Transvenous Lead Extraction SAFeTY Score for Risk Stratification and Proper Patient Selection for Removal Procedures Using Mechanical Tools

Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Lead Extraction Techniques
3. Definitions
- Complete procedural success: removal of all targeted leads and all lead material from the vascular space, with the absence of any permanently disabling complication or procedure-related death.
- Clinical success: removal of all targeted leads and all lead material from the vascular space or retention of a small portion of the lead (tip) or a small part (<4 cm) of the lead or insulation (complete or partial radiographic success), not increasing the risk of complication or perpetuation of infection or causing any permanently disabling complication or procedure-related death.
3.1. Data Analysis
3.2. Statistical Analysis
4. Results
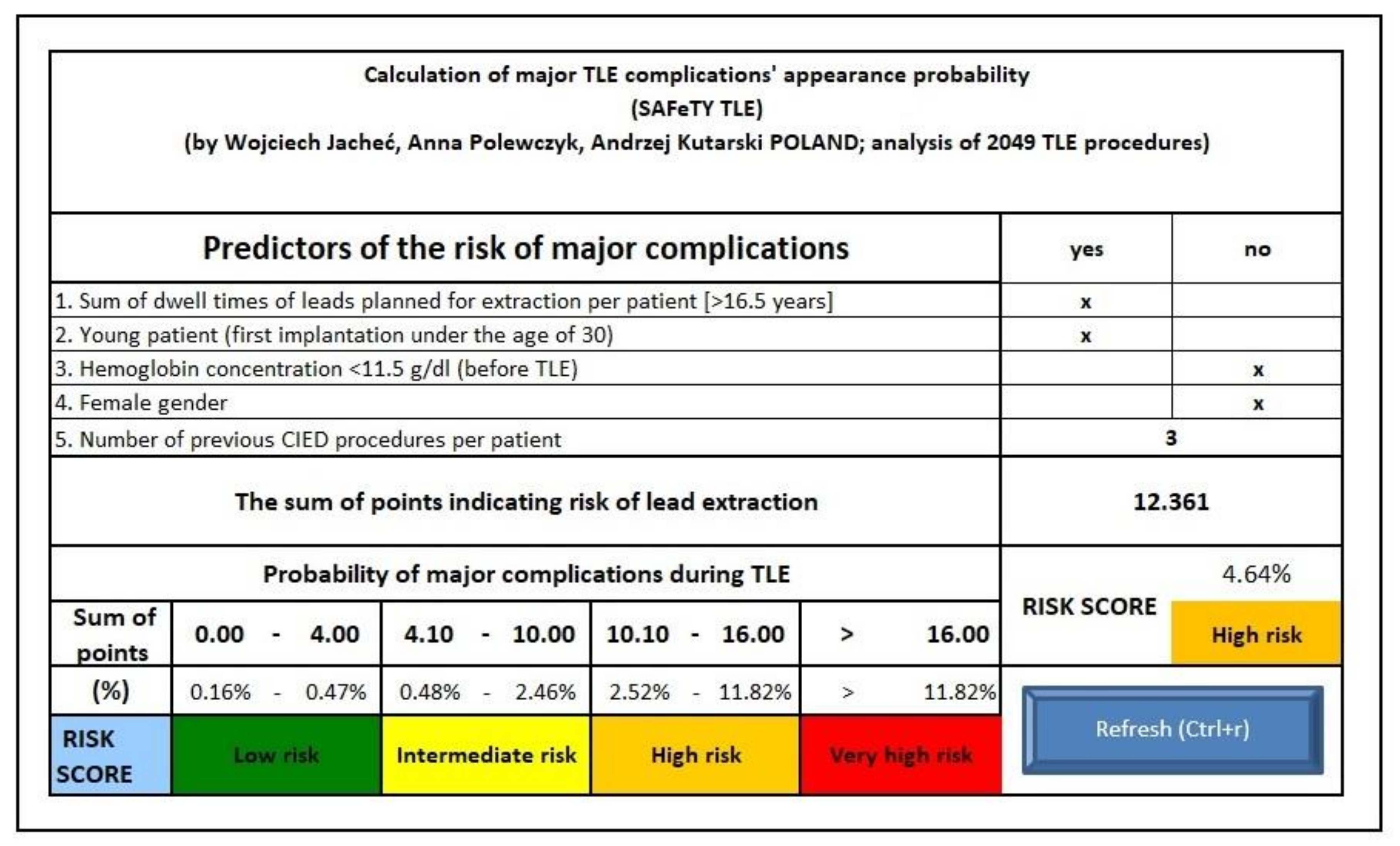
| S | sum of lead dwell times | 6.095 points |
| A | anemia | 2.291 points |
| Fe | female gender | 2.740 points |
| T | treatment (previous procedures) | 1.364 points for each procedure |
| Y | young patient (first implantation under the age of 30) | 2.174 points |
| TLE | transvenous lead extraction |
5. Discussion
6. Limitations
7. Conclusions
Author Contributions
Conflicts of Interest
References
- Raatikainen, M.J.P.; Arnar, D.O.; Merkely, B.; Nielsen, J.C.; Hindricks, G.; Heidbuchel, H.; Camm, J. A Decade of Information on the Use of Cardiac Implantable Electronic Devices and Interventional Electrophysiological Procedures in the European Society of Cardiology Countries: 2017 Report from the European Heart Rhythm Association. Europace 2017, 19 (Suppl. S2), ii1–ii90. [Google Scholar] [CrossRef] [PubMed]
- Kennergren, C.; Bjurman, C.; Wiklund, R.; Gäbel, J. A single-centre experience of over one thousand lead extractions. Europace 2009, 11, 612–617. [Google Scholar] [CrossRef] [PubMed]
- Wazni, O.; Epstein, L.M.; Carrillo, R.G.; Love, C.; Adler, S.W.; Riggio, D.W.; Karim, S.S.; Bashir, J.; Greenspon, A.J.; DiMarco, J.P.; et al. Lead Extraction in the Contemporary Setting: The LExICon Study an Observational Retrospective Study of Consecutive Laser Lead Extractions. JACC 2010, 55, 579–586. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Monaco, A.; Pelargonio, G.; Narducci, M.L.; Manzoli, L.; Boccia, S.; Flacco, M.E.; Capasso, L.; Barone, L.; Perna, F.; Bencardino, G.; et al. Safety of transvenous lead extraction according to centre volume: a systematic review and meta-analysis. Europace 2014, 16, 1496–1507. [Google Scholar] [CrossRef] [PubMed]
- Poole, J.E.; Gleva, M.J.; Mela, T.; Chung, M.K.; Uslan, D.Z.; Borge, R.; Gottipaty, V.; Shinn, T.; Dan, D.; Feldman, L.A.; et al. Complication rates associated with pacemaker or implantable cardioverter-defibrillator generator replacements and upgrade procedures: Results from the REPLACE registry. Circulation 2010, 122, 1553–1561. [Google Scholar] [CrossRef] [PubMed]
- Barakat, A.F.; Wazni, O.M.; Tarakji, K.; Saliba, W.I.; Nimri, N.; Rickard, J.; Brunner, M.; Bhargava, M.; Kanj, M.; Baranowski, B.; et al. Transvenous lead extraction at the time of cardiac implantable electronic device upgrade: Complexity, safety, and outcomes. Heart Rhythm 2017, 14, 1807–1811. [Google Scholar] [CrossRef] [PubMed]
- Mazzone, P.; Migliore, F.; Bertaglia, E.; Facchin, D.; Daleffe, E.; Calzolari, V.; Crosato, M.; Melillo, F.; Peruzza, F.; Marzi, A.; et al. Safety and efficacy of the new bidirectional rotational Evolution® mechanical lead extraction sheath: results from a multicentre Italian registry. Europace 2018, 20, 829–834. [Google Scholar] [CrossRef] [PubMed]
- Bontempi, L.; Vassanelli, F.; Cerini, M.; D’Aloia, A.; Vizzardi, E.; Gargaro, A.; Chiusso, F.; Mamedouv, R.; Lipari, A.; Curnis, A. Predicting the difficulty of a lead extraction procedure: the LED index. J. Cardiovasc. Med. 2014, 15, 668–673. [Google Scholar] [CrossRef] [PubMed]
- Brunner, M.P.; Yu, C.; Hussein, A.A.; Tarakji, K.G.; Wazni, O.M.; Kattan, M.W.; Wilkoff, B.L. Nomogram for predicting 30-day all-cause mortality after transvenous pacemaker and defibrillator lead extraction. Heart Rhythm 2015, 12, 2381–2386. [Google Scholar] [CrossRef] [PubMed]
- Oszczygieł, E.; Kutarski, A.; Oszczygieł, A.; Mańkowska-Załuska, B.; Chudzik, M.; Wranicz, J.K.; Cygankiewicz, I. Risk score to assess mortality risk in patients undergoing transvenous lead extraction. Pacing Clin. Electrophysiol. 2017, 40, 918–923. [Google Scholar] [CrossRef] [PubMed]
- Kusumoto, F.M.; Schoenfeld, M.H.; Wilkoff, B.; Berul, C.I.; Birgersdotter-Green, U.M.; Carrillo, R.; Cha, Y.M.; Clancy, J.; Deharo, J.C.; Ellenbogen, K.A.; et al. 2017 HRS expert consensus statement on cardiovascular implantable electronic device lead management and extraction. Heart Rhythm 2017, 14, e503–e551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bongiorni, M.G.; Kennergren, C.; Butter, C.; Deharo, J.C.; Kutarski, A.; Rinaldi, C.A.; Romano, S.L.; Maggioni, A.P.; Andarala, M.; Auricchio, A.; et al. The European Lead Extraction ConTRolled (ELECTRa) study: European Heart Rhythm Association (EHRA) Registry of Transvenous Lead Extraction Outcomes. Eur. Heart J. 2017, 38, 2995–3005. [Google Scholar] [CrossRef] [PubMed]
- Byrd, C.L.; Schwartz, S.J.; Hedin, N. Lead extraction. Indications and techniques. Cardiol. Clin. 1992, 10, 735–748. [Google Scholar] [CrossRef]
- Byrd, C.L.; Wilkoff, B.L.; Love, C.J.; Sellers, T.D.; Turk, K.T.; Reeves, R.; Young, R.; Crevey, B.; Kutalek, S.P.; Freedman, R.; et al. Intravascular extraction of problematic or infected permanent pacemaker leads: 1994-1996. U.S. Extraction Database, MED Institute. Pacing Clin. Electrophysiol. 1999, 22, 1348–1357. [Google Scholar] [CrossRef] [PubMed]
- Fu, H.X.; Huang, X.M.; Zhong, L.I.; Osborn, M.J.; Asirvatham, S.J.; Espinosa, R.E.; Brady, P.A.; Lee, H.C.; Greason, K.L.; Baddour, L.M.; et al. Outcomes and complications of lead removal: can we estabilish a risk stratification schema for a collaborative and effective approach? Pacing Clin. Electrophysiol. 2015, 38, 1439–1447. [Google Scholar] [CrossRef] [PubMed]
- Kancharla, K.; Acker, N.G.; Li, Z.; Samineni, S.; Cai, C.; Espinosa, R.E.; Osborn, M.; Mulpuru, S.K.; Asirvatham, S.J.; Friedman, P.A.; et al. Efficacy and Safety of Transvenous Lead Extraction in the Device Laboratory and Operating Room Guided by a Novel Risk Stratification Scheme. JACC Clin. Electrophysiol. 2019, 5, 174–182. [Google Scholar] [CrossRef] [PubMed]
- Sood, N.; Martin, D.T.; Lampert, R.; Curtis, J.P.; Parzynski, C.; Clancy, J. Incidence and Predictors of Perioperative Complications with Transvenous Lead Extractions: Real-World Experience with National Cardiovascular Data Registry. Circ. Arrhythm. Electrophysiol. 2018, 11, e004768. [Google Scholar] [CrossRef] [PubMed]
- Zucchelli, G.; Di Cori, A.; Segreti, L.; Laroche, C.; Blomstrom-Lundqvist, C.; Kutarski, A.; Regoli, F.; Butter, C.; Defaye, P.; Pasquié, J.L.; et al. Major cardiac and vascular complications after transvenous lead extraction: acute outcome and predictive factors from the ESC-EHRA ELECTRa (European Lead Extraction ConTRolled) registry. Europace 2019, 21, 771–780. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Major Complications | Without Major Complications | χ2/U Mann-Withney | Univariate Logistic Regression | |||
|---|---|---|---|---|---|---|
| n = 2049 | 37 | 2012 | p | OR | 95% CI | p |
| Age in the time of TLE | 64.03 ± 16.62 | 64.99 ± 15.84 | 0.750 | 0.996 | 0.977–1.016 | 0.713 |
| Age < 30 year, n (%) | 8 (21.622) | 167 (8.302) | 0.010 | 3.041 | 1.368–6.762 | 0.006 |
| Male sex, n (%) | 12 (32.432) | 1237 (61.481) | 0.000 | 0.306 | 0.153–0.613 | 0.001 |
| Female sex, n (%) | 25 (67.568) | 775 (38.519) | 0.000 | 3.270 | 1.633–6.549 | 0.001 |
| NYHA functional class I–II vs. III–IV, n (%) | 33/4 (89.19/10.81) | 1757/255 (87.33/12.67) | 0.930 | 0.718 | 0.435–1.182 | 0.192 |
| LVEF (change by 10%) | 45.556 ± 8.433 | 41.541 ± 10.950 | 0.032 | 1.530 | 1.032–2.270 | 0.034 |
| Creatinine concentration >2mg %, n (%) | 4 (10.81) | 108 (5.37) | 0.281 | 2.190 | 0.760–6.308 | 0.146 |
| Hemoglobin concentration (g/dL) | 11.975 ± 2.174 | 13.110 ± 1.883 | 0.000 | 0.760 | 0.650–0.882 | 0.001 |
| Anticoagulant therapy, n (%) | 9 (24.32) | 690 (34.29) | 0.275 | 0.613 | 0.288–1.306 | 0.204 |
| Antiplatelet therapy, n (%) | 11 (29.73) | 898 (44.63) | 0.101 | 0.560 | 0.275–1.140 | 0.110 |
| Infective indications, n (%) | 14 (37.8) | 801 (39.8) | 0.941 | 0.821 | 0.416–1.620 | 0.569 |
| Pocket infection, n (%) | 5 (13.51) | 580 (28.82) | 0.063 | 1.179 | 0.860–1.601 | 0.291 |
| Lead related infective endocarditis, n (%) | 12 (32.43) | 537 (26.69) | 0.552 | 1.168 | 0.573–1.238 | 0.669 |
| Number of procedures before TLE | 3.216 ± 1.766 | 1.823 ± 1.104 | 0.000 | 1.785 | 1.502–2.121 | 0.000 |
| Leads on the either side of chest, n (%) | 6 (16.216) | 85 (4.225) | 0.000 | 4.335 | 1.761–10.67 | 0.001 |
| TLE for leads implanted on both sides in the chest wall, during the same TLE procedure, n (%) | 5 (13.514) | 30 (1.491) | 0.000 | 10.32 | 3.759–28.32 | 0.000 |
| Age of the oldest extracted lead (years) | 19.145 ± 19.014 | 7.482 ± 5.686 | 0.000 | 1.162 | 1.118–1.207 | 0.000 |
| Mean age of extracted lead (years) | 16.523 ± 18.574 | 6.791 ± 4.885 | 0.000 | 1.194 | 1.138–1.253 | 0.000 |
| Sum of lead dwell times planned for extraction (years) | 28.532 ± 20.229 | 11.718 ± 10.665 | 0.000 | 1.072 | 1.053–1.092 | 0.000 |
| Number of abandoned leads in patients eligible for extraction | 0.705 ± 1.052 | 0.187 ± 0.518 | 0.000 | 2.400 | 1.720–3.351 | 0.000 |
| Presence of abandoned lead(s) before TLE, n (%) | 14 (37.838) | 269 (13.370) | 0.000 | 3.944 | 2.004–0.762 | 0.000 |
| High probability of scar tissue binding the leads, n (%) | 7 (19.919) | 101 (5.020) | 0.000 | 3.624 | 1.478–8.888 | 0.005 |
| TLE of ICD lead, n (%) | 4 (10.811) | 515 (25.60) | 0.063 | 0.345 | 0.122–0.979 | 0.045 |
| Targeted extraction of RA lead (any), n (%) | 30 (81.081) | 1169 (58.101) | 0.008 | 3.091 | 1.350–7.075 | 0.008 |
| Planned extraction of UP A lead, n (%) | 7 (18.919) | 96 (4.771) | 0.000 | 4.706 | 2.014–10.99 | 0.000 |
| Considered extraction of UP V lead, n (%) | 8 (21.622) | 188 (9.344) | 0.026 | 2.675 | 1.205–5.938 | 0.016 |
| TLE of UP leads, n (%) | 10 (27.027) | 231 (11.481) | 0.008 | 2.854 | 1.363–5.974 | 0.005 |
| TLE of UP leads above the median of age, n (%) | 11 (29.730) | 157 (7.803) | 0.000 | 1.739 | 1.121–2.698 | 0.014 |
| TLE of inactive leads, n (%) | 18 (48.649) | 320 (15.905) | 0.000 | 2.117 | 1.427–3.141 | 0.000 |
| TLE leads on either side of chest, n (%) | 5 (13.514) | 30 (1.491) | 0.000 | 10.32 | 3.759–28.319 | 0.000 |
| TLE of the more than three leads, n (%) | 5 (13.514) | 76 (3.777) | 0.009 | 3.978 | 1.507–10.50 | 0.005 |
| Disruption of lead during TLE, n (%) | 5 (13.514) | 71 (3.529) | 0.006 | 4.272 | 1.615–11.30 | 0.003 |
| Any technical problem, n (%) | 14 (37.838) | 311 (15.457) | 0.000 | 3.329 | 1.694–6.542 | 0.001 |
| Number of big technical problems, n (%) | 0.432 ± 0.689 | 0.142 ± 0.413 | 0.000 | 2.464 | 1.559–3.894 | 0.001 |
| Major Complications | Multivariate Regression | ||
|---|---|---|---|
| OR | 95% CI | p | |
| Sum of dwell times of leads planned for extraction per patient >16.5 years | 6.095 | 2.299–16.16 | 0.000 |
| Young patient (first implantation under the age of 30) | 2.174 | 0.881–5.368 | 0.092 |
| Hemoglobin concentration <11.5 g/dL | 2.291 | 1.127–4.655 | 0.022 |
| Female gender | 2.740 | 1.310–5.732 | 0.007 |
| LVEF (change by 10%) | 0.827 | 0.605–1.129 | 0.231 |
| Number of procedures before TLE | 1.364 | 1.048–1.774 | 0.021 |
| Leads on the either side of chest | 0.388 | 0.045–3.371 | 0.391 |
| Need for extracting leads implanted on both sides in the chest wall during the same TLE procedure | 1.250 | 0.445–3.507 | 0.672 |
| High probability of scar tissue binding the leads- | 1.125 | 0.577–2.192 | 0.730 |
| TLE of ICD lead | 0.576 | 0.174 ± 1,192 | 0.367 |
| Number of abandoned leads in patients eligible for extraction | 5.055 | 0.485–52.63 | 0.175 |
| Planned extraction of four or more leads during TLE procedure | 0.697 | 0.185–2.629 | 0.594 |
| Presence of abandoned lead(s) before TLE | 1.099 | 0.338–3.576 | 0.875 |
| Targeted extraction of RA lead (any) | 0.954 | 0.339–2.680 | 0.928 |
| Planned extraction of UP A lead | 1.538 | 0.527–4.490 | 0.431 |
| Considered extraction of UP V lead | 0.495 | 0.170–1.441 | 0.197 |
| Major Complication | OR (SAFeTY-TLE Points) | 95% CI | p |
|---|---|---|---|
| Sum of the dwell times of leads planned for extraction per patient (>16.5 years) | 6.095 | 2.299–16.12 | 0.000 |
| Young patient (first implantation under the age of 30) | 2.174 | 0.881–5.368 | 0.092 |
| Hemoglobin concentration <11.5 g/dL (before TLE) | 2.291 | 1.127–4.655 | 0.022 |
| Female gender | 2.740 | 1.310–5.732 | 0.007 |
| Number of previous CIED procedures per patient (for each procedure) | 1.364 | 1.048–1.774 | 0.021 |
| Risk Assessment Using TLE SAFeTY Score | |||
| TLE SAFeTY | Risk Score | ||
| 0.00–4.00 | Low risk (0.16–0.47%) | ||
| 4.10–10.00 | Moderate risk (0.48–2.46%) | ||
| 10.1–16.00 | High risk (2.52–11.82%) | ||
| >16.00 | Very high risk (>11.82%) | ||
| Major Complications: Appearance, Kind of Injury, Rescue Procedures, and Outcome | No (%) of MJC | % of All TLE | Place of Structural Damage | No of SAFeTY TLE Points | Fatal Outcome | ||||
|---|---|---|---|---|---|---|---|---|---|
| RA | RV | CS | SVC | Other | n (%) | ||||
| Hemopericardium—cardiac surgery | 19 (51.35) | 0.93% | 13 | 3 | 3 | 0 | 0 | 12.05 ** (3.66–19.18) *** | 6 (31.6) |
| Hemopericardium—pericardiocentesis—effective drainage | 11 (29.73) | 0.54% | 10* | 2* | 0 | 0 | 0 | 14.72 ** (10.20–18.76) *** | 0 (0.0) |
| Hemothorax—pleural drainage | 3 (8.11) | 0.15% | 0 | 0 | 0 | 3 | 0 | 11.07 ** (4.10–15.22) *** | 0 (0.0) |
| Hemothorax—thoracic surgery | 1 (2.70) | 0.05% | 0 | 0 | 0 | 1 | 0 | 7.769 | 0 (0.0) |
| Brain emboli—stroke—rehabilitation | 1 (2.70) | 0.05% | 0 | 0 | 0 | 0 | 1 | 10.19 | 0 (0.0) |
| Gradual decrease of contractility and delayed death (no structural damage) | 1 (2.70) | 0.05% | 0 | 0 | 0 | 0 | 1 | 5.47 | 1 (100) |
| Pulmonary embolism—cardiac surgery | 1 (2.70) | 0.05% | 0 | 0 | 0 | 0 | 1 | 13.85 | 1 (100) |
| All patients with major complications | 37 (100) | 1.81% | 23 * | 5 * | 3 | 4 | 3 | 12.54 ** (3.55–19.18) *** | 8 (21.62) |
| All patients without major complications | 2012 (0.00) | 98.19% | 0 | 0 | 0 | 0 | 0 | 5.66 **,AAA (1.36–22.85) *** | 0 (0.00) |
| Major Complications: Appearance, Kind of Injury, Rescue Procedures, and Outcome in Validated Group | No (%) of MJC | % of All TLE | Place of Structural Damage | No of SAFeTY TLE Points | Fatal Outcome | ||||
|---|---|---|---|---|---|---|---|---|---|
| RA | RV | CS | VCS | Other | n (%) | ||||
| Hemopericardium *—cardiac surgery | 7 (100.0) | 1.27% | 4 | 3 | 0 | 0 | 0 | 13.82 ** (6.40–24.77) *** | 0 (0.00) |
| All patients without major complications | 544 (0.00) | 98.73% | 0 | 0 | 0 | 0 | 0 | 6.65 **,AA (1.36–17.95) *** | 0 (0.00) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jacheć, W.; Polewczyk, A.; Polewczyk, M.; Tomasik, A.; Kutarski, A. Transvenous Lead Extraction SAFeTY Score for Risk Stratification and Proper Patient Selection for Removal Procedures Using Mechanical Tools. J. Clin. Med. 2020, 9, 361. https://doi.org/10.3390/jcm9020361
Jacheć W, Polewczyk A, Polewczyk M, Tomasik A, Kutarski A. Transvenous Lead Extraction SAFeTY Score for Risk Stratification and Proper Patient Selection for Removal Procedures Using Mechanical Tools. Journal of Clinical Medicine. 2020; 9(2):361. https://doi.org/10.3390/jcm9020361
Chicago/Turabian StyleJacheć, Wojciech, Anna Polewczyk, Maciej Polewczyk, Andrzej Tomasik, and Andrzej Kutarski. 2020. "Transvenous Lead Extraction SAFeTY Score for Risk Stratification and Proper Patient Selection for Removal Procedures Using Mechanical Tools" Journal of Clinical Medicine 9, no. 2: 361. https://doi.org/10.3390/jcm9020361