Impact on Outcomes across KDIGO-2012 AKI Criteria According to Baseline Renal Function


Abstract
:1. Introduction
2. Experimental Section
3. Results
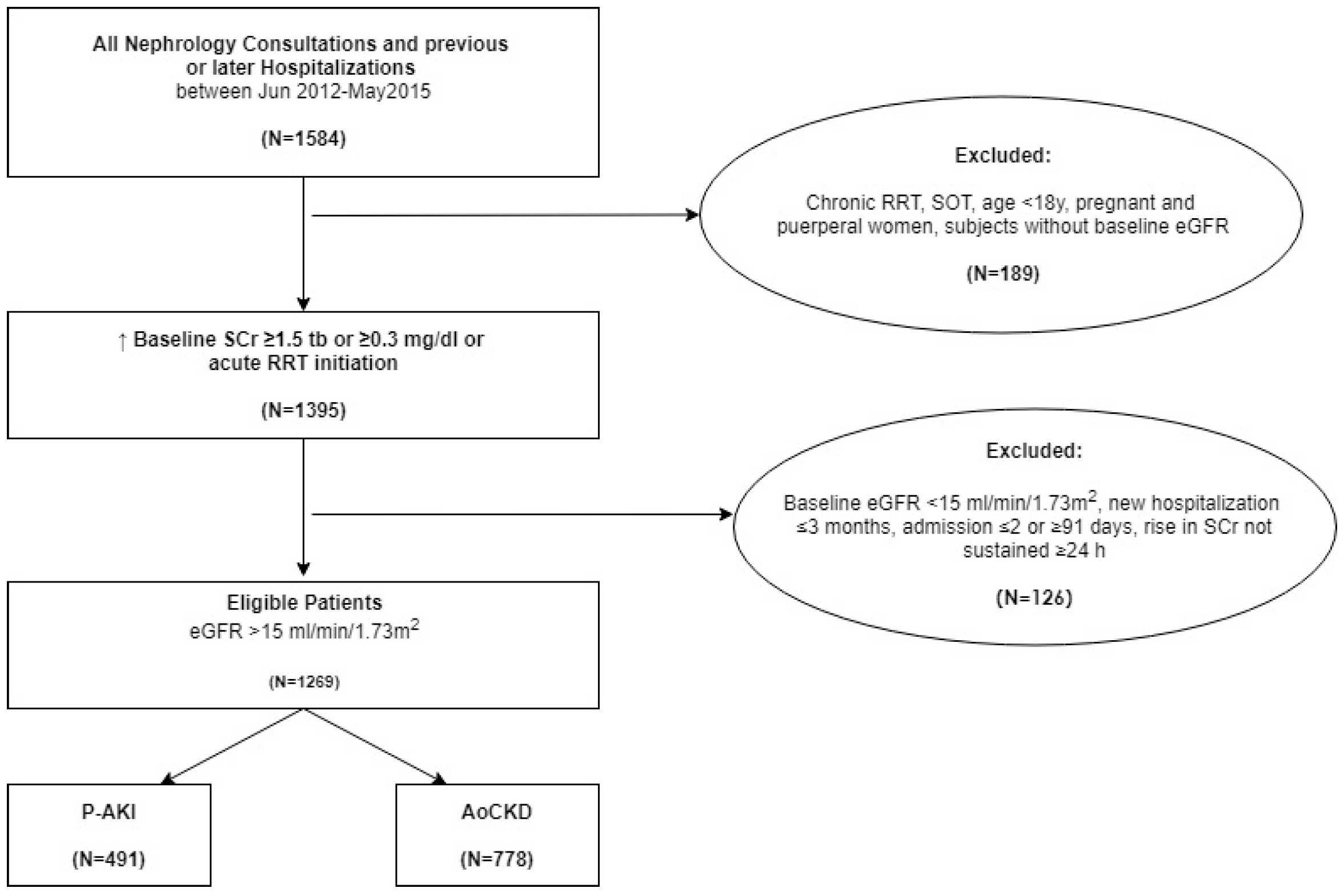
3.1. Demographic Characteristics of Patients
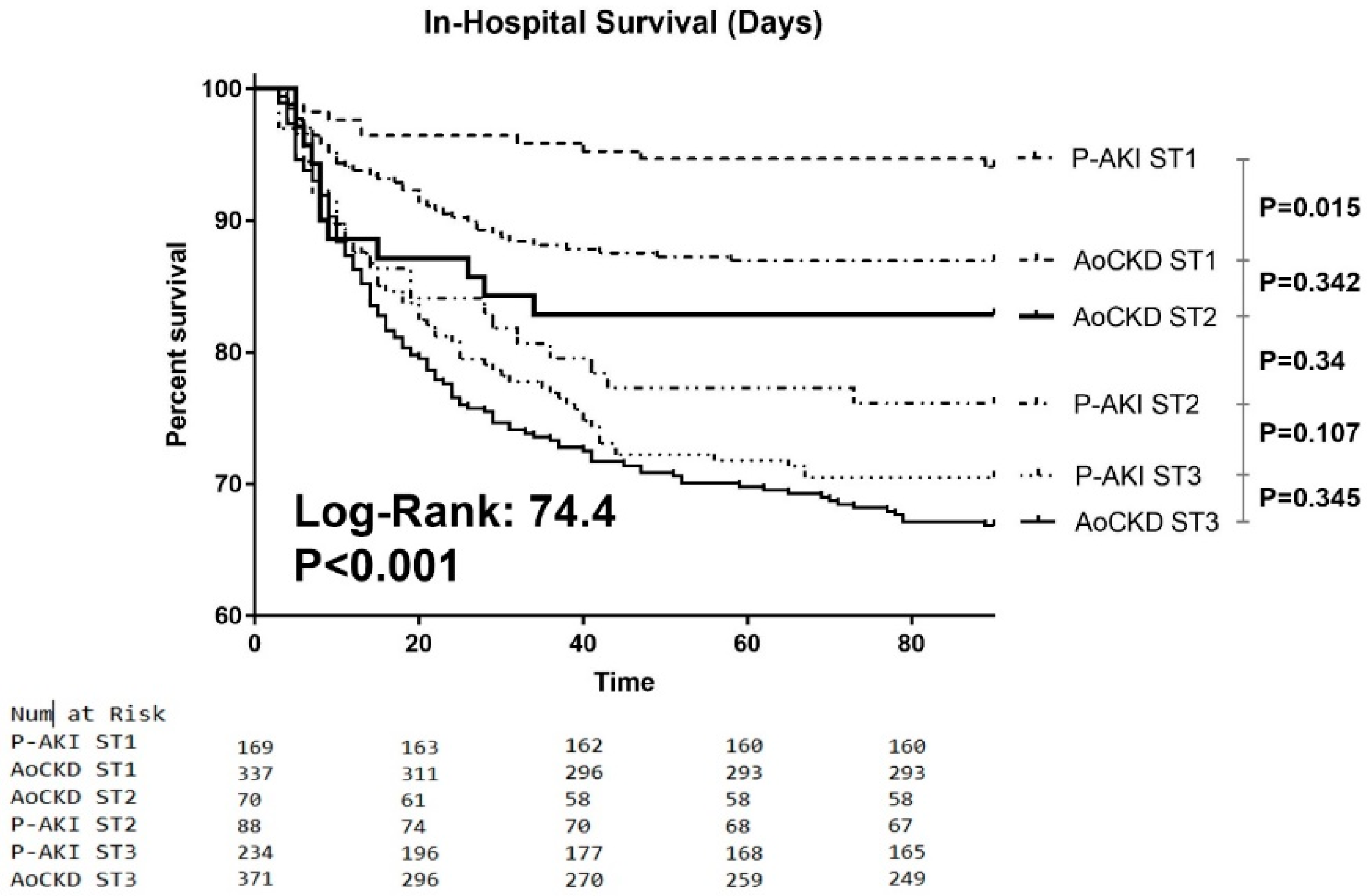
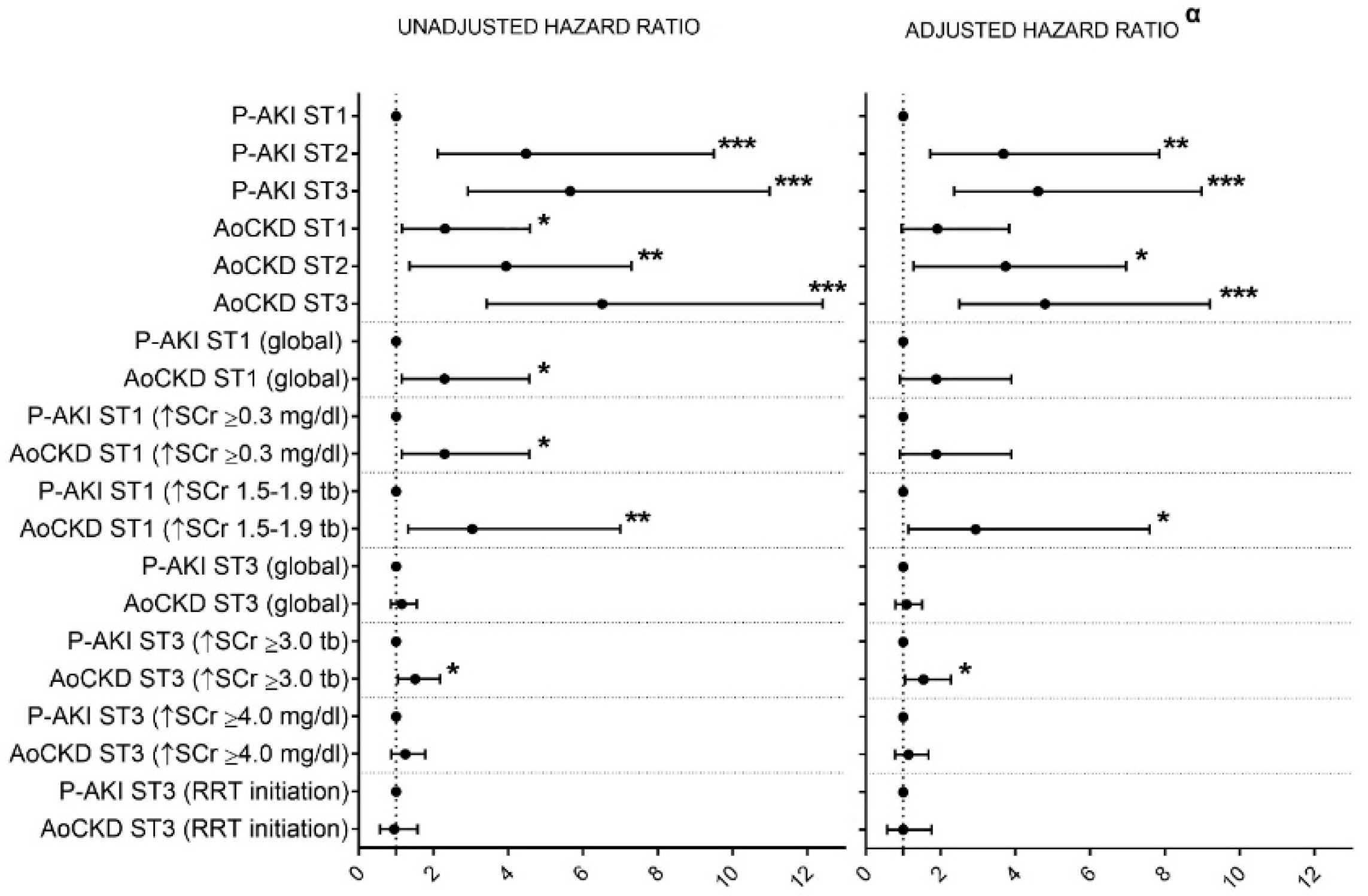
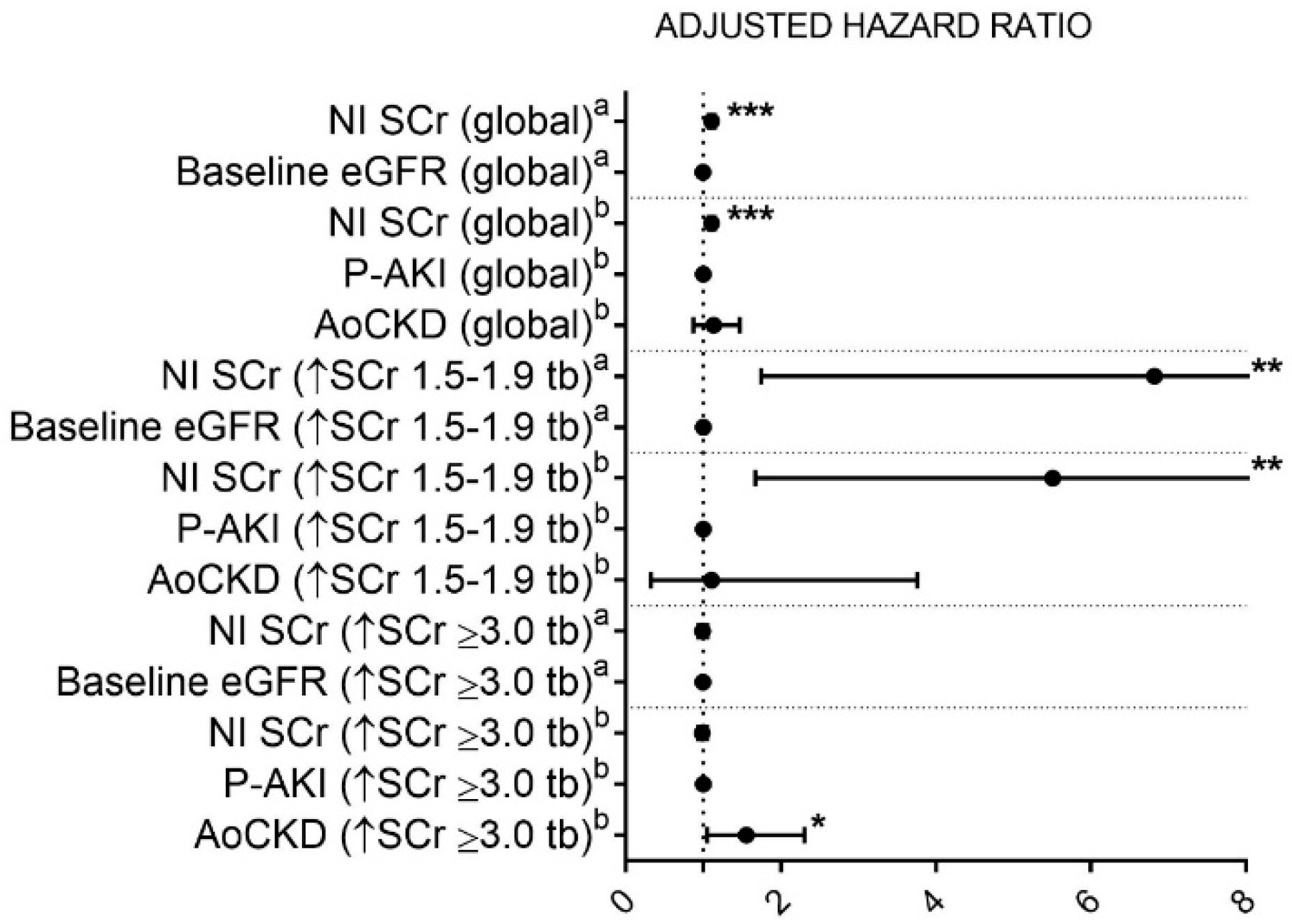
3.2. In-Hospital Mortality
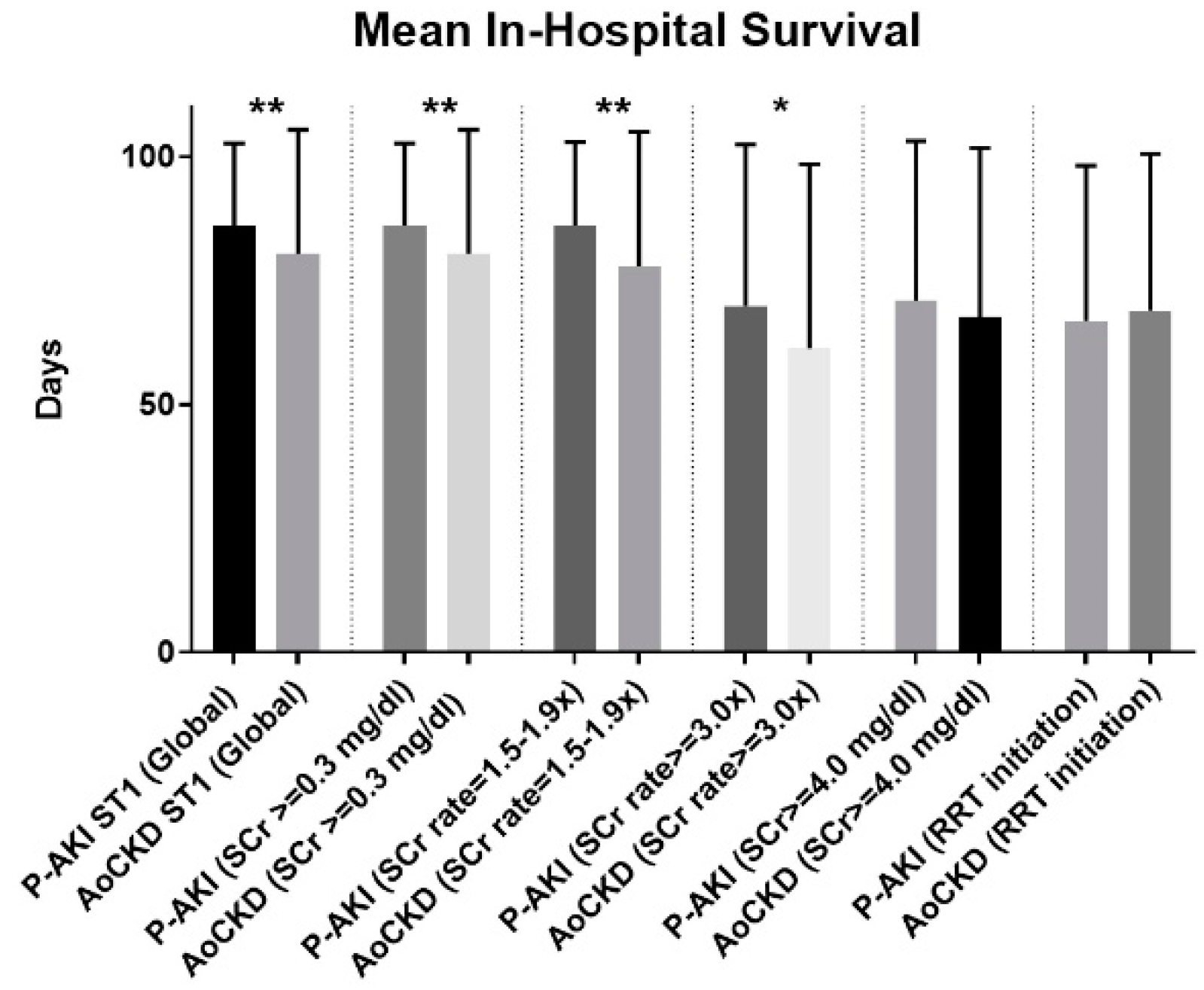
3.3. Secondary Outcomes
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Sawhney, S.; Fraser, S.D. Epidemiology of AKI: Utilizing Large Databases to Determine the Burden of AKI. Adv. Chronic. Kidney Dis. 2017, 24, 194–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kidney Disease: Improving Global Outcomes (KDIGO); Acute Kidney Injury Work Group. KDIGO clinical practice guidelines for acute kidney injury. Kidney Int. Suppl. 2012, 2, 1–138. [Google Scholar]
- Susantitaphong, P.; Cruz, D.N.; Cerda, J.; Abulfaraj, M.; Alqahtani, F.; Koulouridis, I.; Jaber, B.L.; Acute Kidney Injury Advisory Group of the American Society of Nephrology. World incidence of AKI: A meta-analysis. Clin. J. Am. Soc. Nephrol. 2013, 8, 1482–1493. [Google Scholar] [CrossRef] [PubMed]
- Lameire, N.H.; Bagga, A.; Cruz, D.; de Maeseneer, J.; Endre, Z.; Kellum, J.A.; Liu, K.D.; Mehta, R.L.; Pannu, N.; van Biesen, W.; et al. Acute kidney injury: An increasing global concern. Lancet 2013, 382, 170–179. [Google Scholar] [CrossRef]
- Collister, D.; Pannu, N.; Ye, F.; James, M.; Hemmelgarn, B.; Chui, B.; Manns, B.; Klarenbach, S. Alberta Kidney Disease Network. Health Care Costs Associated with AKI. Clin. J. Am. Soc. Nephrol. 2017, 12, 1733–1743. [Google Scholar] [CrossRef] [PubMed]
- Murugan, R.; Kellum, J.A. Acute kidney injury: What’s the prognosis? Nat. Rev. Nephrol. 2011, 7, 209–217. [Google Scholar] [CrossRef]
- Chawla, L.S.; Amdur, R.L.; Shaw, A.D.; Faselis, C.; Palant, C.E.; Kimmel, P.L. Association between AKI and long-term renal and cardiovascular outcomes in United States veterans. Clin. J. Am. Soc. Nephrol. 2014, 9, 448–456. [Google Scholar] [CrossRef]
- Omotoso, B.A.; Abdel-Rahman, E.M.; Xin, W.; Ma, JZ.; Scully, K.W.; Arogundade, F.A.; Balogun, R.A. Acute kidney injury (AKI) outcome, a predictor of long-term major adverse cardiovascular events (MACE). Clin. Nephrol. 2016, 85, 1–11. [Google Scholar] [CrossRef]
- Odutayo, A.; Wong, C.X.; Farkouh, M.; Altman, D.G.; Hopewell, S.; Emdin, C.A.; Hunn, B.H. AKI and Long-Term Risk for Cardiovascular Events and Mortality. J. Am. Soc. Nephrol. 2017, 28, 377–387. [Google Scholar] [CrossRef]
- Chawla, L.S. Disentanglement of the acute kidney injury syndrome. Curr. Opin. Crit. Care. 2012, 18, 579–584. [Google Scholar] [CrossRef]
- Palevsky, P.M. Renal replacement therapy in acute kidney injury. Adv. Chronic. Kidney Dis. 2013, 20, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Brienza, N.; Giglio, M.T.; Dalfino, L. Protocoled resuscitation and the prevention of acute kidney injury. Curr. Opin. Crit. Care. 2012, 18, 613–622. [Google Scholar] [CrossRef] [PubMed]
- Alsabbagh, M.M.; Asmar, A.; Ejaz, N.I.; Aiyer, R.K.; Kambhampati, G.; Ejaz, A.A. Update on clinical trials for the prevention of acute kidney injury in patients undergoing cardiac surgery. Am. J. Surg. 2013, 206, 86–95. [Google Scholar] [CrossRef] [PubMed]
- Chopra, T.A.; Brooks, C.H.; Okusa, M.D. Acute Kidney Injury Prevention. Contrib. Nephrol. 2016, 187, 9–23. [Google Scholar] [CrossRef] [PubMed]
- Hayes, W. Stop adding insult to injury-identifying and managing risk factors for the progression of acute kidney injury in children. Pediatr. Nephrol. 2017, 32, 2235–2243. [Google Scholar] [CrossRef] [PubMed]
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int. Suppl. 2013, 3, 1–150. [Google Scholar]
- Jha, V.; Garcia-Garcia, G.; Iseki, K.; Li, Z.; Naicker, S.; Plattner, B.; Saran, R.; Wang, A.Y.; Yang, C.W. Chronic kidney disease: Global dimension and perspectives. Lancet 2013, 382, 260–272. [Google Scholar] [CrossRef]
- Quaggin, S.E. Kindling the Kidney. N. Engl. J. Med. 2016, 374, 281–283. [Google Scholar] [CrossRef]
- Hsu, C.Y.; Ordonez, J.D.; Chertow, G.M.; Fan, D.; McCulloch, C.E.; Go, A.S. The risk of acute renal failure in patients with chronic kidney disease. Kidney Int. 2008, 74, 101–107. [Google Scholar] [CrossRef] [Green Version]
- Bedford, M.; Farmer, C.; Levin, A.; Ali, T.; Stevens, P. Acute Kidney Injury and CKD: Chicken or Egg? Am. J. Kidney Dis. 2012, 59, 485–491. [Google Scholar] [CrossRef]
- Palevsky, P.M. Chronic-on-acute kidney injury. Kidney Int. 2012, 81, 430–431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heung, M.; Steffick, D.E.; Zivin, K.; Gillespie, B.W.; Banerjee, T.; Hsu, C.Y.; Powe, N.R.; Pavkov, M.E.; Williams, D.E.; Saran, R.; et al. Centers for Disease Control and Prevention CKD Surveillance Team. Acute Kidney Injury Recovery Pattern and Subsequent Risk of CKD: An Analysis of Veterans Health Administration Data. Am. J. Kidney Dis. 2016, 67, 742–752. [Google Scholar] [CrossRef] [PubMed]
- Chawla, L.S.; Eggers, P.W.; Star, R.A.; Kimmel, P.L. Acute kidney injury and chronic kidney disease as interconnected syndromes. N. Engl. J. Med. 2014, 371, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Lim, P.; Khoo, O.T. Hypermagnesaemia in Presence of Magnesium Depletion in Acute-on-chronic Renal Failure. Br. Med. J. 1969, 1, 414–416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, L.; Wei, Q.; Liu, J.; Yi, M.; Liu, Y.; Liu, H.; Sun, L.; Peng, Y.; Liu, F.; Venkatachalam, M.A.; et al. AKI on CKD: Heightened injury, suppressed repair, and the underlying mechanisms. Kidney Int. 2017, 92, 1071–1083. [Google Scholar] [CrossRef] [PubMed]
- Zager, R.A. Progression of Acute Kidney Injury to Chronic Kidney Disease: Clinical and Experimental Insights and Queries. Nephron. Clin. Pract. 2014, 127, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Zager, R.A. ‘Biologic memory’ in response to acute kidney injury: Cytoresistance, toll-like receptor hyper-responsiveness and the onset of progressive renal disease. Nephrol. Dial. Transplant. 2013, 28, 1985–1993. [Google Scholar] [CrossRef] [PubMed]
- Goldfarb, M.; Rosenberger, C.; Abassi, Z.; Shina, A.; Zilbersat, F.; Eckardt, K.U.; Rosen, S.; Heyman, S.N.; Source, AJ. Acute-on-chronic renal failure in the rat: Functional compensation and hypoxia tolerance. Am. J. Nephrol. 2006, 26, 22–33. [Google Scholar] [CrossRef] [PubMed]
- Singh, P.; Rifkin, D.E.; Blantz, R.C. Chronic kidney disease: An inherent risk factor for acute kidney injury? Clin. J. Am. Soc. Nephrol. 2010, 5, 1690–1695. [Google Scholar] [CrossRef]
- Grams, M.E.; Sang, Y.; Ballew, S.H.; Gansevoort, R.T.; Kimm, H.; Kovesdy, C.P.; Naimark, D.; Oien, C.; Smith, D.H.; Coresh, J.; et al. A Meta-analysis of the Association of Estimated GFR, Albuminuria, Age, Race, and Sex with Acute Kidney Injury. Am. J. Kidney Dis. 2015, 66, 591–601. [Google Scholar] [CrossRef]
- Zhou, Q.; Zhao, C.; Xie, D.; Xu, D.; Bin, J.; Chen, P.; Liang, M.; Zhang, X.; Hou, F. Acute and acute-on-chronic kidney injury of patients with decompensated heart failure: Impact on outcomes. BMC Nephrol. 2012. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.Y.; Chertow, G.M.; McCulloch, C.E.; Fan, D.; Ordoñez, J.D.; Go, A.S. Nonrecovery of Kidney Function and Death after Acute on Chronic Renal Failure. Clin. J. Am. Soc. Nephrol. 2009, 4, 891–898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pannu, N.; James, M.; Hemmelgarn, B.R.; Dong, J.; Tonelli, M.; Klarenbach, S. Modification of outcomes after acute kidney injury by the presence of CKD. Am. J. Kid. Dis. 2011, 58, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Neyra, J.A.; Mescia, F.; Li, X.; Adams-Huet, B.; Yessayan, L.; Yee, J.; Toto, R.D.; Moe, O.W. Impact of acute kidney injury and CKD on adverse outcomes in critically ill septic patients. Kidney Int. Rep. 2018, 3, 1344–1353. [Google Scholar] [CrossRef] [PubMed]
- Pan, H.C.; Wu, P.C.; Wu, V.C.; Yang, Y.F.; Huang, T.M.; Shiao, C.C.; Chen, T.C.; Tarng, D.C.; Lin, J.H.; Yang, W.S.; et al. A nationwide survey of clinical characteristics, management, and outcomes of acute kidney injury (AKI)-patients with and without preexisting chronic kidney disease have different prognoses. Medicine (Baltimore) 2016, 95, e4987. [Google Scholar] [CrossRef] [PubMed]
- Khosla, N.; Soroko, S.B.; Chertow, G.M.; Himmelfarb, J.; Ikizler, T.A.; Paganini, E.; Mehta, R.L.; Program to Improve Care in Acute Renal Disease (PICARD). Preexisting chronic kidney disease: A potential for improved outcomes from acute kidney injury. Clin. J. Am. Soc. Nephrol. 2009, 4, 1914–1919. [Google Scholar] [CrossRef] [PubMed]
- Prakash, J.; Rathore, S.S.; Arora, P.; Ghosh, B.; Singh, T.B.; Gupta, T.; Mishra, R.N. Comparison of clinical characteristics of acute kidney injury versus acute-on-chronic renal failure: Our experience in a developing country. Hong Kong J. Nephrol. 2015, 17, 14e20. [Google Scholar] [CrossRef]
- Ali, T.; Khan, I.; Simpson, W.; Prescott, G.; Townend, J.; Smith, W.; Macleod, A. Incidence and outcomes in acute kidney injury: A comprehensive population-based study. J. Am. Soc. Nephrol. 2007, 18, 1292–1298. [Google Scholar] [CrossRef] [PubMed]
- Bellomo, R.; Ronco, C.; Kellum, J.A.; Mehta, R.L.; Palevsky, P.; ADQI Workgroup. Acute renal failure—definition, outcome measures, animal models, fluid therapy and information technology needs: The Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit. Care 2004, 8, R204–R212. [Google Scholar] [CrossRef]
- Ronco, C.; Levin, A.; Warnock, D.G.; Mehta, R.; Kellum, J.A.; Shah, S.; Molitoris, B.A.; AKIN Working Group. Improving outcomes from acute kidney injury (AKI): Report on an initiative. Int. J. Artif. Organs. 2007, 30, 373–376. [Google Scholar] [CrossRef]
- Levey, A.S.; Bosch, J.P.; Lewis, J.B.; Greene, T.; Rogers, N.; Roth, D. A more accurate method to estimate glomerular filtration rate from serum creatinine: A new prediction equation. Modification of Diet in Renal Disease Study Group. Ann. Intern. Med. 1999, 130, 461–470. [Google Scholar] [CrossRef] [PubMed]
- Siew, E.D.; Ikizler, T.A.; Matheny, M.E.; Shi, Y.; Schildcrout, J.S.; Danciu, I.; Dwyer, J.P.; Srichai, M.; Hung, A.M.; Smith, J.P.; et al. Estimating Baseline Kidney Function in Hospitalized Patients with Impaired Kidney Function. Clin. J. Am. Soc. Nephrol. 2012, 7, 712–719. [Google Scholar] [CrossRef] [PubMed]
- Der Mesropian, P.J.; Kalamaras, J.S.; Eisele, G.; Phelps, K.R.; Asif, A.; Mathew, R.O. Long-term outcomes of community-acquired versus hospital-acquired acute kidney injury: A retrospective analysis. Clin. Nephrol. 2014, 81, 81–174. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic. Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Hatakeyama, Y.; Horino, T.; Nagata, K.; Matsumoto, T.; Terada, Y.; Okuhara, Y. Transition from acute kidney injury to chronic kidney disease: A single centre cohort study. Clin. Exp. Nephrol. 2018, 22, 1281–1293. [Google Scholar] [CrossRef] [PubMed]
- Machado, M.N.; Nakazone, M.A.; Maia, L.N. Acute kidney injury based on KDIGO (Kidney Disease Improving Global Outcomes) criteria in patients with elevated baseline serum creatinine undergoing cardiac surgery. Rev. Bras. Cir. Cardiovasc. 2014, 29, 299–307. [Google Scholar] [CrossRef]
- Sawhney, S.; Marks, A.; Fluck, N.; Levin, A.; Prescott, G.; Black, C. Intermediate and long-term outcomes of survivors of acute kidney injury episodes: A large population-based cohort study. Am. J. Kid. Dis. 2017, 69, 18–28. [Google Scholar] [CrossRef] [PubMed]
- Chao, C.T.; Wu, VC.; Lai, C.F.; Shiao, C.C.; Huang, T.M.; Wu, P.C.; Tsai, I.J.; Hou, C.C.; Wang, W.J.; Tsai, H.B.; et al. Advanced age affects the outcome-predictive power of RIFLE classification in geriatric patients with acute kidney injury. Kidney Int. 2012, 82, 920–927. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Stage | Serum Creatinine | Urine Output |
|---|---|---|
| 1 | 1.5–1.9 times baseline | <0.5 mL/kg/h for 6–12 h |
| OR | ||
| ≥0.3 mg/dL increase | ||
| 2 | 2.0–2.9 times baseline | <0.5 mL/kg/h for ≥12 h |
| 3 | 3.0 times baseline | <0.3 mL/kg/h for ≥24 h |
| OR | OR | |
| Increase in serum creatinine to ≥4.0 mg/dL | Anuria for ≥12 h to ≥4.0 mg/dL | |
| OR | ||
| Initiation of renal replacement therapy | ||
| OR | ||
| In patients <18 years. Decrease in eGFR to <35 mL/min/1.73 m2 |
| ALL | P-AKI | AoCKD | p Value2 | |||||
|---|---|---|---|---|---|---|---|---|
| AoCKD | p Value1 | |||||||
| CKD-3A | CKD-3B | CKD-4 | ||||||
| N | 1269 | 491 | 778 | 221 | 282 | 275 | ||
| Male sex—No. (%) | 883 (70) | 339 (69) | 544 (70) | 0.739 | 162 (73) | 198 (70) | 184 (67) | 0.476 |
| Age (years)—Median (IQR) | 75 (65–81) | 71 (61–79) | 77 (69–83) | <0.001 | 76 (69–82) | 78 (70–83) | 77 (67–83) | <0.001 |
| HTN—No. (%) | 1125 (89) | 395 (80) | 730 (94) | <0.001 | 206 (93) | 268 (95) | 256 (93) | <0.001 |
| DM—No. (%) | 536 (42) | 158 (32) | 378 (49) | <0.001 | 96 (43) | 145 (51) | 137 (50) | <0.001 |
| CAD—No. (%) | 385 (30) | 107 (22) | 278 (36) | <0.001 | 73 (33) | 105 (37) | 100 (36) | <0.001 |
| CHF—No. (%) | 491 (39) | 140 (29) | 351 (45) | <0.001 | 94 (43) | 146 (52) | 111 (40) | <0.001 |
| PAD—No. (%) | 392 (31) | 108 (22) | 284 (37) | <0.001 | 89 (40) | 112 (40) | 83 (30) | <0.001 |
| CHD—No. (%) | 231 (18) | 37 (8) | 36 (5) | 0.03 | 11 (5) | 14 (5) | 11 (4) | 0.171 |
| Charlson Comorbidity Index (SD) | 4 (3–6) | 4 (2–6) | 5 (3–6) | <0.001 | 4 (3–6) | 5 (3–6) | 6 (4–7) | <0.001 |
| Unit of Admission | ||||||||
| Medical Unit—No. (%) | 808 (64) | 180 (37) | 281 (36) | 0.845 | 91 (41) | 110 (39) | 80 (29) | 0.025 |
| ICU—No. (%) | 241 (19) | 117 (24) | 124 (16) | <0.001 | 44 (20) | 42 (15) | 38 (14) | 0.001 |
| AKI Type | ||||||||
| Community Acquired—No. (%) | 870 (69) | 160 (33) | 239 (31) | 0.485 | 74 (34) | 90 (32) | 75 (27) | 0.396 |
| KDIGO-2012 AKI Stage 1 (global)—No. (%) | 506 (40) | 169 (34) | 337 (43) | 0.002 | 115 (53) | 145 (51) | 77 (28) | <0.001 |
| ≥0.3 mg/dL | 506 (40) | 169 (34) | 337 (43) | 0.002 | 115 (53) | 145 (51) | 77 (28) | <0.001 |
| SCr 1.5–1.9× | 264 (21) | 115 (23) | 149 (19) | 0.068 | 59 (27) | 70 (25) | 20 (7) | <0.001 |
| KDIGO-2012 AKI Stage 2 (SCr 2.0–2.9×)—No. (%) | 158 (13) | 88 (18) | 70 (9) | <0.001 | 42 (19) | 27 (10) | 1 (0.4) | <0.001 |
| KDIGO-2012 AKI Stage 3 (global)—No. (%) | 605 (48) | 234 (48) | 371 (48) | 0.992 | 60 (28) | 112 (39) | 199 (72) | <0.001 |
| SCr ≥ 3.0× | 354 (28) | 229 (47) | 125 (16) | <0.001 | 46 (21) | 54 (19) | 25 (9) | <0.001 |
| SCr ≥ 4.0 mg/dL | 503 (40) | 150 (31) | 353 (45) | <0.001 | 48 (22) | 108 (38) | 197 (71) | <0.001 |
| Initiation RRT | 167 (13) | 62 (13) | 105 (14) | 0.656 | 16 (7) | 24 (9) | 65 (24) | <0.001 |
| Baseline SCr (mg/dL) | 1.4 (1–2) | 0.9 (0.7–1.1) | 1.9 (1.5–2.5) | <0.001 | 1.4 (1.2–1.5) | 1.8 (1.6–2) | 2.7 (2.4–3.2) | <0.001 |
| Peak SCr (mg/dL) | 3.4 (2.2–5.2) | 2.5 (1.5–4.5) | 3.7 (2.6–5.5) | <0.001 | 2.6 (2–3.8) | 3.4 (2.6–4.9) | 5 (3.9–6.7) | <0.001 |
| SCr Net Increase (mg/dL) | 1.6 (0.7–3.3) | 1.6 (0.6–3.6) | 1.7 (0.9–3) | 0.232 | 1.2 (0.7–2.4) | 1.6 (0.8–3.2) | 2.2 (1.2–3.5) | <0.001 |
| Discharge SCr (mg/dL) | 1.9 (1.3–2.9) | 1.2 (0.9–1.7) | 2.4 (1.7–3.5) | <0.001 | 1.7 (1.4–2.2) | 2.3 (1.8–2.8) | 3.6 (2.7–4.9) | <0.001 |
| ARF | AoCKD | p Value | |
|---|---|---|---|
| N | 491 | 778 | |
| Primary Endpoint | |||
| In-Hospital Mortality—No. (%) | 100 (20.4) | 179 (23) | 0.15 |
| Secondary Endpoints | |||
| Initiation of RRT—No. (%) | 62 (12.6) | 105 (13.5) | 0.36 |
| Length of Hospital Stay (days) | 12 (7–25) | 12 (7–21) | 0.08 |
| Time to Nephrology Consultation (days) | 4 (1–8) | 3 (1–6) | <0.001 |
| Dialysis Dependence at Discharge—No. (%) | 7 (1.4) | 40 (5.1) | <0.001 |
| In-Hospital Mortality | ARF | AoCKD | p Value |
| KDIGO-2012 AKI Stage 1 (global) | 10 (5.9) | 44 (13.1) | 0.014 |
| ≥0.3 mg/dL | 10 (5.9) | 44 (13.1) | 0.014 |
| SCr 1.5–1.9× | 7 (6.1) | 26 (17.4) | 0.006 |
| KDIGO-2012 AKI Stage 2 | 21 (23.9) | 12 (17.1) | 0.302 |
| KDIGO-2012 AKI Stage 3 (global) | 69 (29.5) | 123 (33.2) | 0.345 |
| SCr 3.0× | 67 (29.3) | 50 (40) | 0.04 |
| SCr ≥ 4.0 mg/dL | 41 (27.3) | 116 (32.9) | 0.221 |
| Initiation RRT | 24 (38.7) | 39 (37.1) | 0.84 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Acosta-Ochoa, I.; Bustamante-Munguira, J.; Mendiluce-Herrero, A.; Bustamante-Bustamante, J.; Coca-Rojo, A. Impact on Outcomes across KDIGO-2012 AKI Criteria According to Baseline Renal Function. J. Clin. Med. 2019, 8, 1323. https://doi.org/10.3390/jcm8091323
Acosta-Ochoa I, Bustamante-Munguira J, Mendiluce-Herrero A, Bustamante-Bustamante J, Coca-Rojo A. Impact on Outcomes across KDIGO-2012 AKI Criteria According to Baseline Renal Function. Journal of Clinical Medicine. 2019; 8(9):1323. https://doi.org/10.3390/jcm8091323
Chicago/Turabian StyleAcosta-Ochoa, Isabel, Juan Bustamante-Munguira, Alicia Mendiluce-Herrero, Jesús Bustamante-Bustamante, and Armando Coca-Rojo. 2019. "Impact on Outcomes across KDIGO-2012 AKI Criteria According to Baseline Renal Function" Journal of Clinical Medicine 8, no. 9: 1323. https://doi.org/10.3390/jcm8091323