptor Antagonists in Nonresolving Central Serous Chorioretinopathy. Am. J. Ophthalmol. 2019, 198, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Gangaputra, S.; Lee, K.E.; Narkar, A.R.; Klein, R.; Klein, B.E.K.; Meuer, S.M.; Danis, R.P. Signal Quality Assessment of Retinal Optical Coherence Tomography Images. Investig. Opthalmol. Vis. Sci. 2012, 53, 2133–2141. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Lee, J.; Chung, H.; Kim, H.C. Baseline spectral domain optical coherence tomographic hyperreflective foci as a predictor of visual outcome and recurrence for central serous chorioretinopathy. Retina 2016, 36, 1372–1380. [Google Scholar] [CrossRef]
- Petkovsek, D.S.; Cherfan, D.G.; Conti, F.F.; Hom, G.L.; Ehlers, J.P.; Babiuch, A.S.; Rachitskaya, A.V.; Kaiser, P.K.; Schachat, A.P.; Srivastava, S.K.; et al. Eplerenone for the treatment of chronic central serous chorioretinopathy: 3-year clinical experience. Br. J. Ophthalmol. 2019. [Google Scholar] [CrossRef]
- Comyn, O.; Heng, L.Z.; Ikeji, F.; Bibi, K.; Hykin, P.G.; Bainbridge, J.W.; Patel, P.J. Repeatability of Spectralis OCT Measurements of Macular Thickness and Volume in Diabetic Macular Edema. Investig. Opthalmol. Vis. Sci. 2012, 53, 7754–7759. [Google Scholar] [CrossRef]
- Toto, L.; D’Aloisio, R.; Mastropasqua, R.; Di Antonio, L.; Di Nicola, M.; Di Martino, G.; Evangelista, F.; Erroi, E.; Doronzo, E.; Mariotti, C. Anatomical and Functional Changes of the Retina and the Choroid after Resolved Chronic CSCR. J. Clin. Med. 2019, 8, 474. [Google Scholar] [CrossRef] [PubMed]
- Hirami, Y.; Tsujikawa, A.; Sasahara, M.; Gotoh, N.; Tamura, H.; Otani, A.; Mandai, M.; Yoshimura, N. Alterations of retinal pigment epithelium in central serous chorioretinopathy. Clin. Exp. Ophthalmol. 2007, 35, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Van Rijssen, T.J.; Van Dijk, E.H.C.; Scholz, P.; Breukink, M.B.; Blanco-Garavito, R.; Souied, E.H.; MacLaren, R.E.; Querques, G.; Fauser, S.; Hoyng, C.B.; et al. Patient characteristics of untreated chronic central serous chorioretinopathy patients with focal versus diffuse leakage. Graefe’s Arch. Clin. Exp. Ophthalmol. 2019, 257, 1419–1425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herold, T.R.; Rist, K.; Priglinger, S.G.; Ulbig, M.W.; Wolf, A. Long-term results and recurrence rates after spironolactone treatment in non-resolving central serous chorio-retinopathy (CSCR). Graefes Arch. Clin. Exp. Ophthalmol. 2017, 255, 221–229. [Google Scholar] [CrossRef] [PubMed]
- Gergely, R.; Kovács, I.; Schneider, M.; Resch, M.; Papp, A.; Récsán, Z.; Nagy, Z.Z.; Ecsedy, M. Mineralocorticoid receptor antagonist treatment in bilateral chronic central serous chorioretinopathy. Retina 2017, 37, 1084–1091. [Google Scholar] [CrossRef] [PubMed]
- Nassisi, M.; Fan, W.; Shi, Y.; Lei, J.; Borrelli, E.; Ip, M.; Sadda, S.R. Quantity of Intraretinal Hyperreflective Foci in Patients With Intermediate Age-Related Macular Degeneration Correlates with 1-Year Progression. Investig. Opthalmol. Vis. Sci. 2018, 59, 3431–3439. [Google Scholar] [CrossRef] [PubMed]
- Benson, S.E.; Schlottmann, P.G.; Bunce, C.; Xing, W.; Charteris, D.G. Assessment of the reproducibility and repeatability of a method of grading macular subretinal fluid using optical coherence tomography. Eye 2006, 26, 1030–1033. [Google Scholar] [CrossRef]
- Ikuno, Y.; Maruko, I.; Yasuno, Y.; Miura, M.; Sekiryu, T.; Nishida, K.; Iida, T. Reproducibility of Retinal and Choroidal Thickness Measurements in Enhanced Depth Imaging and High-Penetration Optical Coherence Tomography. Investig. Opthalmol. Vis. Sci. 2011, 52, 5536–5540. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CSC Patients | |
|---|---|
| Number of eyes enrolled (patients) | 50 (50) |
| Age, years | 44.0 ± 8.9 |
| Gender | |
| M, n (%) | 45 (90%) |
| F, n (%) | 5 (10%) |
| Race | |
| M, n (%) | 50 (100%) |
| Form | |
| Acute | 14 (28%) |
| Chronic | 36 (72%) |
| Disease Duration, months | 37.8 ± 53.2 |
| Previous Treatments | |
| PDT | 6 (12.2%) |
| Laser | 0 (0%) |
| Anti-VEGF | 0 (0%) |
| BCVA, LogMAR | 0.20 ± 0.14 |
| Baseline | 3 Months | p Value | 12 Months | p Value | |
|---|---|---|---|---|---|
| Subfoveal Choroidal Thickness, μm | 398 (342–468) | 370 (329–442) | 0.046 | 396 (309–462) | 0.124 |
| Subfoveal Subretinal Fluid Height, μm | 169 (52–148) | 0 (0–84) | <0.0001 | 0 (0–24) | <0.0001 |
| Subretinal Fluid maximum Height, μm | 182 (97–272) | 68 (0–121) | <0.0001 | 0 (0–58) | <0.0001 |
| Subretinal Fluid Maximum Diameter, μm | 2449 (1351–3112) | 1065 (0–2307) | <0.0001 | 0 (0–726) | <0.0001 |
| Pigment Epithelium Detachments, n | 1 (0–2) | 0 (0–1) | 0.004 | 0 (0–1) | 0.003 |
| Hyperreflective Foci, n | 9 (4–18) | 5 (3–8) | <0.0001 | 0 (2–4) | <0.0001 |
| Predictor for Foveal Complete Resolution | 3 Months | 12 Months | ||||
|---|---|---|---|---|---|---|
| Odds Ratio | 95% CI | p Value | Odds Ratio | 95% CI | p Value | |
| Subfoveal Choroidal Thickness | 1.012 | 1.001–1.024 | 0.030 | 0.998 | 0.988–1.008 | 0.702 |
| Subfoveal Subretinal Fluid Height | 0.991 | 0.974–1.008 | 0.308 | 0.988 | 0.967–1.009 | 0.266 |
| Subretinal Fluid Maximum Height | 1.010 | 0.987–1.033 | 0.407 | 1.019 | 0.991–1.047 | 0.180 |
| Subretinal Fluid Maximum Diameter | 0.999 | 0.998–1.000 | 0.162 | 1.000 | 0.999–1.001 | 0.538 |
| Pigment Epithelium Detachments’ Number | 0.693 | 0.401–1.198 | 0.189 | 0.886 | 0.464–1.691 | 0.714 |
| Hyperreflective Foci Number | 0.972 | 0.874–1.060 | 0.543 | 1.014 | 0.909–1.110 | 0.779 |
| Age | 1.064 | 0.989–1.144 | 0.094 | 1.012 | 0.933–1.097 | 0.780 |
| Disease Duration | 0.995 | 0.982–1.008 | 0.456 | 1.004 | 0.989–1.019 | 0.618 |
| Previous Treatments | 0.971 | 0.911–1.031 | 0.515 | 1.007 | 0.982–1.032 | 0.218 |
| Predictor for Macular Complete Resolution | 3 Months (n = 50) | 12 Months (n = 39) | ||||
|---|---|---|---|---|---|---|
| Odds Ratio | 95% CI | p Value | Odds Ratio | 95% CI | p Value | |
| Subfoveal Choroidal Thickness | 1.021 | 1.004–1.038 | 0.013 | 0.991 | 0.978–1.004 | 0.158 |
| Subfoveal Subretinal Fluid Height | 1.000 | 0.982–1.018 | 0.969 | 0.997 | 0.978–1.015 | 0.719 |
| Subretinal Fluid Maximum Height | 1.017 | 0.914–1.017 | 0.211 | 1.023 | 0.994–1.053 | 0.129 |
| Subretinal Fluid Maximum Diameter | 0.996 | 0.994–0.999 | 0.013 | 1.000 | 0.999–1.001 | 0.984 |
| Pigment Epithelium Detachments’ Number | 0.259 | 0.088–0.759 | 0.012 | 0.817 | 0.326–2.047 | 0.667 |
| Hyperreflective Foci Number | 0.694 | 0.349–0.967 | 0.025 | 0.938 | 0.902–1.059 | 0.331 |
| Age | 1.173 | 0.972–1.232 | 0.012 | 1.006 | 0.923–1.097 | 0.887 |
| Disease Duration | 0.997 | 0.974–1.020 | 0.774 | 1.008 | 0.993–1.025 | 0.300 |
| Previous Treatments | 0.871 | 0.823–0.919 | 0.614 | 1.005 | 0.979–1.028 | 0.225 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borrelli, E.; Zuccaro, B.; Zucchiatti, I.; Parravano, M.; Querques, L.; Costanzo, E.; Sacconi, R.; Prascina, F.; Scarinci, F.; Bandello, F.; et al. Optical Coherence Tomography Parameters as Predictors of Treatment Response to Eplerenone in Central Serous Chorioretinopathy. J. Clin. Med. 2019, 8, 1271. https://doi.org/10.3390/jcm8091271
Borrelli E, Zuccaro B, Zucchiatti I, Parravano M, Querques L, Costanzo E, Sacconi R, Prascina F, Scarinci F, Bandello F, et al. Optical Coherence Tomography Parameters as Predictors of Treatment Response to Eplerenone in Central Serous Chorioretinopathy. Journal of Clinical Medicine. 2019; 8(9):1271. https://doi.org/10.3390/jcm8091271
Chicago/Turabian StyleBorrelli, Enrico, Biancamaria Zuccaro, Ilaria Zucchiatti, Mariacristina Parravano, Lea Querques, Eliana Costanzo, Riccardo Sacconi, Francesco Prascina, Fabio Scarinci, Francesco Bandello, and et al. 2019. "Optical Coherence Tomography Parameters as Predictors of Treatment Response to Eplerenone in Central Serous Chorioretinopathy" Journal of Clinical Medicine 8, no. 9: 1271. https://doi.org/10.3390/jcm8091271