Surgery of Inverted Papilloma of the Maxillary Sinus via Translacrimal Approach—Long-Term Outcome and Literature Review

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
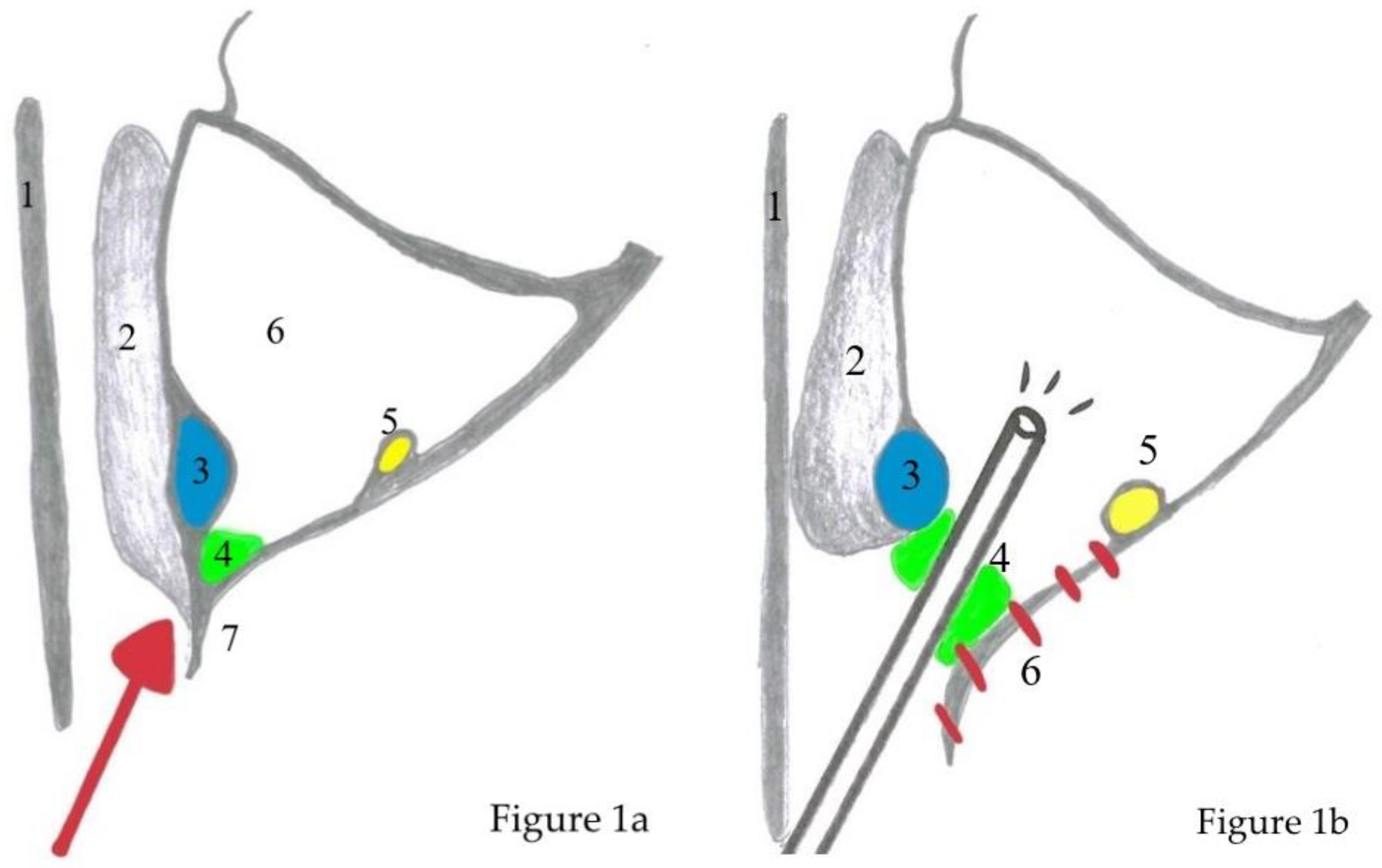
Surgical Technique
- debulking of the exophytic tumor inside the nasal cavity;
- uncinectomy, middle meatal antrostomy type III, with or without opening of the bulla ethmoidalis and an anterior ethmoidectomy;
- entry of the maxillary sinus via the prelacrimal approach with complete exposure of the IP and its attachment;
- creation of a medially based mucosal flap from the nasal floor towards the maxillary sinus;
- subperiosteal resection of the IP and drilling of the bone at the attachment site until the bone shows a clear white color and healthy appearance. In some cases, some parts of the maxillary wall need to be completely resected to the level of the periosteum of the hard palate and the pterygopalatine fossa;
- resection of the nasolacrimal duct if necessary due to tumor invasion;
- performing a medial maxillectomy; and,
- repositioning the mucosal flap and the inferior turbinate, which is sutured to the mucosa of the lateral nasal wall with one or two stitches.
3. Results
3.1. Patient Population
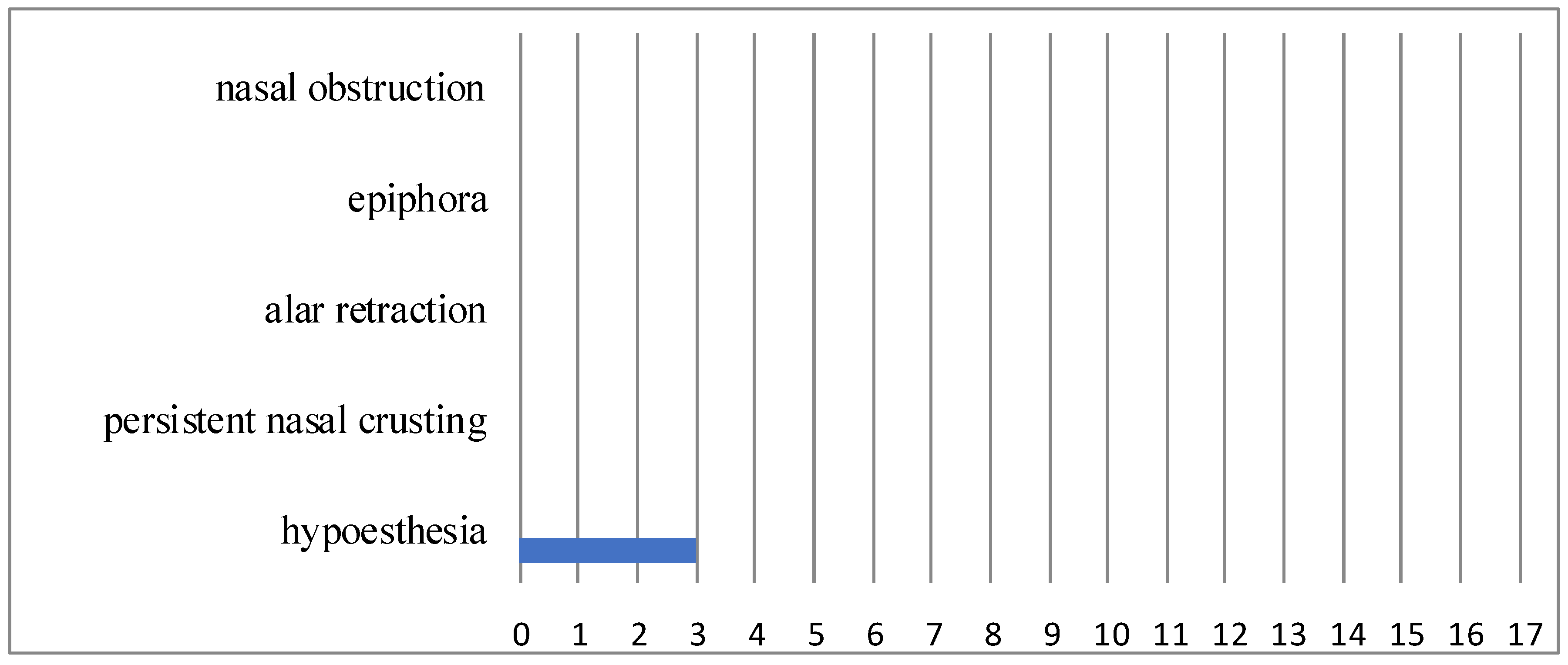
3.2. Functional Outcome
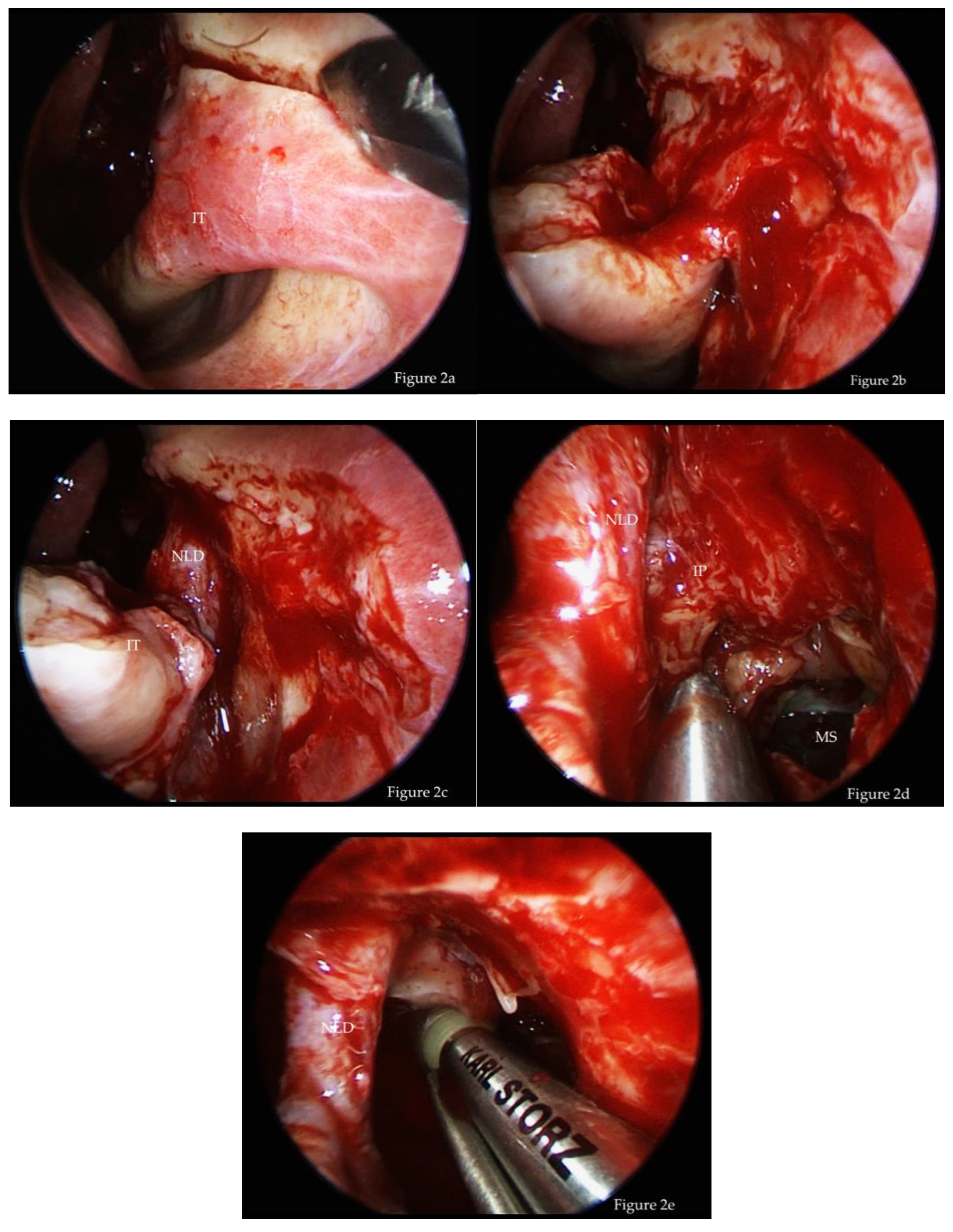
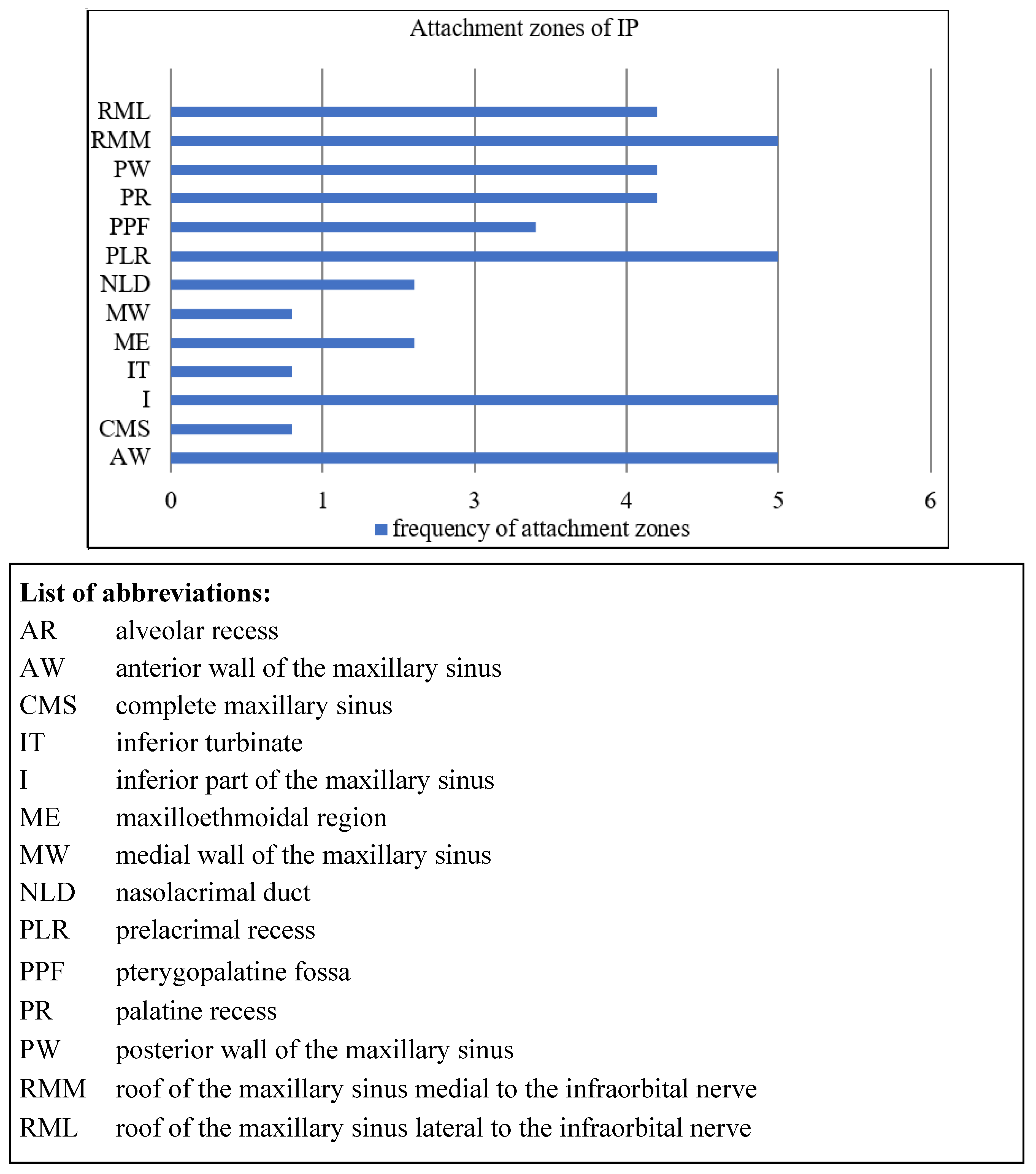
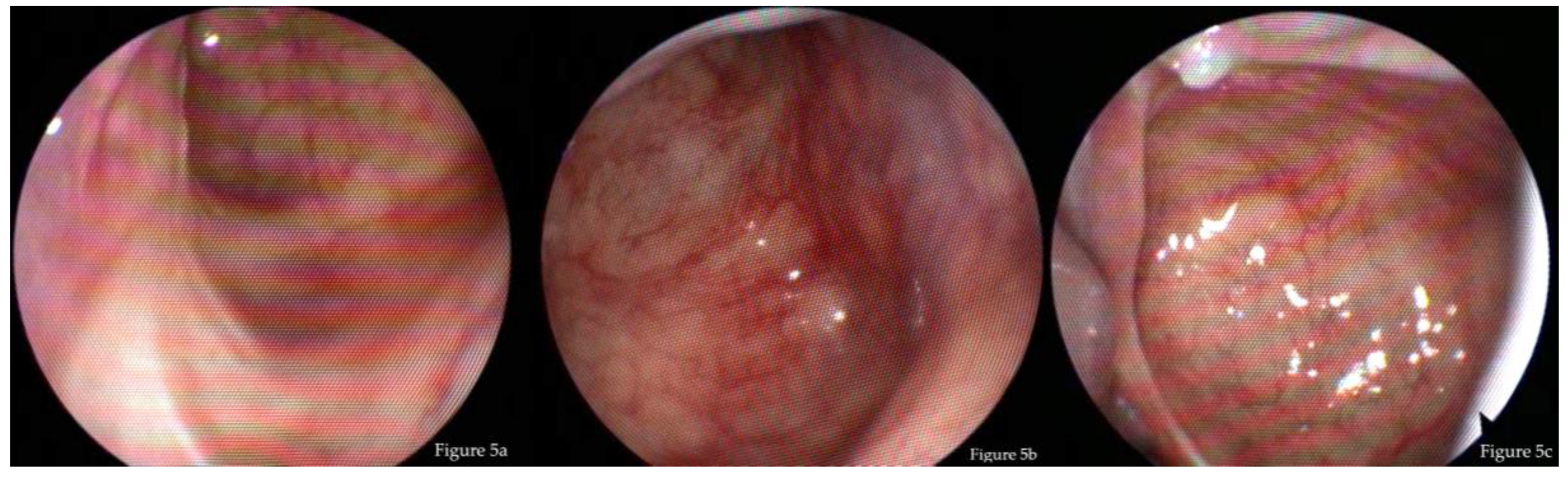
3.3. Endoscopic Findings
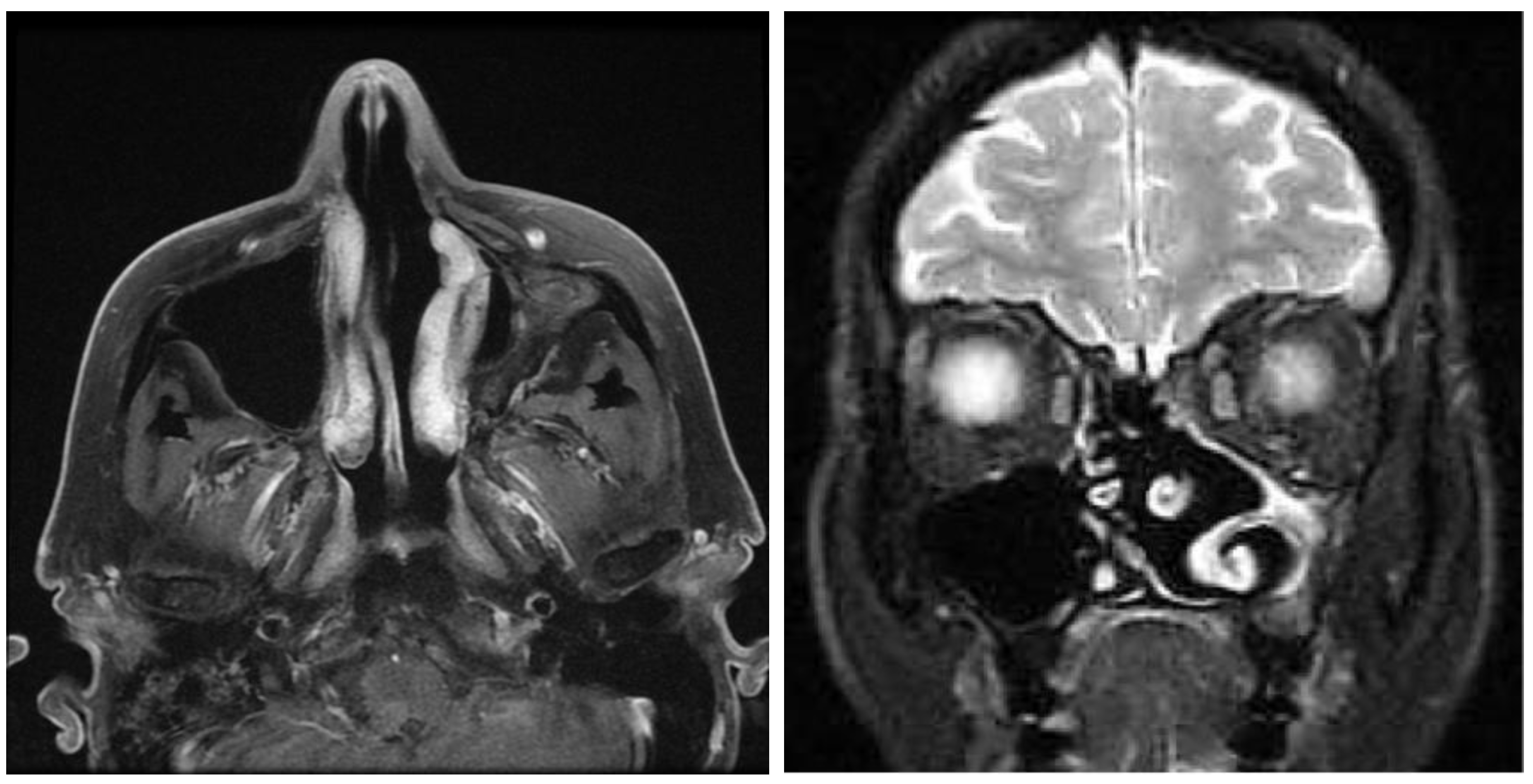
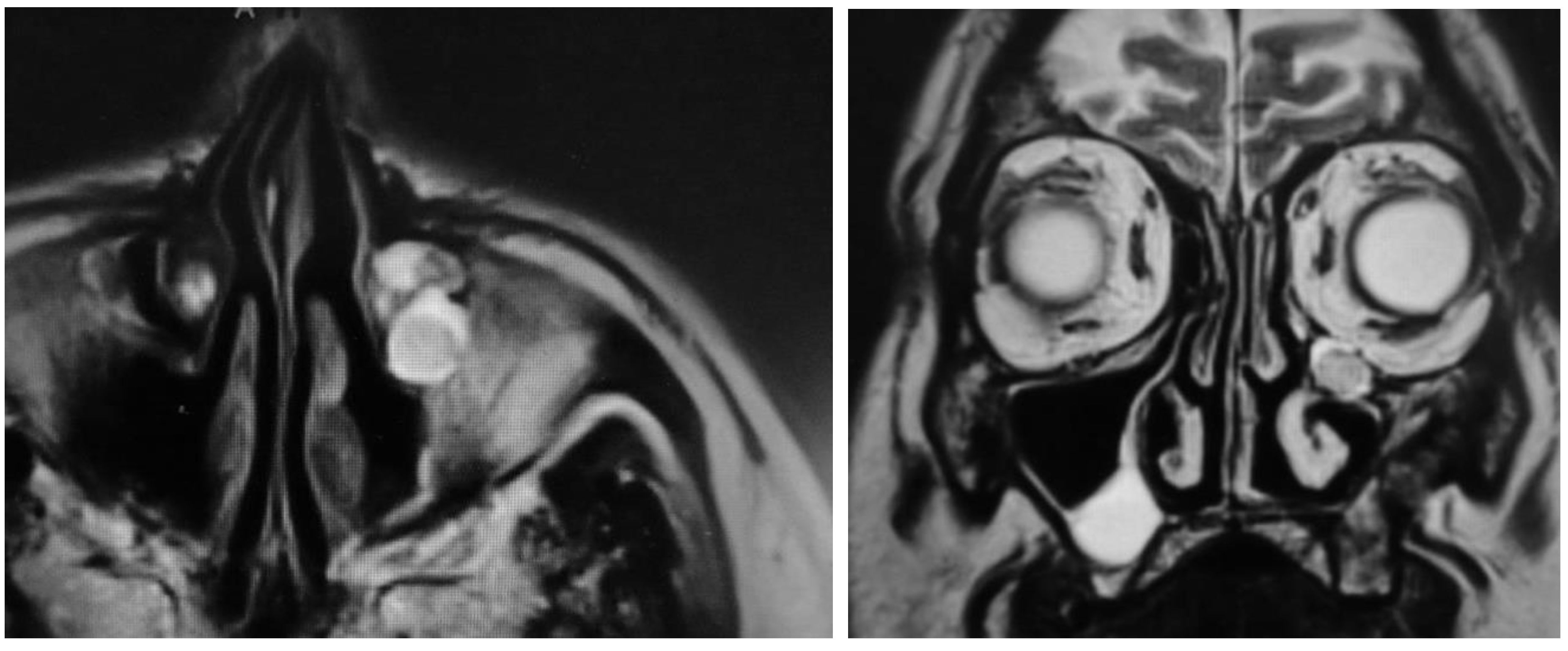
3.4. MRI
4. Discussion
4.1. Surgical Technique and Recurrence
4.2. Postoperative Morbidity
5. Limitations
6. Conclusions
Author Contributions
Conflicts of Interest
References
- Anari, S.; Carrie, S. Sinonasal inverted papilloma: Narrative review. J. Laryngol. Otol. 2010, 124, 705–715. [Google Scholar] [CrossRef] [PubMed]
- Attlmayr, B.; Derbyshire, S.G.; Kasbekar, A.V.; Swift, A.C. Management of inverted papilloma: Review. J. Laryngol. Otol. 2017, 131, 284–289. [Google Scholar] [CrossRef] [PubMed]
- Turfe, Z.; Ahmad, A.; Peterson, E.I.; Craig, J.R. Odontogenic sinusitis is a common cause of unilateral sinus disease with maxillary sinus opacification. Int. Forum Allergy Rhinol. 2019. [Google Scholar] [CrossRef]
- Eckhoff, A.; Cox, D.; Luk, L.; Maidman, S.; Wise, S.K.; DelGaudio, J.M. Unilateral versus bilateral sinonasal disease: Considerations in differential diagnosis and workup. Laryngoscope 2019. [Google Scholar] [CrossRef] [PubMed]
- Lawson, W.; Kaufman, M.R.; Biller, H.F. Treatment outcomes in the management of inverted papilloma: An analysis of 160 cases. Laryngoscope 2003, 113, 1548–1556. [Google Scholar] [CrossRef] [PubMed]
- Mirza, S.; Bradley, P.J.; Acharya, A.; Stacey, M.; Jones, N.S. Sinonasal inverted papillomas: Recurrence, and synchronous and metachronous malignancy. J. Laryngol. Otol. 2007, 121, 857–864. [Google Scholar] [CrossRef] [PubMed]
- Giotakis, E.; Eleftheriadou, A.; Ferekidou, E.; Kandiloros, D.; Manolopoulos, L.; Yiotakis, I. Clinical outcomes of sinonasal inverted papilloma surgery. A retrospective study of 67 cases. B-ENT 2010, 6, 111–116. [Google Scholar] [PubMed]
- Lund, V.J.; Howard, D.; Wei, W.I. Tumors of the Nose, Sinuses and Nasopharynx; Thieme: Stuttgart, Germany; New York, NY, USA, 2014. [Google Scholar]
- Lund, V.J.; Stammberger, H.; Nicolai, P.; Castelnuovo, P.; Beal, T.; Beham, A.; Bernal-Sprekelsen, M.; Braun, H.; Cappabianca, P.; Carrau, R.; et al. European position paper on endoscopic management of tumours of the nose, paranasal sinuses and skull base. Rhinol. Suppl. 2010, 22, 1–143. [Google Scholar]
- Weber, R.K.; Hosemann, W. Comprehensive review on endonasal endoscopic sinus surgery. GMS Curr. Top. Otorhinolaryngol. Head Neck Surg. 2015, 14, Doc08. [Google Scholar] [CrossRef]
- Krouse, J.H. Endoscopic treatment of inverted papilloma: Safety and efficacy. Am. J. Otolaryngol. 2001, 22, 87–99. [Google Scholar] [CrossRef]
- Carta, F.; Blancal, J.P.; Verillaud, B.; Tran, H.; Sauvaget, E.; Kania, R.; Herman, P. Surgical management of inverted papilloma: Approaching a new standard for surgery. Head Neck 2013, 35, 1415–1420. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Han, D.; Zhang, L. Modified endoscopic maxillary medial sinusotomy for sinonasal inverted papilloma with attachment to the anterior medial wall of maxillary sinus. ORL J. Otorhinolaryngol. Relat. Spec. 2012, 74, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Pasquini, E.; Sciarretta, V.; Farneti, G.; Modugno, G.C.; Ceroni, A.R. Inverted papilloma: Report of 89 cases. Am. J. Otolaryngol. 2004, 25, 178–185. [Google Scholar] [CrossRef] [PubMed]
- Eloy, P.; Mardyla, N.; Bertrand, B.; Rombaux, P. Endoscopic endonasal medial maxillectomy: Case series. Indian J. Otolaryngol. Head Neck Surg. 2010, 62, 252–257. [Google Scholar] [CrossRef]
- Healy, D.Y., Jr.; Chhabra, N.; Metson, R.; Holbrook, E.H.; Gray, S.T. Surgical risk factors for recurrence of inverted papilloma. Laryngoscope 2016, 126, 796–801. [Google Scholar] [CrossRef]
- Landsberg, R.; Cavel, O.; Segev, Y.; Khafif, A.; Fliss, D.M. Attachment-oriented endoscopic surgical strategy for sinonasal inverted papilloma. Am. J. Rhinol. 2008, 22, 629–634. [Google Scholar] [CrossRef]
- Lombardi, D.; Tomenzoli, D.; Butta, L.; Bizzoni, A.; Farina, D.; Sberze, F.; Karligkiotis, A.; Castelnuovo, P.; Nicolai, P. Limitations and complications of endoscopic surgery for treatment for sinonasal inverted papilloma: A reassessment after 212 cases. Head Neck 2011, 33, 1154–1161. [Google Scholar] [CrossRef]
- Lee, T.J.; Huang, S.F.; Huang, C.C. Tailored endoscopic surgery for the treatment of sinonasal inverted papilloma. Head Neck 2004, 26, 145–153. [Google Scholar] [CrossRef]
- Minovi, A.; Kollert, M.; Draf, W.; Bockmuhl, U. [Endonasal micro-endoscopic resection of sinonasal inverted papilloma]. Laryngorhinootologie 2006, 85, 421–425. [Google Scholar] [CrossRef]
- Pagella, F.; Pusateri, A.; Giourgos, G.; Tinelli, C.; Matti, E. Evolution in the treatment of sinonasal inverted papilloma: Pedicle-oriented endoscopic surgery. Am. J. Rhinol. Allergy 2014, 28, 75–81. [Google Scholar] [CrossRef]
- Kim, J.S.; Kwon, S.H. Recurrence of sinonasal inverted papilloma following surgical approach: A meta-analysis. Laryngoscope 2017, 127, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Lawson, W.; Patel, Z.M. The evolution of management for inverted papilloma: An analysis of 200 cases. Otolaryngol. Head Neck Surg. 2009, 140, 330–335. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Li, X.; Shi, L.; Cai, X.; Ye, P.; Feng, X.; Pan, X. Endoscopic surgery for maxillary sinus inverted papilloma. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi 2014, 49, 721–725. [Google Scholar] [PubMed]
- Konstantinidis, I.; Constantinidis, J. Medial maxillectomy in recalcitrant sinusitis: When, why and how? Curr. Opin. Otolaryngol. Head Neck Surg. 2014, 22, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Robey, A.; O’Brien, E.K.; Leopold, D.A. Assessing current technical limitations in the small-hole endoscopic approach to the maxillary sinus. Am. J. Rhinol. Allergy 2010, 24, 396–401. [Google Scholar] [CrossRef]
- Donmez, D.; Giotakis, E.; Hosemann, W.G.; Kuhnel, T.S.; Hirt, B.; Weber, R.K. Posterior translacrimal approach to the maxillary sinus. J. Laryngol. Otol. 2017, 131, 871–879. [Google Scholar] [CrossRef]
- Hosemann, W.; Scotti, O.; Bentzien, S. Evaluation of telescopes and forceps for endoscopic transnasal surgery on the maxillary sinus. Am. J. Rhinol. 2003, 17, 311–316. [Google Scholar] [CrossRef]
- Albu, S.; Baciut, M.; Opincariu, I.; Rotaru, H.; Dinu, C. The canine fossa puncture technique in chronic odontogenic maxillary sinusitis. Am. J. Rhinol. Allergy 2011, 25, 358–362. [Google Scholar] [CrossRef]
- Albu, S.; Gocea, A.; Necula, S. Simultaneous inferior and middle meatus antrostomies in the treatment of the severely diseased maxillary sinus. Am. J. Rhinol. Allergy 2011, 25, e80–e85. [Google Scholar] [CrossRef]
- Anand, V.; Santosh, S.; Aishwarya, A. Canine fossa approaches in endoscopic sinus surgery-our experience. Indian J. Otolaryngol. Head Neck Surg. 2008, 60, 214–217. [Google Scholar] [CrossRef]
- Byun, J.Y.; Lee, J.Y.; Baek, B.J. Weakness of buccal branch of facial nerve after canine fossa puncture. J. Laryngol. Otol. 2011, 125, 214–216. [Google Scholar] [CrossRef] [PubMed]
- Byun, J.Y.; Lee, J.Y. Canine fossa puncture for severe maxillary disease in unilateral chronic sinusitis with nasal polyp. Laryngoscope 2013, 123, E79–E84. [Google Scholar] [CrossRef] [PubMed]
- Bernal-Sprekelsen, M.; Kalweit, H.; Welkoborsky, H.J. Discomforts after endoscopy of the maxillary sinus via canine fossa. Rhinology 1991, 29, 69–75. [Google Scholar] [PubMed]
- Lee, J.T.; Suh, J.D.; Carrau, R.L.; Chu, M.W.; Chiu, A.G. Endoscopic Denker’s approach for resection of lesions involving the anteroinferior maxillary sinus and infratemporal fossa. Laryngoscope 2017, 127, 556–560. [Google Scholar] [CrossRef]
- Masterson, L.; Al Gargaz, W.; Bath, A.P. Endoscopic Caldwell-Luc technique. J. Laryngol. Otol. 2010, 124, 663–665. [Google Scholar] [CrossRef]
- Robinson, S.R.; Baird, R.; Le, T.; Wormald, P.J. The incidence of complications after canine fossa puncture performed during endoscopic sinus surgery. Am. J. Rhinol. 2005, 19, 203–206. [Google Scholar] [CrossRef]
- Tomenzoli, D.; Castelnuovo, P.; Pagella, F.; Berlucchi, M.; Pianta, L.; Delu, G.; Maroldi, R.; Nicolai, P. Different endoscopic surgical strategies in the management of inverted papilloma of the sinonasal tract: Experience with 47 patients. Laryngoscope 2004, 114, 193–200. [Google Scholar] [CrossRef]
- Singhal, D.; Douglas, R.; Robinson, S.; Wormald, P.J. The incidence of complications using new landmarks and a modified technique of canine fossa puncture. Am. J. Rhinol. 2007, 21, 316–319. [Google Scholar] [CrossRef]
- Erbek, S.S.; Koycu, A.; Buyuklu, F. Endoscopic modified medial maxillectomy for treatment of inverted papilloma originating from the maxillary sinus. J. Craniofac. Surg. 2015, 26, e244–e246. [Google Scholar] [CrossRef]
- Weber, R.K.; Werner, J.A.; Hildenbrand, T. Endonasal endoscopic medial maxillectomy with preservation of the inferior turbinate. Am. J. Rhinol. Allergy 2010, 24, 132–135. [Google Scholar] [CrossRef]
- Zhou, B.; Han, D.M.; Cui, S.J.; Huang, Q.; Wang, C.S. Intranasal endoscopic prelacrimal recess approach to maxillary sinus. Chin. Med. J. (Engl.) 2013, 126, 1276–1280. [Google Scholar] [PubMed]
- Zhou, B.; Han, D.M.; Cui, S.J.; Huang, Q.; Wei, Y.X.; Liu, H.C.; Liu, M. [Endoscopic nasal lateral wall dissection approach to maxillary sinus]. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi 2007, 42, 743–748. [Google Scholar] [PubMed]
- Suzuki, M.; Nakamura, Y.; Nakayama, M.; Inagaki, A.; Murakami, S.; Takemura, K.; Yokota, M. Modified transnasal endoscopic medial maxillectomy with medial shift of preserved inferior turbinate and nasolacrimal duct. Laryngoscope 2011, 121, 2399–2401. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, M.; Nakamura, Y.; Yokota, M.; Ozaki, S.; Murakami, S. Modified transnasal endoscopic medial maxillectomy through prelacrimal duct approach. Laryngoscope 2017, 127, 2205–2209. [Google Scholar] [CrossRef]
- Rutherford, K.D.; Brown, S.M. Endoscopic resection of maxillary sinus inverted papillomas with inferior turbinate preservation. Otolaryngol. Head Neck Surg. 2010, 142, 760–762. [Google Scholar] [CrossRef]
- Nakayama, T.; Asaka, D.; Okushi, T.; Yoshikawa, M.; Moriyama, H.; Otori, N. Endoscopic medial maxillectomy with preservation of inferior turbinate and nasolacrimal duct. Am. J. Rhinol. Allergy 2012, 26, 405–408. [Google Scholar] [CrossRef]
- Nakamaru, Y.; Furuta, Y.; Takagi, D.; Oridate, N.; Fukuda, S. Preservation of the nasolacrimal duct during endoscopic medial maxillectomy for sinonasal inverted papilloma. Rhinology 2010, 48, 452–456. [Google Scholar] [CrossRef]
- Pagella, F.; Pusateri, A.; Matti, E.; Avato, I.; Zaccari, D.; Emanuelli, E.; Volo, T.; Cazzador, D.; Citraro, L.; Ricci, G.; et al. “TuNa-saving” endoscopic medial maxillectomy: A surgical technique for maxillary inverted papilloma. Eur. Arch. Otorhinolaryngol. 2017, 274, 2785–2791. [Google Scholar] [CrossRef]
- Wormald, P.J.; Ooi, E.; van Hasselt, C.A.; Nair, S. Endoscopic removal of sinonasal inverted papilloma including endoscopic medial maxillectomy. Laryngoscope 2003, 113, 867–873. [Google Scholar] [CrossRef]
- Wormald, P.J. Endoscopic Sinus Surgery: Anatomy, Three-Dimensional Reconstruction and Surgical Technique, 3rd ed.; Thieme: New York, NY, USA, 2013. [Google Scholar]
- Simmen, D.J.N. Manual of Endoscopic Sinus and Skull Base Surgery, 2nd ed.; Thieme: Stuttgart, Germany, 2013. [Google Scholar]
- Morrissey, D.K.; Wormald, P.J.; Psaltis, A.J. Prelacrimal approach to the maxillary sinus. Int. Forum Allergy Rhinol. 2016, 6, 214–218. [Google Scholar] [CrossRef]
- Gras-Cabrerizo, J.R.; Massegur-Solench, H.; Pujol-Olmo, A.; Montserrat-Gili, J.R.; Adema-Alcover, J.M.; Zarraonandia-Andraca, I. Endoscopic medial maxillectomy with preservation of inferior turbinate: How do we do it? Eur. Arch. Otorhinolaryngol. 2011, 268, 389–392. [Google Scholar] [CrossRef] [PubMed]
- Krouse, J.H. Development of a staging system for inverted papilloma. Laryngoscope 2000, 110, 965–968. [Google Scholar] [CrossRef] [PubMed]
- Yousuf, K.; Wright, E.D. Site of attachment of inverted papilloma predicted by CT findings of osteitis. Am. J. Rhinol. 2007, 21, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Sham, C.L.; King, A.D.; van Hasselt, A.; Tong, M.C. The roles and limitations of computed tomography in the preoperative assessment of sinonasal inverted papillomas. Am. J. Rhinol. 2008, 22, 144–150. [Google Scholar] [CrossRef]
- Weber, R.K.; Hosemann, W.; Kühnel, T. Hands-On Dissection Guide on Advanced Endoscopic Endonasal Sinus Surgery, 1st ed.; Endo Press GmbH: Tuttlingen, Germany, 2018. [Google Scholar]
- Busquets, J.M.; Hwang, P.H. Endoscopic resection of sinonasal inverted papilloma: A meta-analysis. Otolaryngol. Head Neck Surg. 2006, 134, 476–482. [Google Scholar] [CrossRef]
- Kamel, R.H.; Abdel Fattah, A.F.; Awad, A.G. Transnasal endoscopic medial maxillectomy in recurrent maxillary sinus inverted papilloma. Rhinology 2014, 52, 381–385. [Google Scholar] [CrossRef] [Green Version]
- Larget, I.; Bastier, P.L.; De Gabory, L. External versus endoscopic approach in the management of 131 sinonasal inverted papillomas. Rev. Laryngol. Otol. Rhinol. 2015, 136, 3–7. [Google Scholar]
- Heathcote, K.J.; Nair, S.B. The impact of modern techniques on the recurrence rate of inverted papilloma treated by endonasal surgery. Rhinology 2009, 47, 339–344. [Google Scholar] [CrossRef]
- Liu, Q.; Yu, H.; Minovi, A.; Wei, W.; Wang, D.; Zheng, C.; Li, F.; Zhang, Z. Management of maxillary sinus inverted papilloma via transnasal endoscopic anterior and medial maxillectomy. ORL J. Otorhinolaryngol. Relat. Spec. 2010, 72, 247–251. [Google Scholar] [CrossRef]
- Dean, N.R.; Illing, E.A.; Woodworth, B.A. Endoscopic resection of anterolateral maxillary sinus inverted papillomas. Laryngoscope 2015, 125, 807–812. [Google Scholar] [CrossRef]
- Salzano, G.; Turri-Zanoni, M.; Karligkiotis, A.; Zocchi, J.; Dell’Aversana Orabona, G.; Califano, L.; Battaglia, P.; Castelnuovo, P. Infraorbital nerve transposition to expand the endoscopic transnasal maxillectomy. Int. Forum Allergy Rhinol. 2017, 7, 149–153. [Google Scholar] [CrossRef] [PubMed]
- Sathananthar, S.; Nagaonkar, S.; Paleri, V.; Le, T.; Robinson, S.; Wormald, P.J. Canine fossa puncture and clearance of the maxillary sinus for the severely diseased maxillary sinus. Laryngoscope 2005, 115, 1026–1029. [Google Scholar] [CrossRef] [PubMed]
- Seiberling, K.; Ooi, E.; MiinYip, J.; Wormald, P.J. Canine fossa trephine for the severely diseased maxillary sinus. Am. J. Rhinol. Allergy 2009, 23, 615–618. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, A.; Pal, S.; Srivastava, A.; Saha, S. Modification of endoscopic medial maxillectomy: A novel approach for inverted papilloma of the maxillary sinus. J. Laryngol. Otol. 2015, 129, 159–163. [Google Scholar] [CrossRef]
- Miglani, A.; Hoxworth, J.M.; Zarka, M.A.; Lal, D. Use of intraoperative negative margins reduces inverted papilloma recurrence. Am. J. Rhinol. Allergy 2018, 32, 57–60. [Google Scholar] [CrossRef]
- Jiang, X.D.; Dong, Q.Z.; Li, S.L.; Huang, T.Q.; Zhang, N.K. Endoscopic surgery of a sinonasal inverted papilloma: Surgical strategy, follow-up, and recurrence rate. Am. J. Rhinol. Allergy 2017, 31, 51–55. [Google Scholar] [CrossRef]
- Adriaensen, G.F.; Lim, K.H.; Georgalas, C.; Reinartz, S.M.; Fokkens, W.J. Challenges in the Management of Inverted Papilloma: A Review of 72 Revision Cases. Laryngoscope 2016, 126, 322–328. [Google Scholar] [CrossRef]
- Bertazzoni, G.; Accorona, R.; Schreiber, A.; Pietrobon, G.; Karligkiotis, A.; Fazio, E.; Castelnuovo, P.; Nicolai, P. Postoperative long-term morbidity of extended endoscopic maxillectomy for inverted papilloma. Rhinology 2017, 55, 319–325. [Google Scholar] [CrossRef] [Green Version]
- Kasahara, N.; Morita, W.; Tanaka, R.; Hayashi, T.; Kenmotsu, S.; Ohshima, H. The Relationships of the Maxillary Sinus with the Superior Alveolar Nerves and Vessels as Demonstrated by Cone-Beam CT Combined With mu-CT and Histological Analyses. Anat. Rec. (Hoboken) 2016, 299, 669–678. [Google Scholar] [CrossRef]
- Robinson, S.; Wormald, P.J. Patterns of innervation of the anterior maxilla: A cadaver study with relevance to canine fossa puncture of the maxillary sinus. Laryngoscope 2005, 115, 1785–1788. [Google Scholar] [CrossRef]
- Schünke, M.; Schulte, E.; Schumacher, U. PROMETHEUS LernAtlas der Anatomie: Kopf, Hals und Neuroanatomie; 2. Auflage, Überarbeitet und Erweitert ed.; Thieme: New York, NY, USA, 2009. [Google Scholar]
- Elhadi, A.M.; Zaidi, H.A.; Yagmurlu, K.; Ahmed, S.; Rhoton, A.L., Jr.; Nakaji, P.; Preul, M.C.; Little, A.S. Infraorbital nerve: A surgically relevant landmark for the pterygopalatine fossa, cavernous sinus, and anterolateral skull base in endoscopic transmaxillary approaches. J. Neurosurg. 2016, 125, 1460–1468. [Google Scholar] [CrossRef] [PubMed]
- Moreno, P.M.; Meseguer, D.H. Bone changes after maxillary sinus surgery: An experimental scanning electron microscopy study. J. Laryngol. Otol. 2008, 122, 470–475. [Google Scholar] [CrossRef] [PubMed]







© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hildenbrand, T.; Weber, R.; Mertens, J.; Stuck, B.A.; Hoch, S.; Giotakis, E. Surgery of Inverted Papilloma of the Maxillary Sinus via Translacrimal Approach—Long-Term Outcome and Literature Review. J. Clin. Med. 2019, 8, 1873. https://doi.org/10.3390/jcm8111873
Hildenbrand T, Weber R, Mertens J, Stuck BA, Hoch S, Giotakis E. Surgery of Inverted Papilloma of the Maxillary Sinus via Translacrimal Approach—Long-Term Outcome and Literature Review. Journal of Clinical Medicine. 2019; 8(11):1873. https://doi.org/10.3390/jcm8111873
Chicago/Turabian StyleHildenbrand, Tanja, Rainer Weber, Janina Mertens, Boris A. Stuck, Stephan Hoch, and Evangelos Giotakis. 2019. "Surgery of Inverted Papilloma of the Maxillary Sinus via Translacrimal Approach—Long-Term Outcome and Literature Review" Journal of Clinical Medicine 8, no. 11: 1873. https://doi.org/10.3390/jcm8111873