Cardiovascular Events after Community-Acquired Pneumonia: A Global Perspective with Systematic Review and Meta-Analysis of Observational Studies


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Population and Outcomes
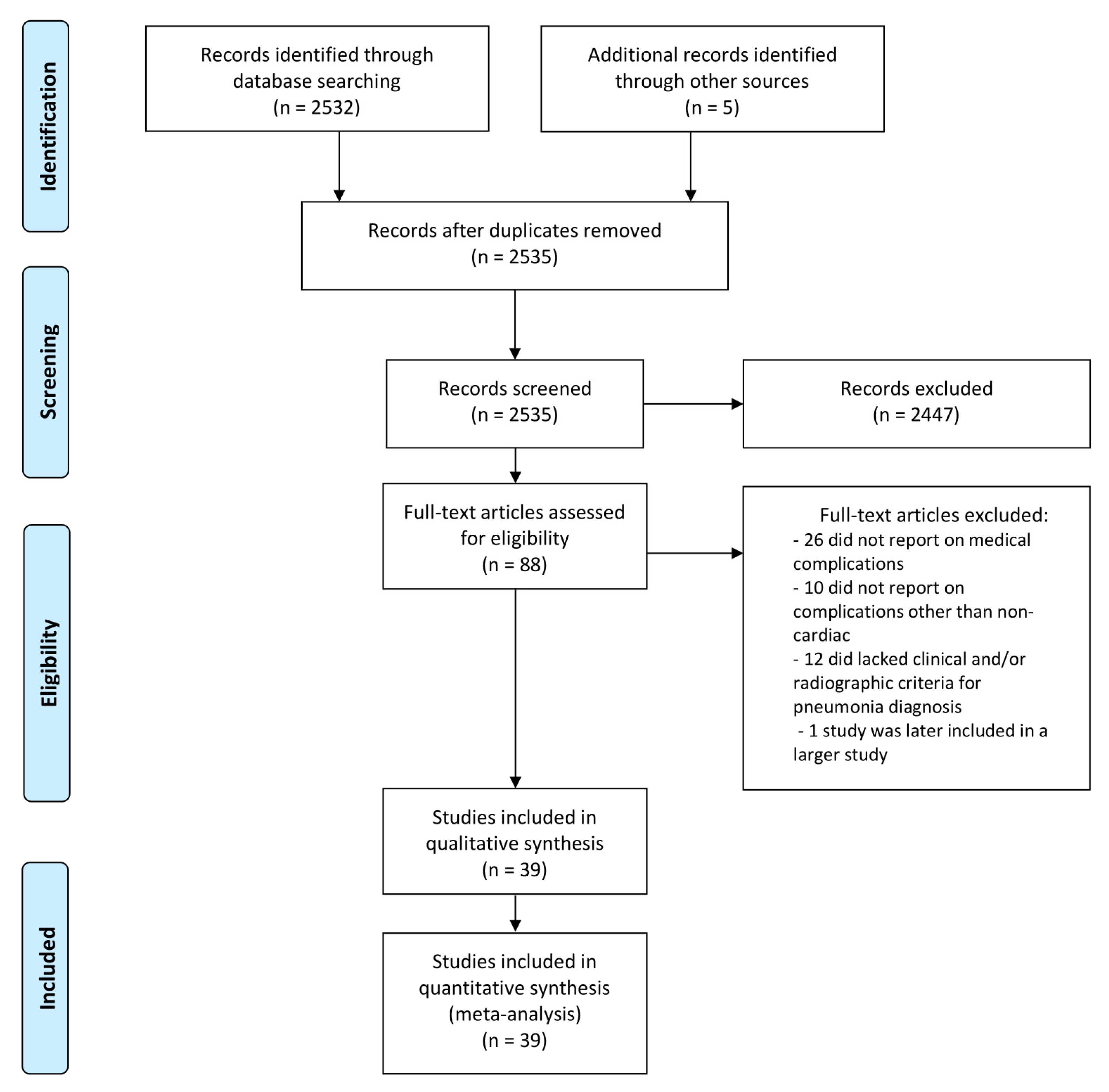
2.3. Study Selection, Data Extraction and Synthesis
2.4. Statistical Analysis
3. Results
3.1. Basic Science and Clinical Insights Associating CAP to CV Events
3.1.1. Coronary Arteries and Myocardial Infarction
3.1.2. Myocardium and Heart Failure
3.1.3. Cardiac Rhythm Disturbances
3.2. Clinical Studies of Short Term Incident Acute CV Disease after CAP
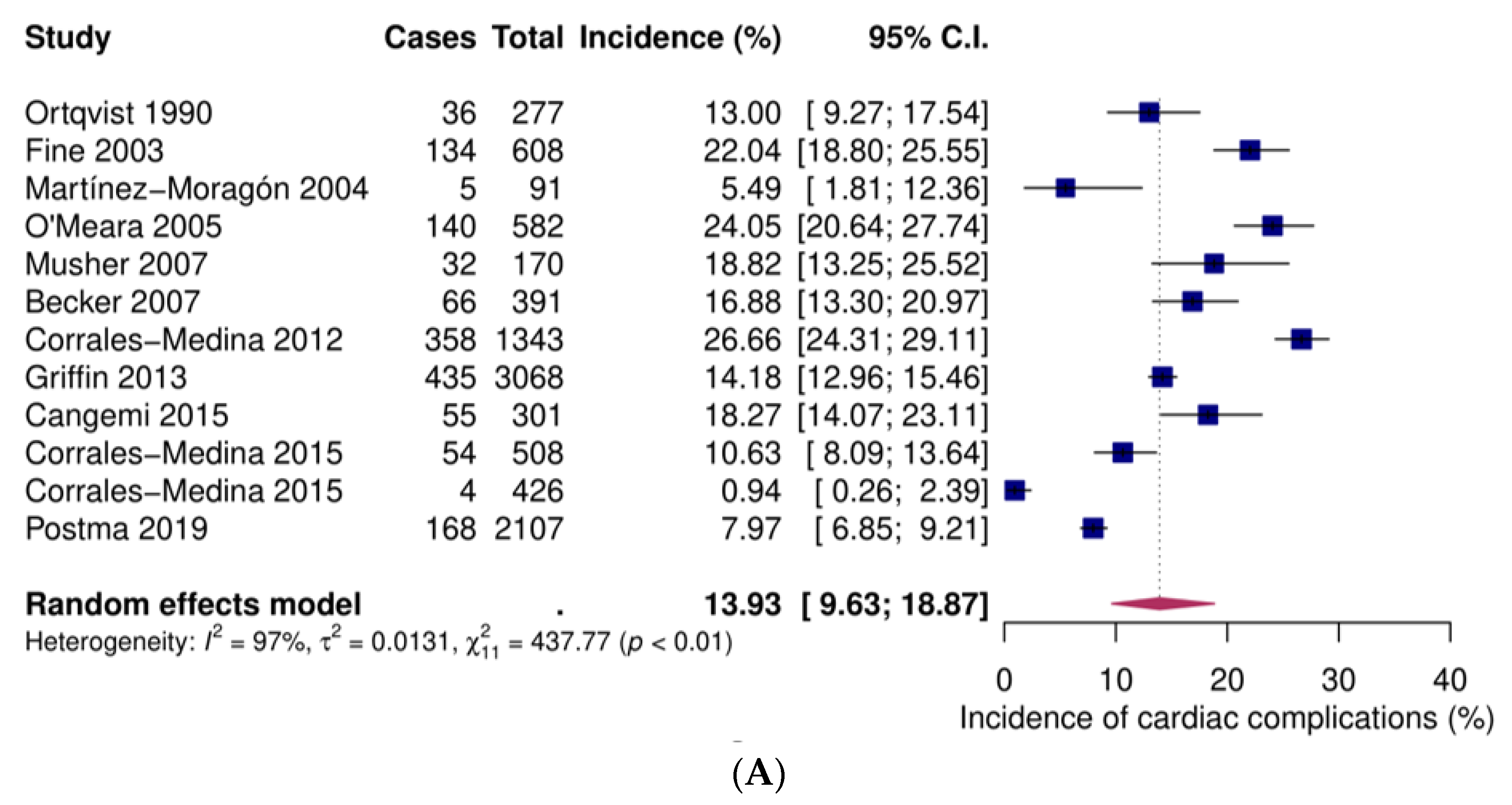
3.2.1. Overall Cardiac Complications
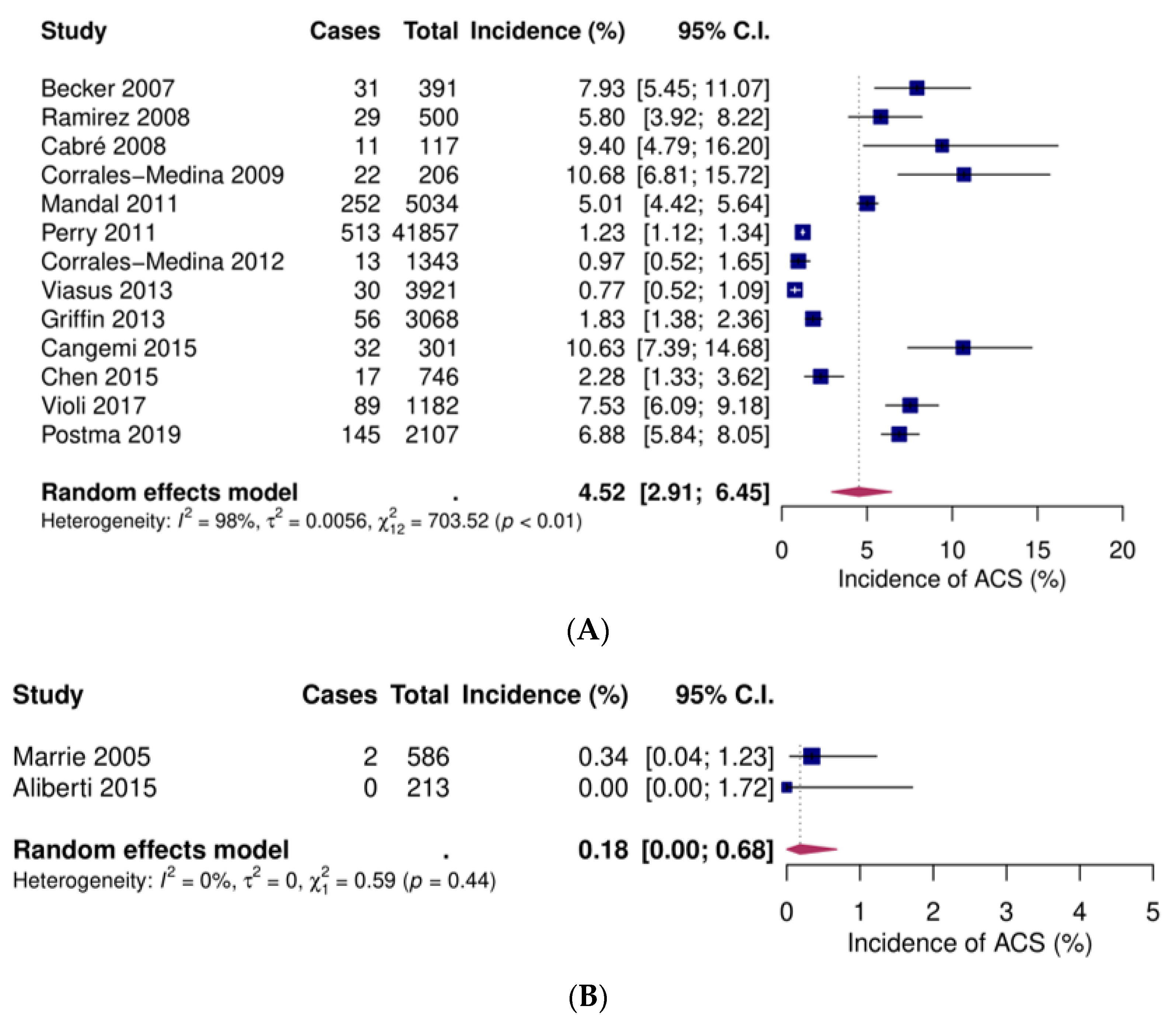
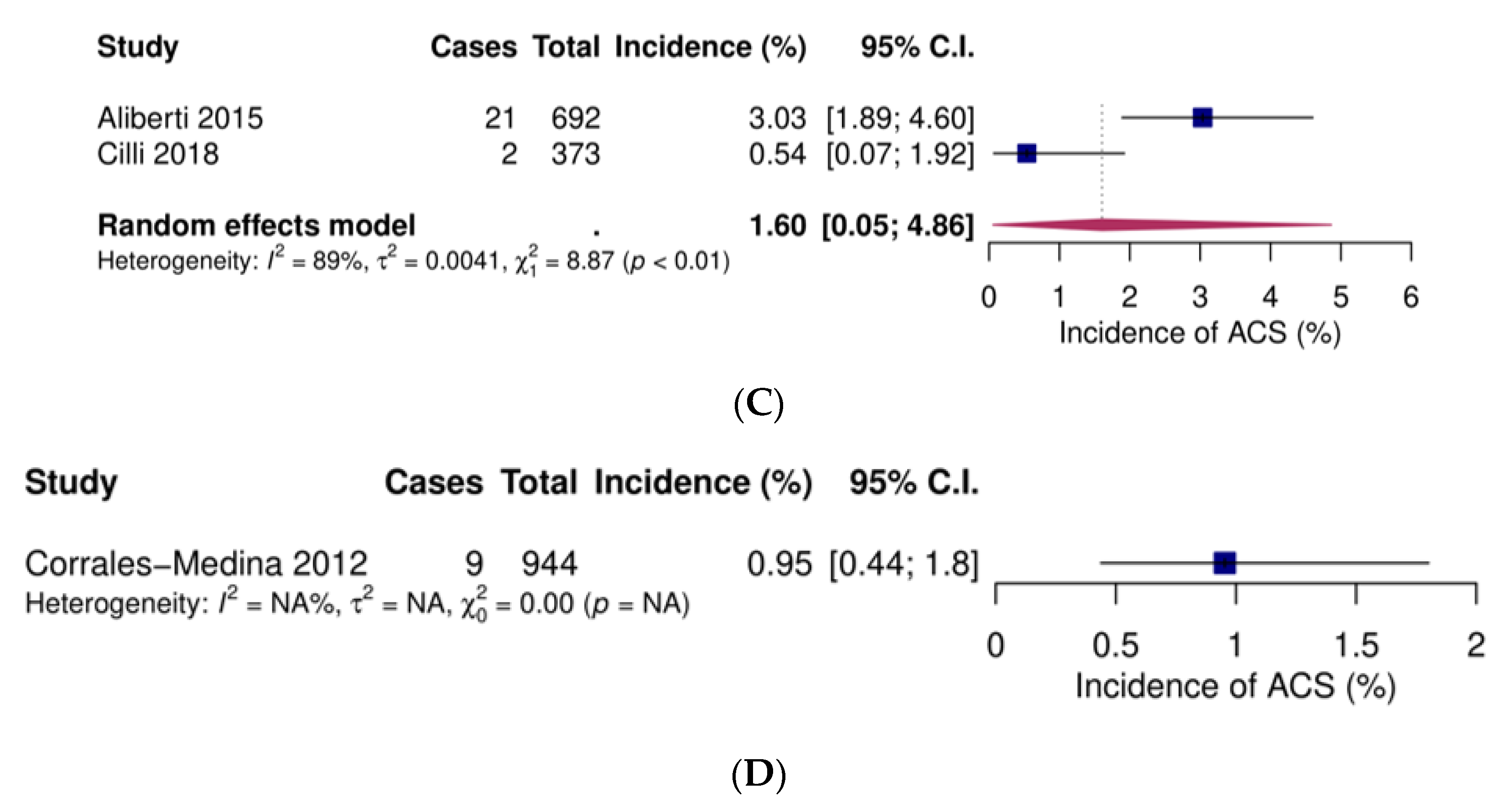
3.2.2. Acute Coronary Syndromes
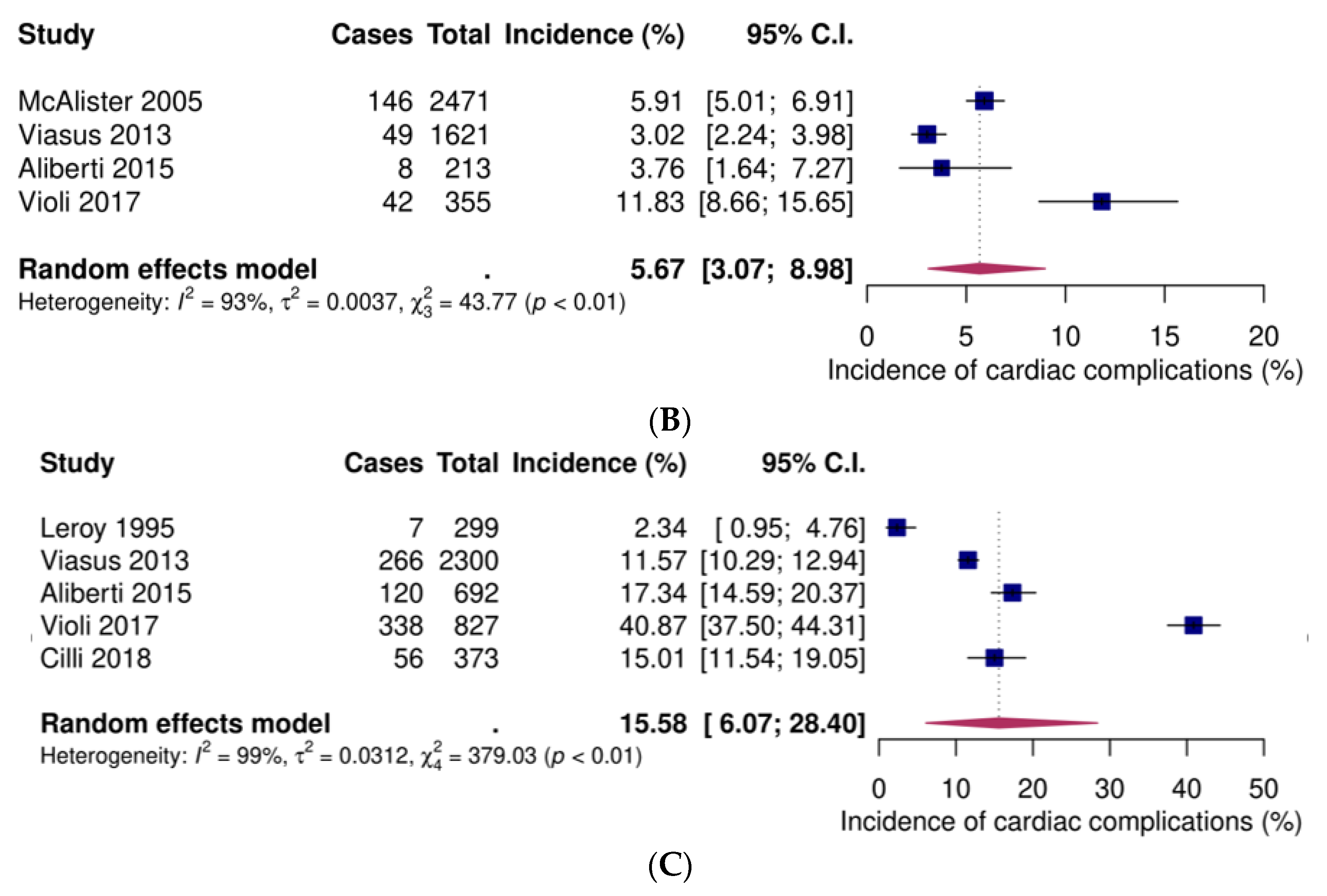
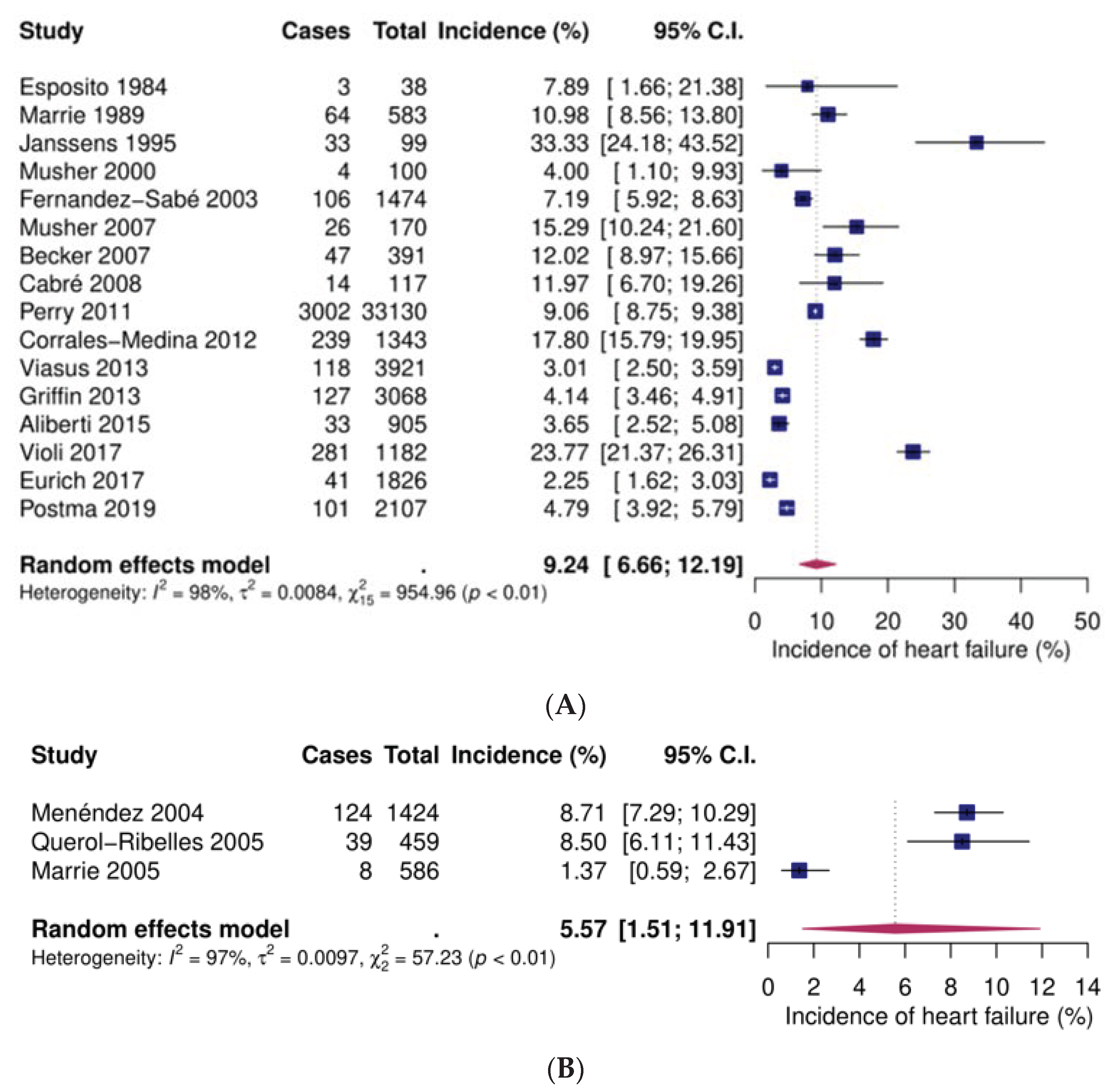
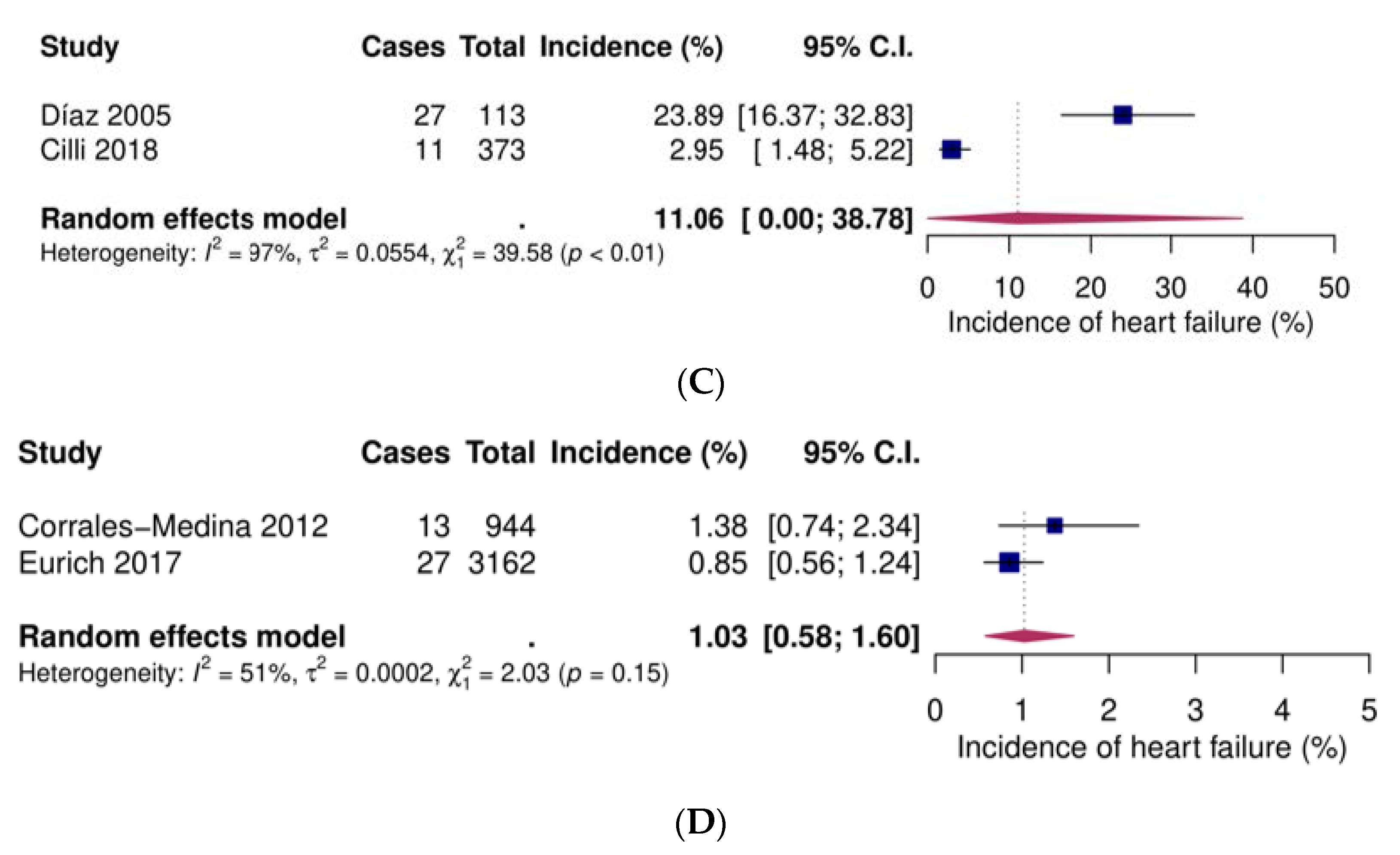
3.2.3. Heart Failure
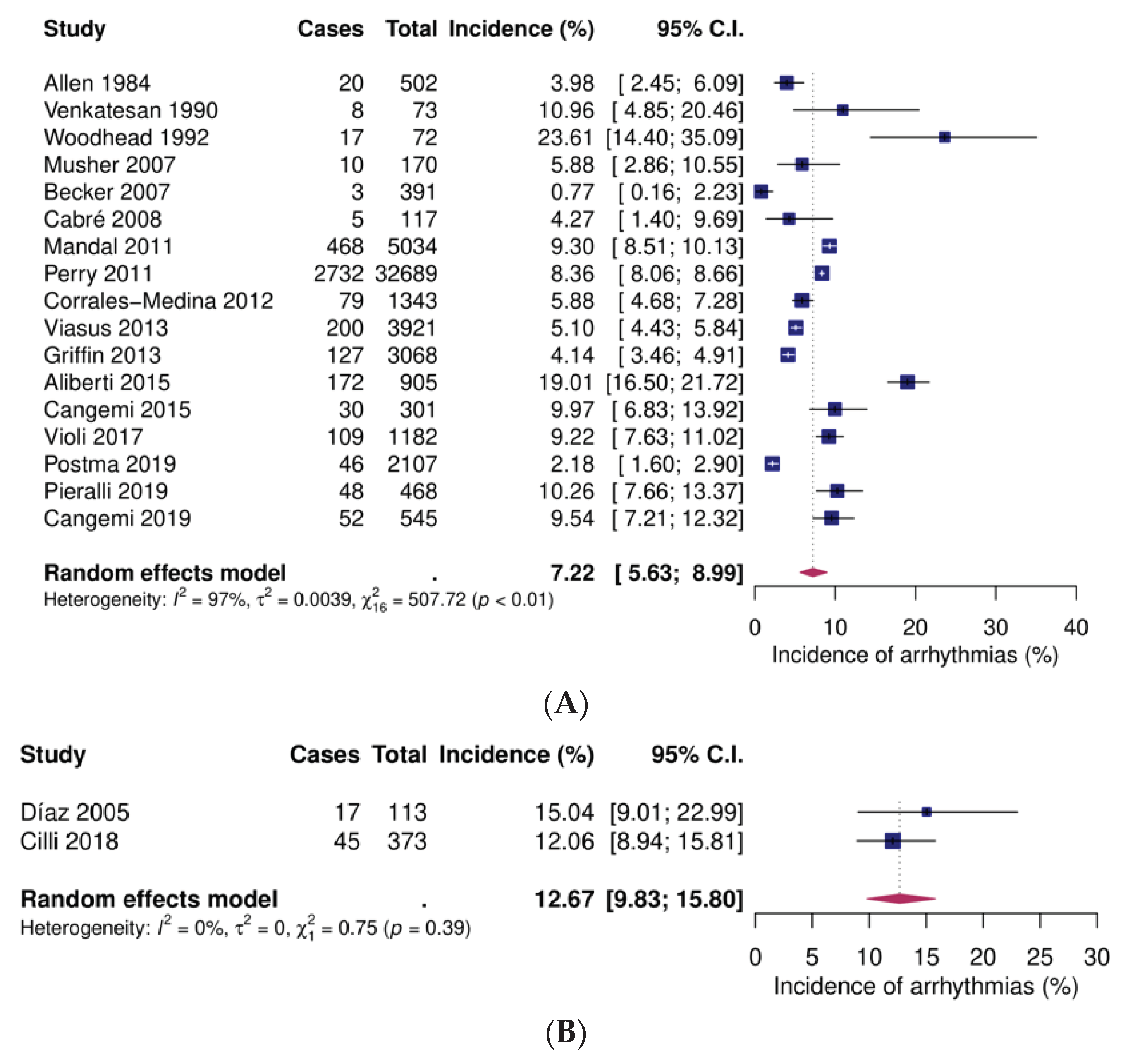
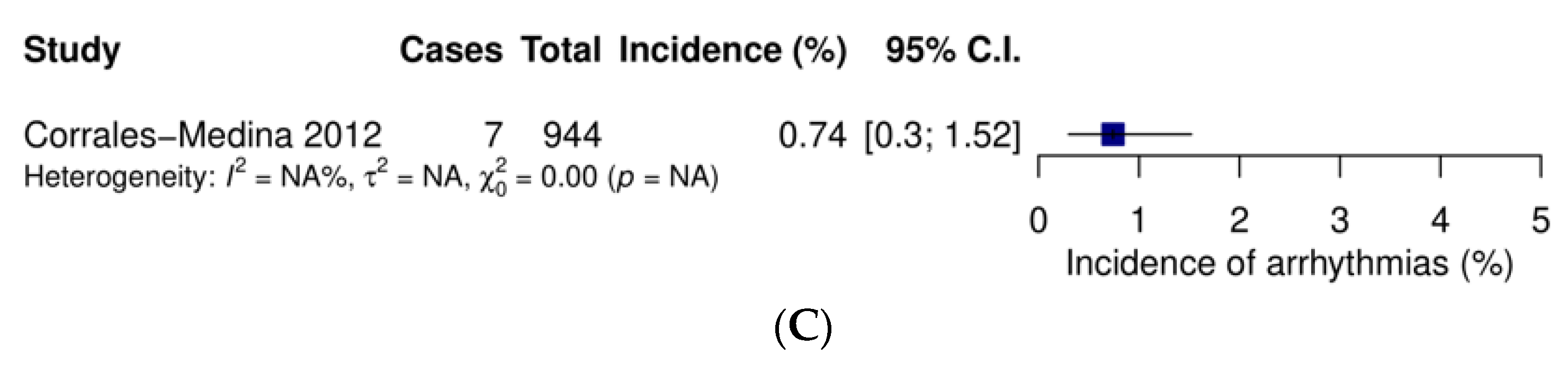
3.2.4. Arrhythmias
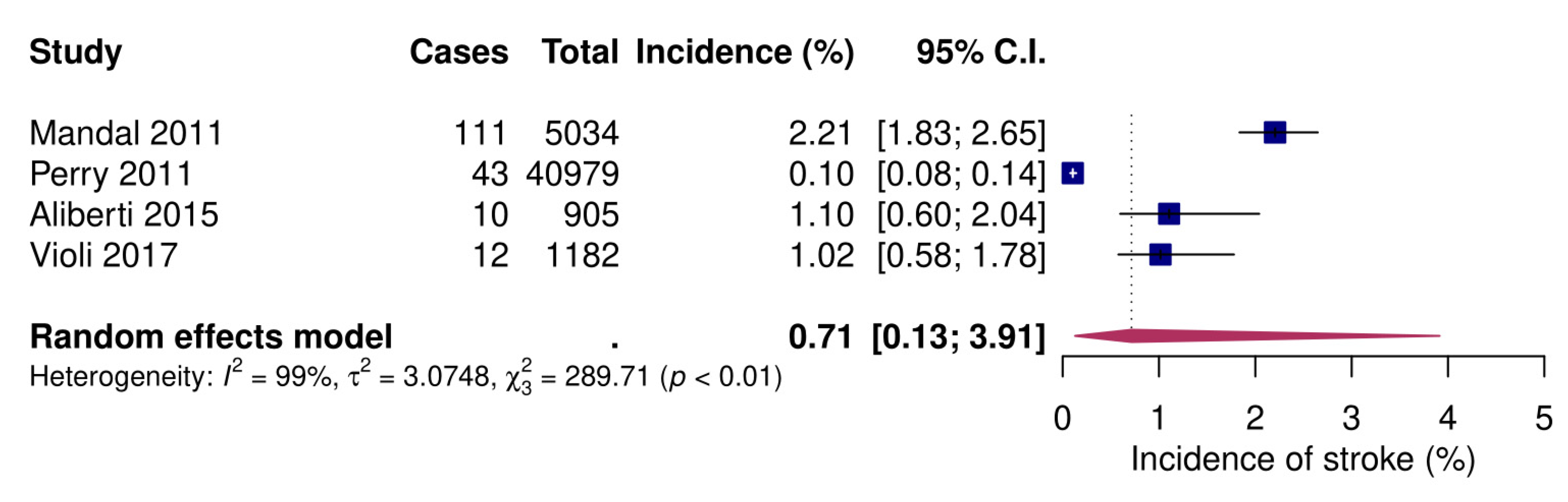
3.2.5. Stroke
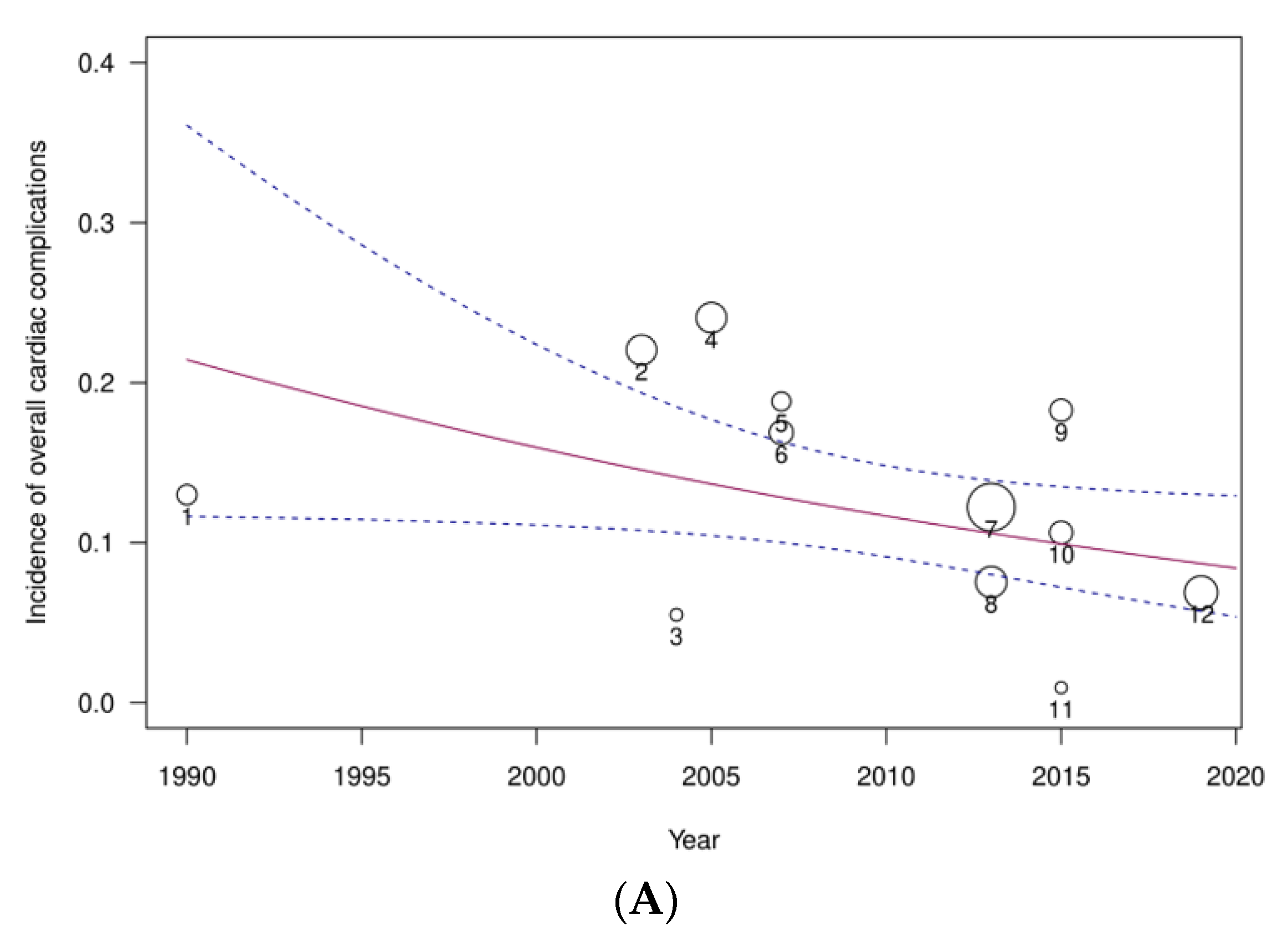
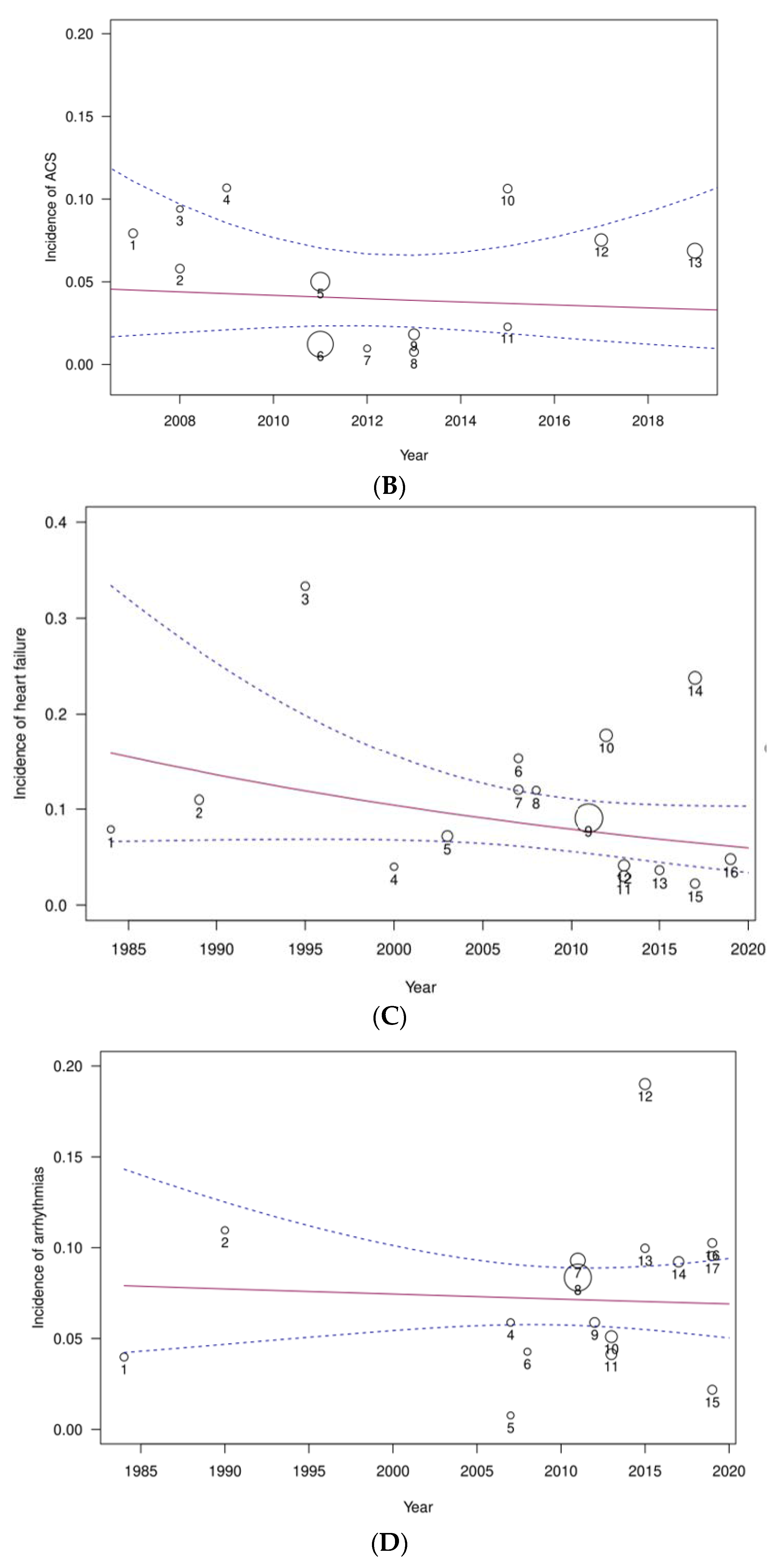
3.2.6. Meta-Regression Analysis and Publication Bias Assessment
3.3. Risk Factors and Impact of Cardiac Complications on CAP Outcomes
3.4. Long Tterm Outcomes after CAP
3.5. What Is the Role of Pharmacological Therapies?
3.5.1. Antiplatelet Drugs
3.5.2. Statins and Other Lipid Lowering Agents
3.5.3. Beta-Blockers, Angiotensin-Converting Enzyme Inhibitors (ACEi) and Angiotensin Receptor Blockers (ARB)
3.5.4. Corticosteroids
3.5.5. Novel Drugs
3.6. Vaccination
3.7. Effects of Antibiotics on the Cardiovascular System
4. Discussion
5. Future Directions
Supplementary Materials
Author Contributions
Conflicts of Interest
References
- National Vital Statistics Reports. Available online: https://www.cdc.gov/nchs/data/nvsr/nvsr68/nvsr68_09_tables-508.pdf (accessed on 1 November 2019).
- Rui, P.; Kang, K. National Hospital Ambulatory Medical Care Survey: 2016 Emergency Department Summary Tables. 2016. Available online: https://www.cdc.gov/nchs/data/nhamcs/web_tables/2016_ed_web_tables.pdf (accessed on 1 November 2019).
- OECD/EU. Health at a Glance: Europe 2018: State of Health in the EU Cycle; OECD Publishing: Paris, France, 2018; Available online: https://doi.org/10.1787/health_glance_eur-2018-en (accessed on 1 November 2019).
- Froes, F.; Diniz, A.; Mesquita, M.; Serrado, M.; Nunes, B. Hospital admissions of adults with community-acquired pneumonia in Portugal between 2000 and 2009. Eur. Respir. J. 2013, 41, 1141–1146. [Google Scholar] [CrossRef] [Green Version]
- Naghavi, M.; Abajobir, A.A.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abera, S.F.; Aboyans, V.; Adetokunboh, O.; Afshin, A.; Agrawal, A.; et al. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1151–1210. [Google Scholar] [CrossRef] [Green Version]
- Yende, S.; Angelo, G.D.; Kellum, J.A.; Weissfeld, L.; Fine, J.; Welch, R.D.; Kong, L.; Carter, M.; Angus, D.C.; Investigators, G. Inflammatory Markers at Hospital Discharge Predict Subsequent Mortality after Pneumonia and Sepsis. Am. J. Respir. Crit. Care Med. 2008, 177, 1242–1247. [Google Scholar] [CrossRef] [Green Version]
- Corrales-Medina, V.F.; Musher, D.M.; Shachkina, S.; Chirinos, J.A. Acute pneumonia and the cardiovascular system. Lancet 2013, 381, 496–505. [Google Scholar] [CrossRef]
- Bergh, C.; Fall, K.; Udumyan, R.; Sjo, H.; Montgomery, S. Severe infections and subsequent delayed cardiovascular disease. Eur. J. Prev. Cardiol. 2017, 24, 1958–1966. [Google Scholar] [CrossRef] [Green Version]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. Introduction to Meta-Analysis; John Wiley & Sons: Hoboken, NJ, USA, 2011. [Google Scholar]
- Raudenbush, S.W.; Bryk, A.S. Empirical Bayes Meta-Analysis. J. Educ. Stat. 1985, 10, 75–98. [Google Scholar] [CrossRef]
- Light, R.; Pillemer, D. Summing Up: The Science of Reviewing Research; Harvard University Press: Cambridge, MA, USA, 1984. [Google Scholar]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D. Fourth Universal Definition of Myocardial Infarction. J. Am. Coll. Cardiol. 2018, 72, 2231–2264. [Google Scholar] [CrossRef] [PubMed]
- Libby, P. Mechanisms of Acute Coronary Syndromes and Their Implications for Therapy. N. Engl. J. Med. 2013, 368, 2004–2013. [Google Scholar] [CrossRef] [Green Version]
- Kaynar, A.M.; Yende, S.; Zhu, L.; Frederick, D.R.; Chambers, R.; Burton, C.L.; Carter, M.; Stolz, D.B.; Agostini, B.; Gregory, A.D.; et al. Effects of intra-abdominal sepsis on atherosclerosis in mice. Crit. Care 2014, 18, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Mauriello, A.; Sangiorgi, G.; Fratoni, S.; Palmieri, G.; Bonanno, E.; Anemona, L.; Schwartz, R.S.; Spagnoli, L.G. Diffuse and Active Inflammation Occurs in Both Vulnerable and Stable Plaques of the Entire Coronary Tree A Histopathologic Study of Patients Dying of Acute Myocardial Infarction. J. Am. Coll. Cardiol. 2005, 45, 1585–1593. [Google Scholar] [CrossRef] [PubMed]
- Madjid, M.; Vela, D.; Khalili-Tabrizi, H.; Casscells, S.W.; Litovsky, S. Systemic infections cause exaggerated local inflammation in atherosclerotic coronary arteries: Clues to the triggering effect of acute infections on acute coronary syndromes. Tex. Heart Inst. J. 2007, 34, 11–18. [Google Scholar] [PubMed]
- Milbrandt, E.B.; Reade, M.C.; Lee, M.; Shook, S.L.; Angus, D.C.; Kong, L.; Carter, M.; Yealy, D.M.; Kellum, J.A.; Investigators, G. Prevalence and significance of coagulation abnormalities in community-acquired pneumonia. Mol. Med. 2009, 15, 438–445. [Google Scholar] [CrossRef] [PubMed]
- Cunnion, R.E.; Schaer, G.L.; Parker, M.M.; Natanson, C.; Parrillo, J.E. The coronary circulation in human septic shock. Circulation 1986, 73, 637–644. [Google Scholar] [CrossRef] [Green Version]
- Sibelius, U.; Grandel, U.; Buerke, M.; Mueller, D.; Kiss, L.; Kraemer, H.; Braun-dullaeus, R.; Haberbosch, W.; Seeger, W.; Grimminger, F. Staphylococcal α-toxin provokes coronary vasoconstriction and loss in Myocardial Contractility in Perfused Rat Hearts Role of Thromboxane Generation. Circulation 2000, 101, 78–85. [Google Scholar] [CrossRef] [Green Version]
- Kotaka, M.; Kitaura, Y. Myocarditis in Mice Light and Electron Microscopic, Virologic and Hemodynamic study. Am. J. Pathol. 1990, 136, 409–419. [Google Scholar]
- Brown, A.O.; Mann, B.; Gao, G.; Hankins, J.S.; Humann, J.; Giardina, J.; Faverio, P.; Restrepo, M.I.; Halade, G.V.; Mortensen, E.M.; et al. Streptococcus pneumoniae Translocates into the Myocardium and Forms Unique Microlesions That Disrupt Cardiac Function. PLoS Pathog. 2014, 10, e1004383. [Google Scholar] [CrossRef]
- Wilke, T.; Groth, A.; Mueller, S.; Pfannkuche, M.; Verheyen, F.; Linder, R.; Maywald, U.; Bauersachs, R.; Breithardt, G. Incidence and prevalence of atrial fibrillation: An analysis based on 8.3 million patients. Europace 2012, 15, 486–493. [Google Scholar] [CrossRef]
- Kirchhof, P.; Benussi, S.; Kotecha, D.; Ahlsson, A.; Atar, D.; Casadei, B.; Castella, M.; Diener, H.C.; Heidbuchel, H.; Hendriks, J.; et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur. Heart J. 2016, 37, 2893–2962. [Google Scholar] [CrossRef] [Green Version]
- Moss, T.J.; Calland, J.F.; Enfield, K.B.; Gomez-Manjarres, D.C.; Ruminski, C.; Dimarco, J.P.; Lake, D.E.; Moorman, J.R. New-onset atrial fibrillation in the critically III. Crit. Care Med. 2017, 45, 790–797. [Google Scholar] [CrossRef]
- Yoshida, T.; Uchino, S.; Yokota, T.; Fujii, T.; Uezono, S.; Takinami, M. The impact of sustained new-onset atrial fibrillation on mortality and stroke incidence in critically ill patients: A retrospective cohort study. J. Crit. Care 2018, 44, 267–272. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, T.; Uchino, S.; Sasabuchi, Y.; Hagiwara, Y.; The AFTER-ICU study group; Yoshida, T.; Nashiki, H.; Suzuki, H.; Takahashi, H.; Kishihara, Y.; et al. Prognostic impact of sustained new-onset atrial fibrillation in critically ill patients. Intensive Care Med. 2019, 46, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Allen, S.C. Lobar pneumonia in Northern Zambia: Clinical study of 502 adult patients. Thorax 1984, 39, 612–616. [Google Scholar] [CrossRef] [Green Version]
- Esposito, A.L. Community-Acquired Bacteremic Pneumococcal Pneumonia: Effect of Age on Manifestations and Outcome. Arch. Intern. Med. 1984, 144, 945–948. [Google Scholar] [CrossRef] [PubMed]
- Marrie, T.J.; Durant, H.; Yates, L. Community-acquired pneumonia requiring hospitalization: 5-year prospective study. Rev. Infect. Dis. 1989, 11, 586–599. [Google Scholar] [CrossRef] [PubMed]
- Ortqvist, A.; Hedlund, J.; Grillner, L.; Jalonen, E.; Kallings, I.; Leinonen, M.; Kalin, M. Aetiology, outcome and prognostic factors in community-acquired pneumonia requiring hospitalization. Eur. Respir. J. 1990, 3, 1105–1113. [Google Scholar]
- Venkatesan, P.; Gladman, J.; Macfarlane, J.T.; Barer, D.; Berman, P.; Kinnear, W.; Finch, R.G. A hospital study of community acquired pneumonia in the elderly. Thorax 1990, 45, 254–258. [Google Scholar] [CrossRef] [Green Version]
- Fine, M.J.; Smith, D.N.; Singer, D.E. Hospitalization decision in patients with community-acquired pneumonia: A prospective cohort study. Am. J. Med. 1990, 89, 713–721. [Google Scholar] [CrossRef]
- The British Thoracic Society Research Committee. The Public Health Laboratory Service The aetiology, management and outcome of severe community-acquired pneumonia on the intensive care unit. Respir. Med. 1992, 86, 7–13. [Google Scholar] [CrossRef]
- Leroy, O.; Santré, C.; Beuscart, C.; Georges, H.; Guery, B.; Jacquier, J.M.; Beaucaire, G. A five-year study of severe community-acquired pneumonia with emphasis on prognosis in patients admitted to an intensive care unit. Intensive Care Med. 1995, 21, 24–31. [Google Scholar] [CrossRef]
- Janssens, J.P.; Gauthey, L.; Herrmann, F.; Tkatch, L.; Michel, J.P. Community-acquired pneumonia in older patients. J. Am. Geriatr. Soc. 1996, 44, 539–544. [Google Scholar] [CrossRef] [PubMed]
- Musher, D.M.; Alexandraki, I.; Graviss, E.A.; Yanbeiy, N.; Eid, A.; Inderias, L.A.; Phan, H.M.; Solomon, E. Bacteremic and Nonbacteremic Pneumococcal. Medicine 2000, 79, 210–221. [Google Scholar] [CrossRef]
- Fernández-Sabé, N.; Carratalà, J.; Rosón, B.; Dorca, J.; Verdaguer, R.; Manresa, F.; Gudiol, F. Community-acquired pneumonia in very elderly patients: Causative organisms, clinical characteristics, and outcomes. Medicine 2003, 82, 159–169. [Google Scholar] [CrossRef] [PubMed]
- Fine, M.J.; Stone, R.A.; Lave, J.R.; Hough, L.J.; Obrosky, D.S.; Mor, M.K.; Kapoor, W.N. Implementation of an evidence-based guideline to reduce duration of intravenous antibiotic therapy and length of stay for patients hospitalized with community-acquired pneumonia: A randomized controlled trial. Am. J. Med. 2003, 115, 343–351. [Google Scholar] [CrossRef]
- Martínez-Moragón, E.; García Ferrer, L.; Serra Sanchis, B.; Fernández Fabrellas, E.; Gómez Belda, A.; Juive Pardo, R. La neumonía adquirida en la comunidad de los ancianos: Diferencias entre los que viven en residencias y en domicilios particulares. Arch. Bronconeumol. 2004, 40, 547–552. [Google Scholar] [CrossRef]
- Menéndez, R.; Torres, A.; Zalacaín, R.; Aspa, J.; Martín Villasclaras, J.J.; Borderías, J.; Benítez Moya, J.M.; Ruiz-Manzano, J.; Rodríguez de Castro, F.; Blanquer, J.; et al. Guidelines for the Treatment of Community-acquired Pneumonia Predictors of Adherence and Outcome. Am. J. Respir. Crit. Care 2005, 172, 757–762. [Google Scholar] [CrossRef] [PubMed]
- Querol-Ribelles, J.M.; Tenías, J.M.; Querol-Borrás, J.M.; Labrador, T.; Nieto, A.; González-Granda, D.; Martínez, I. Levofloxacin versus ceftriaxone plus clarithromycin in the treatment of adults with community-acquired pneumonia requiring hospitalization. Int. J. Antimicrob. Agents 2005, 25, 75–83. [Google Scholar] [CrossRef]
- Díaz, A.; Alvarez, M.; Callejas, C.; Rosso, R.; Schnettler, K.; Saldías, F. Clinical picture and prognostic factors for severe community-acquired pneumonia in adults admitted to the intensive care unit. Arch. Bronconeumol. 2005, 41, 20–26. [Google Scholar] [CrossRef]
- Marrie, T.J.; Huang, J.Q. Low-risk patients admitted with community-acquired pneumonia. Am. J. Med. 2005, 118, 1357–1363. [Google Scholar] [CrossRef]
- McAlister, F.A.; Majumdar, S.R.; Blitz, S.; Rowe, B.H.; Romney, J.; Marrie, T.J. The relation between hyperglycemia and outcomes in 2471 patients admitted to the hospital with community-acquired pneumonia. Diabetes Care 2005, 28, 810–815. [Google Scholar] [CrossRef] [Green Version]
- O’Meara, E.S.; White, M.; Siscovick, D.S.; Lyles, M.F.; Kuller, L.H. Hospitalization for pneumonia in the Cardiovascular Health Study: Incidence, mortality, and influence on longer-term survival. J. Am. Geriatr. Soc. 2005, 53, 1108–1116. [Google Scholar] [CrossRef] [PubMed]
- Musher, D.M.; Rueda, A.M.; Kaka, A.S.; Mapara, S.M. The Association between Pneumococcal Pneumonia and Acute Cardiac Events. Clin. Infect. Dis. 2007, 45, 158–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Becker, T.; Moldoveanu, A.; Cukierman, T.; Gerstein, H.C. Clinical outcomes associated with the use of subcutaneous insulin-by-glucose sliding scales to manage hyperglycemia in hospitalized patients with pneumonia. Diabetes Res. Clin. Pract. 2007, 78, 392–397. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, J.; Aliberti, S.; Mirsaeidi, M.; Peyrani, P.; Filardo, G.; Amir, A.; Moffett, B.; Gordon, J.; Blasi, F.; Bordon, J. Acute Myocardial Infarction in Hospitalized Patients with Community-Acquired Pneumonia. Clin. Infect. Dis. 2015, 47, 182–187. [Google Scholar] [CrossRef] [Green Version]
- Cabré, M.; Serra-Prat, M.; Force, L.; Palomera, E.; Pallarés, R. Functional status as a risk factor for mortality in very elderly patients with pneumonia. Med. Clin. 2008, 131, 167–170. [Google Scholar] [CrossRef]
- Corrales-Medina, V.C.; Serpa, J.; Rueda, A.M.; Thomas, P.; Bozkurt, B.; Madjid, M.; Tweardy, D.; Musher, D.M. Acute Bacterial Pneumonia is Associated with the Occurrence of Acute Coronary Syndromes. Med. Clin. 2009, 88, 154–159. [Google Scholar] [CrossRef]
- Mandal, P.; Chalmers, J.D.; Choudhury, G.; Akram, A.R.; Hill, A.T. Vascular complications are associated with poor outcome in community-acquired pneumonia. QJM 2011, 104, 489–495. [Google Scholar] [CrossRef] [Green Version]
- Perry, T.W.; Pugh, M.J.V.; Waterer, G.W.; Nakashima, B.; Orihuela, C.J.; Copeland, L.A.; Marcos, I.; Anzueto, A.; Mortensen, E.M. Incidence of Cardiovascular Events After Hospital Admission for Pneumonia. Am. J. Med. 2012, 124, 244–251. [Google Scholar] [CrossRef] [Green Version]
- Corrales-Medina, V.F.; Musher, D.M.; Wells, G.A.; Chirinos, J.A.; Chen, L.; Fine, M.J. Cardiac Complications in Patients with Community-Acquired Pneumonia: Incidence, Timing, Risk Factors, and Association with Short-Term Mortality. Circulation 2012, 125, 773–781. [Google Scholar] [CrossRef] [Green Version]
- Viasus, D.; Garcia-Vidal, C.; Manresa, F. Risk stratification and prognosis of acute cardiac events in hospitalized adults with community-acquired pneumonia. J. Infect. 2013, 66, 27–33. [Google Scholar] [CrossRef]
- Griffin, A.T.; Wiemken, T.L.; Arnold, F.W. Risk factors for cardiovascular events in hospitalized patients with community-acquired pneumonia. Int. J. Infect. Dis. 2013, 17, e1125–e1129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aliberti, S.; Ramirez, J.; Cosentini, R.; Valenti, V.; Voza, A.; Rossi, P.; Stolz, D.; Legnani, D.; Pesci, A.; Richeldi, L.; et al. Acute myocardial infarction versus other cardiovascular events in community- acquired pneumonia. ERJ Open Res. 2015, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cangemi, R.; Romiti, F.; Rossi, E.; Ruscio, E.; Russo, A. Relation of Cardiac Complications In The Early Phase Of Community-Acquired Pneumonia To Long-Term Mortality And Cardiovascular Events. Am. J. Cardiol. 2015, 116, 647–651. [Google Scholar] [CrossRef] [PubMed]
- Corrales-Medina, V.F.; Alvarez, K.N.; Weissfeld, L.A.; Angus, D.C.; Chirinos, J.A.; Chang, C.H.; Newman, A.; Loehr, L.; Folsom, A.R.; Elkind, M.S.; et al. Association Between Hospitalization for Pneumonia and Subsequent Risk of Cardiovascular Disease. JAMA 2015, 313, 264–274. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.C.; Liao, W.I.; Wang, Y.C.; Chang, W.C.; Hsu, C.W.; Chen, Y.H.; Tsai, S.H. An Elevated Glycemic Gap is Associated with Adverse Outcomes in Diabetic Patients with Community-Acquired Pneumonia. Medicine 2015, 94, e1456. [Google Scholar] [CrossRef] [PubMed]
- Violi, F.; Cangemi, R.; Falcone, M.; Taliani, G.; Pieralli, F.; Vannucchi, V.; Nozzoli, C.; Venditti, M. Cardiovascular Complications and Short-term Mortality Risk in Community-Acquired Pneumonia. Clin. Infect. Dis. 2017, 64, 1486–1493. [Google Scholar] [CrossRef] [PubMed]
- Eurich, D.T.; Marrie, T.J. Risk of heart failure after community acquired pneumonia: Prospective controlled study with 10 years of follow-up. BMJ 2017, 413, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Cilli, A.; Cakin, O.; Aksoy, E.; Karakurt, Z.; Mersin, S.; Bozkurt, S.; Ciftci, F.; Cengiz, M.; Diseases, S.T.; Surgery, T.; et al. Acute cardiac events in severe community-acquired pneumonia: A multicenter study. Clin. Respir. J. 2018, 12, 2212–2219. [Google Scholar] [CrossRef]
- Postma, D.F.; Spitoni, C.; Van Werkhoven, C.H.; Van Elden, L.J.R.; Oosterheert, J.J.; Bonten, M.J.M. Cardiac events after macrolides or fluoroquinolones in patients hospitalized for community-acquired pneumonia: Post-hoc analysis of a cluster-randomized trial. BMC Infect. Dis. 2019, 19, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Pieralli, F.; Biondo, B.; Vannucchi, V.; Falcone, M.; Antonielli, E.; De Marzi, G.; Casati, C.; Maddaluni, L.; Nozzoli, C.; Olivotto, I. Performance of the CHA 2 DS 2-VASc score in predicting new onset atrial fibrillation during hospitalization for community-acquired pneumonia. Eur. J. Intern. Med. 2019, 62, 24–28. [Google Scholar] [CrossRef]
- Cangemi, R.; Calvieri, C.; Taliani, G.; Pignatelli, P.; Morelli, S.; Falcone, M.; Pastori, D.; Violi, F. Left Atrium Dilatation and Left Ventricular Hypertrophy Predispose to Atrial Fibrillation in Patients with Community-Acquired Pneumonia. Am. J. Cardiol. 2019, 124, 723–728. [Google Scholar] [CrossRef] [PubMed]
- Musher, D.M.; Abers, M.S.; Corrales-Medina, V.F. Acute Infection and Myocardial Infarction. N. Eng. J. Med. 2019, 380, 171–176. [Google Scholar] [CrossRef] [PubMed]
- McNeil, J.J.; Wolfe, R.; Woods, R.L.; Tonkin, A.M.; Donnan, G.A.; Nelson, M.R.; Reid, C.M.; Lockery, J.E.; Kirpach, B.; Storey, E.; et al. Effect of Aspirin on Cardiovascular Events and Bleeding in the Healthy Elderly. N. Engl. J. Med. 2018, 379, 1509–1518. [Google Scholar] [CrossRef] [PubMed]
- Gaziano, J.M.; Brotons, C.; Coppolecchia, R.; Cricelli, C.; Darius, H.; Gorelick, P.B.; Howard, G.; Pearson, T.A.; Rothwell, P.M.; Ruilope, L.M.; et al. Use of aspirin to reduce risk of initial vascular events in patients at moderate risk of cardiovascular disease (ARRIVE): A randomised, double-blind, placebo-controlled trial. Lancet 2018, 392, 1036–1046. [Google Scholar] [CrossRef]
- Falcone, M.; Russo, A.; Shindo, Y.; Farcomeni, A.; Pieralli, F.; Cangemi, R.; Liu, J.; Xia, J.; Okumura, J.; Sano, M.; et al. A Hypothesis-Generating Study of the Combination of Aspirin plus Macrolides in Patients with Severe Community-Acquired Pneumonia. Antimicrob. Agents Chem. 2019, 63, e01556-18. [Google Scholar] [CrossRef] [Green Version]
- Falcone, M.; Russo, A.; Cangemi, R.; Farcomeni, A.; Calvieri, C.; Barillà, F.; Scarpellini, M.G.; Bertazzoni, G.; Palange, P.; Taliani, G.; et al. Lower mortality rate in elderly patients with community-onset pneumonia on treatment with aspirin. J. Am. Heart Assoc. 2015, 4, e001595. [Google Scholar] [CrossRef] [Green Version]
- Sexton, T.R.; Zhang, G.; Macaulay, T.E.; Callahan, L.A.; Charnigo, R.; Vsevolozhskaya, O.A.; Li, Z.; Smyth, S. Ticagrelor Reduces Thromboinflammatory Markers in Patients with Pneumonia. JACC. Basic Transl. Sci. 2018, 3, 435–449. [Google Scholar] [CrossRef]
- Collaborators, C.T.T.; Mihaylova, B.; Emberson, J.; Blackwell, L.; Keech, A.; Simes, J.; Barnes, E.H.; Voysey, M.; Gray, A.; Collins, R.; et al. The effects of lowering LDL cholesterol with statin therapy in people at low risk of vascular disease: Meta-analysis of individual data from 27 randomised trials. Lancet 2012, 380, 581–590. [Google Scholar]
- Tralhão, A.F.R.; De Souza-Dantas, V.C.; Figueira Salluh, J.I.; Rodrigues Póvoa, P.M.S. Impact of statins in outcomes of septic patients: A systematic review. Postgrad. Med. 2014, 126, 45–58. [Google Scholar] [CrossRef]
- Papazian, L.; Roch, A.; Charles, P.-E.; Penot-Ragon, C.; Perrin, G.; Roulier, P.; Goutorbe, P.; Lefrant, J.-Y.; Wiramus, S.; Jung, B.; et al. Effect of Statin Therapy on Mortality in Patients with Ventilator-Associated Pneumonia: A Randomized Clinical TrialStatin Therapy and Mortality in Patients with VAP. JAMA 2013, 310, 1692–1700. [Google Scholar] [CrossRef]
- McAuley, D.F.; Laffey, J.G.; O’Kane, C.M.; Perkins, G.D.; Mullan, B.; Trinder, T.J.; Johnston, P.; Hopkins, P.A.; Johnston, A.J.; McDowell, C.; et al. Simvastatin in the Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2014, 371, 1695–1703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwartz, G.G.; Steg, P.G.; Szarek, M.; Bhatt, D.L.; Bittner, V.A.; Diaz, R.; Edelberg, J.M.; Goodman, S.G.; Hanotin, C.; Harrington, R.A.; et al. Alirocumab and Cardiovascular Outcomes after Acute Coronary Syndrome. N. Engl. J. Med. 2018, 379, 2097–2107. [Google Scholar] [CrossRef] [PubMed]
- Sabatine, M.S.; Giugliano, R.P.; Keech, A.C.; Honarpour, N.; Wiviott, S.D.; Murphy, S.A.; Kuder, J.F.; Wang, H.; Liu, T.; Wasserman, S.M.; et al. Evolocumab and Clinical Outcomes in Patients with Cardiovascular Disease. N. Engl. J. Med. 2017, 376, 1713–1722. [Google Scholar] [CrossRef] [PubMed]
- Berger, J.-M.; Loza Valdes, A.; Gromada, J.; Anderson, N.; Horton, J.D. Inhibition of PCSK9 does not improve lipopolysaccharide-induced mortality in mice. J. Lipid Res. 2017, 58, 1661–1669. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, A.; Good, C.; Downs, J.R.; Fine, M.J.; Pugh, M.J.V.; Anzueto, A.; Mortensen, E.M. The Association of Cardioprotective Medications with Pneumonia-Related Outcomes. PLoS ONE 2014, 9, e85797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stern, A.; Skalsky, K.; Avni, T.; Carrara, E.; Leibovici, L.; Paul, M. Corticosteroids for pneumonia. Cochrane Database Syst. Rev. 2017, 12, CD007720. [Google Scholar] [CrossRef]
- Briel, M.; Spoorenberg, S.M.C.; Snijders, D.; Torres, A.; Fernandez-Serrano, S.; Meduri, G.U.; Gabarrús, A.; Blum, C.A.; Confalonieri, M.; Kasenda, B.; et al. Corticosteroids in Patients Hospitalized with Community-Acquired Pneumonia: Systematic Review and Individual Patient Data Meta-analysis. Clin. Infect. Dis. 2017, 66, 346–354. [Google Scholar] [CrossRef] [Green Version]
- Cangemi, R.; Falcone, M.; Taliani, G.; Calvieri, C.; Tiseo, G.; Romiti, G.F.; Bertazzoni, G.; Farcomeni, A.; Violi, F.; The SIXTUS Study Group. Corticosteroid Use and Incident Myocardial Infarction in Adults Hospitalized for Community-acquired Pneumonia. Ann. Am. Thorac. Soc. 2019, 16, 91–98. [Google Scholar] [CrossRef]
- Ridker, P.M.; Everett, B.M.; Thuren, T.; MacFadyen, J.G.; Chang, W.H.; Ballantyne, C.; Fonseca, F.; Nicolau, J.; Koenig, W.; Anker, S.D.; et al. Antiinflammatory Therapy with Canakinumab for Atherosclerotic Disease. N. Engl. J. Med. 2017, 377, 1119–1131. [Google Scholar] [CrossRef]
- Eurich, D.T.; Marrie, T.J.; Violi, F.; Cangemi, R.; Falcone, M.; Taliani, G.; Pieralli, F.; Vannucchi, V.; Nozzoli, C.; Venditti, M.; et al. The Efficacy of Influenza Vaccine in Elderly Persons: A Meta-Analysis and Review of the Literature. Ann. Intern. Med. 2017, 45, 518–527. [Google Scholar]
- Udell, J.A.; Zawi, R.; Bhatt, D.L.; Keshtkar-jahromi, M.; Gaughran, F.; Phrommintikul, A.; Ciszewski, A. Association Between Influenza Vaccination and Cardiovascular Outcomes in High-Risk Patients a Meta-analysis. JAMA 2013, 310, 1711–1720. [Google Scholar] [CrossRef] [PubMed]
- Ren, S.; Newby, D.; Li, S.C.; Walkom, E.; Miller, P.; Hure, A.; Attia, J. Effect of the adult pneumococcal polysaccharide vaccine on cardiovascular disease: A systematic review and meta-analysis. Open Heart 2015, 2, e000247. [Google Scholar] [CrossRef] [PubMed]
- Vardeny, O.; Claggett, B.; Udell, J.A.; Packer, M.; Zile, M.; Rouleau, J.; Swedberg, K.; Desai, A.S.; Lefkowitz, M.; Shi, V.; et al. Influenza Vaccination in Patients with Chronic Heart Failure: The PARADIGM-HF Trial. JACC Heart Fail. 2016, 4, 152–158. [Google Scholar] [CrossRef]
- Ray, W.A.; Murray, K.T.; Hall, K.; Arbogast, P.G.; Stein, C.M. Azithromycin and the risk of cardiovascular death. N. Engl. J. Med 2012, 36, 1881–1890. [Google Scholar] [CrossRef]
- Schembri, S.; Williamson, P.A.; Short, P.M.; Singanayagam, A.; Akram, A.; Taylor, J.; Singanayagam, A.; Hill, A.T.; Chalmers, J.D. Cardiovascular events After clarithromycin use in lower respiratory tract infections: Analysis of two prospective cohort studies. BMJ 2013, 346, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collins, S.D. Excess Mortality from Causes Other than Influenza and Pneumonia during Influenza Epidemics. Public Health Rep. (1896–1970) 1932, 47, 2159–2179. [Google Scholar] [CrossRef]
- Yende, S.; Angelo, G.D.; Mayr, F.; Kellum, J.A.; Weissfeld, L.; Murat, A.; Young, T.; Irani, K.; Angus, D.C.; Investigators, G. Elevated Hemostasis Markers after Pneumonia Increases One-Year Risk of All-Cause and Cardiovascular Deaths. PLoS ONE 2011, 6, e2284. [Google Scholar] [CrossRef] [Green Version]
- Warren-Gash, C.; Hayward, A.C.; Hemingway, H.; Denaxas, S.; Thomas, S.L.; Timmis, A.D.; Whitaker, H.; Smeeth, L. Influenza Infection and Risk of Acute Myocardial Infarction in England and Wales: ACALIBER Self-Controlled Case Series Study. J. Infect. Dis. 2012, 206, 1652–1659. [Google Scholar] [CrossRef] [Green Version]
- Jafarzadeh, S.R.; Thomas, B.S.; Warren, D.K.; Gill, J.; Fraser, V.J. Longitudinal Study of the Effects of Bacteremia and Sepsis on 5-year Risk of Cardiovascular Events. Clin. Infect. Dis. 2016, 63, 495–500. [Google Scholar] [CrossRef] [Green Version]
- Warren-Gash, C.; Blackburn, R.; Whitaker, H.; Mcmenamin, J.; Hayward, A.C. Laboratory-confirmed respiratory myocardial infarction and stroke: A self-controlled case series analysis of national linked datasets from Scotland. Eur. Respir. J. 2018, 51, 1701794. [Google Scholar] [CrossRef]
- Yeh, J.; Lin, C.; Kao, C. Relationship between pneumonia and cardiovascular diseases: A retrospective cohort study of the general population. Eur. J. Intern. Med. 2019, 59, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Corrales-Medina, V.F.; Suh, K.N.; Rose, G.; Chirinos, J.A.; Doucette, S.; Cameron, D.W.; Fergusson, D.A. Cardiac complications in patients with community-acquired pneumonia: A systematic review and meta-analysis of observational studies. PLoS Med. 2011, 8, e1001048. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reynolds, K.; Go, A.S.; Leong, T.K.; Boudreau, D.M.; Bushrow, A.E.C.; Fortmann, S.P.; Goldberg, R.J.; Gurwitz, J.H.; Magid, D.J.; Margolis, K.L.; et al. Trends in Incidence of Hospitalized Acute Myocardial Infarction in the Cardiovascular Research Network (CVRN). Am. J. Med. 2017, 130, 317–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conrad, N.; Judge, A.; Tran, J.; Mohseni, H.; Hedgecott, D.; Crespillo, A.P.; Allison, M.; Hemingway, H.; Cleland, J.G.; McMurray, J.J.V.; et al. Temporal trends and patterns in heart failure incidence: A population-based study of 4 million individuals. Lancet 2018, 391, 572–580. [Google Scholar] [CrossRef] [Green Version]
- Schnabel, R.B.; Yin, X.; Gona, P.; Larson, M.G.; Beiser, A.S.; McManus, D.D.; Newton-Cheh, C.; Lubitz, S.A.; Magnani, J.W.; Ellinor, P.T.; et al. 50 year trends in atrial fibrillation prevalence, incidence, risk factors, and mortality in the Framingham Heart Study: A cohort study. Lancet 2015, 386, 154–162. [Google Scholar] [CrossRef] [Green Version]
- García-Suárez, M.D.M.; Flórez, N.; Astudillo, A.; Vázquez, F.; Villaverde, R.; Fabrizio, K.; Pirofski, L.-A.; Méndez, F.J. The role of pneumolysin in mediating lung damage in a lethal pneumococcal pneumonia murine model. Respir. Res. 2007, 8, 3. [Google Scholar] [CrossRef] [Green Version]
- Feldman, C.; Munro, N.C.; Jeffery, P.K.; Mitchell, T.J.; Andrew, P.W.; Boulnois, G.J.; Guerreiro, D.; Rohde, J.A.; Todd, H.C.; Cole, P.J. Pneumolysin induces the salient histologic features of pneumococcal infection in the rat lung in vivo. Am. J. Respir. Cell Mol. Biol. 1991, 5, 416–423. [Google Scholar] [CrossRef]
- Feldman, C.; Anderson, R. Prevalence, pathogenesis, therapy, and prevention of cardiovascular events in patients with community-acquired pneumonia. Pneumonia 2016, 8, 11. [Google Scholar] [CrossRef] [Green Version]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| - | Year | Country | Study Type | Setting | n | CV Events a (%) | ACS b (%) | Heart Failure (%) | Stroke c (%) | Arrhythmias d (%) |
|---|---|---|---|---|---|---|---|---|---|---|
| Allen et al. [28] | 1984 | Zambia | Retrospective single center | Inpatients | 502 | - | - | - | - | 0.40 |
| Esposito et al. [29] | 1984 | USA | Prospective single center | Inpatients | 38 | - | - | 7.9 | - | - |
| Marrie et al. [30] | 1989 | Canada | Prospective single center | Inpatients | 583 | - | - | 11 | - | - |
| Ortqvist et al. [31] | 1990 | Sweden | Prospective, single center | Inpatients | 277 | 13 | - | - | - | - |
| Venkatesan et al. [32] | 1990 | UK | Prospective single center | Inpatients | 73 | - | - | - | - | 11 |
| Fine et al. [33] | 1990 | USA | Prospective single center | Low-risk e inpatients Outpatients | 170 | - | 0.6 | - | - | 0.6 |
| Woodhead et al. [34] | 1992 | UK | Retrospective multicenter | High-risk f inpatients | 72 | - | - | - | - | 23 |
| Leroy et al. [35] | 1995 | France | Retrospective single center | High-risk f inpatients | 299 | 2.3 | - | - | - | - |
| Janssens et al. [36] | 1995 | Switzerland | Prospective, single center | Inpatients | 99 | - | - | 33 | - | - |
| Musher et al. [37] | 2000 | USA | Prospective single center | Inpatients | 100 | - | - | 4.0 | - | - |
| Férnandez-Sabé et al. [38] | 2003 | Spain | Prospective single center | Inpatients | 1474 | - | - | 7.2 | - | - |
| Fine et al. [39] | 2003 | USA | Prospective multicenter | Inpatients | 608 | 22 | - | - | - | - |
| Martínez-Moragón et al. [40] | 2004 | Spain | Prospective single-center | Inpatients | 91 | 5.0 | - | - | - | - |
| Menéndez et al. [41] | 2004 | Spain | Prospective multicenter | Low-risk e inpatients | 1424 | - | - | 8.7 | - | - |
| Querol-Ribelles et al. [42] | 2005 | Spain | Prospective single-center | Low-risk e inpatients | 459 | - | - | 8.6 | - | - |
| Díaz et al. [43] | 2005 | Chile | Prospective Single-center | High-risk f inpatients | 113 | - | - | 24 | - | 15 |
| Marrie et al. [44] | 2005 | Canada | Prospective single center | Low-risk e inpatients | 586 | - | 0.3 | 1.4 | - | - |
| McAlister et al. [45] | 2005 | Canada | Prospective multicenter | Low-risk e inpatients | 2471 | 5.9 | - | - | - | - |
| O’Meara et al. [46] | 2005 | USA | Prospective multicenter | Inpatients | 582 | 24 | - | - | - | - |
| Musher et al. [47] | 2007 | USA | Retrospective single-center | Inpatients g | 170 | 19 | 7 | 15 | - | 6 |
| Becker et al. [48] | 2007 | Canada | Retrospective multicenter | Inpatients | 391 | 17 | 8 | 12 | - | 3 |
| Ramirez et al. [49] | 2008 | Spain | Retrospective single-center | Inpatients | 500 | - | 5.8 | - | - | - |
| Cabré et al. [50] | 2008 | Spain | Prospective single-center | Inpatients | 117 | - | 0.9 | 12 | - | 4.4 |
| Corrales-Medina et al. [51] | 2009 | USA | Retrospective single-center | Inpatients | 206 | - | 11 | - | - | - |
| Mandal et al. [52] | 2011 | Scotland | Retrospective multicenter | Inpatients | 5034 | - | 5.0 | - | 2.2 | 9.3 |
| Perry et al. [53] | 2011 | USA | Retrospective multicenter | Inpatients | 50119 | - | 2.3 | 9.1 | 0.1 | 8.4 |
| Corrales-Medina et al. [54] | 2012 | USA and Canada | Prospective multicenter | Inpatients Outpatients | 1343 944 | 27 2.1 | 3.6 0 | 67 65 | - | 22 35 |
| Viasus et al. [55] | 2013 | Spain | Prospective single center | Low-risk inpatients High-risk inpatients f | 1621h 2300 | 3.0 11.6 | 0.76 | 3.0 | - | 5.1 |
| Griffin et al. [56] | 2013 | 13 countries | Retrospective multicenter | Inpatients | 3068 | 14 | 1.3 | 2.1 | - | 3.6 |
| Aliberti et al. [57] | 2015 | Italy, Switzerland | Retrospective multicenter | Inpatients | 905 | - | 2.3 | 3.7 | 1.1 | 19 |
| Cangemi et al. [58] | 2015 | Italy | Prospective, single center | Inpatients | 301 | 18 | 11 | - | - | 10 |
| Corrales-Medina et al. [59] | 2015 | USA | Retrospective multicenter | Inpatients | 508 | 11 | - | - | - | - |
| Corrales-Medina et al. [59] | 2015 | USA | Retrospective multicenter | Inpatients | 426 | 0.90 | - | - | - | - |
| Chen et al. [60] | 2015 | Taiwan | Single-center retrospective | Inpatients | 746 | - | 2.3 | - | - | - |
| Violi et al. [61] | 2017 | Italy, Canada | Prospective multicenter | Low-risk inpatients High-risk inpatients f | 355 h 827 | 12 41 | 8.4 | 24 | 0.1 | 9.2 |
| Eurich et al. [62] | 2017 | Canada | Prospective multicenter | Inpatients Outpatients | 4988 | - | - | 12 | - | - |
| Cilli et al. [63] | 2018 | Turkey | Retrospective multicenter | High-risk f inpatients | 373 | 15 | 0.54 | 2.9 | - | 12 |
| Postma et al. [64] | 2019 | Netherlands | Retrospective multicenter | Inpatients | 2107 | 7.9 | 0.7 | 4.8 | - | 2.5 |
| Pieralli et al. [65] | 2019 | Italy | Retrospective single-center | Inpatients | 468 | - | - | - | - | 10.3 |
| Cangemi et al. [66] | 2019 | Italy | Prospective single center | Inpatients | 545 | - | - | - | - | 9.5 |
| Author | Year | n with Event | Outcome | Independent Predictors |
|---|---|---|---|---|
| Corrales-Medina et al. [51] | 2009 | 206 | ACS | Age Congestive heart failure |
| Mandal et al. [52] | 2011 | 252 | ACS | Age ≥ 65 Previous MI COPD Chronic kidney disease |
| 468 | Arrhythmias | Age Previous MI Diabetes | ||
| 111 | Stroke | Prior stroke COPD | ||
| Perry et al. [53] | 2011 | 2002 | CHF | Age Admission to ICU Previous MI COPD Diabetes Chronic kidney disease Cancer |
| 2732 | Arrhythmias | Age Admission to ICU | ||
| Corrales-Medina et al. [54] | 2012 | 378 | Overall cardiac complications | Age Nursing home Hypertension Previous CAD Previous arrhythmias Previous CHF RR ≥ 30/min pH < 7.35 BUN ≥ 30 mg/dL Sodium < 130 mmol/L Hematocrit < 30% Pleural effusion Inpatient |
| Viasus et al. [55] | 2013 | 315 | Overall cardiac complications | Age ≥ 65 Chronic heart disease Septic shock Tachycardia Albumin < 3 g/dL Multilobar pneumonia Streptococcal pneumonia |
| Griffin et al. [56] | 2013 | 376 | Overall cardiac complications | Hyperlipidemia Statin therapy 1 Staphylococcus aureus Klebsiella pneumoniae PSI |
| Aliberti et al. [57] | 2015 | 21 | ACS | Female sex Severe sepsis Liver disease |
| Cangemi et al. [58] | 2015 | 55 | Overall cardiac complications | Age Hypertension Diabetes Baseline troponin |
| Violi et al. [61] | 2017 | 308 | Overall cardiac complications | Age CHF PSI |
| Cilli et al. [63] | 2018 | 56 | Overall cardiac complications | Age Hypoalbuminemia Diuretic Vasopressor Haloperidol |
| Postma et al. [64] | 2019 | 2107 | Overall cardiac complications | Erythromycin use |
| Pieralli et al. [65] | 2019 | 468 | Atrial fibrillation | CURB-65 > 2 CHA2DS2-VASc > 3 |
| Cangemi et al. [66] | 2019 | 545 | Atrial fibrillation | Prior paroxysmal AF, Enlarged LAAi Left ventricular hypertrophy |
| Study | Year | Event | Mortality | Measure of Risk |
|---|---|---|---|---|
| Mandal et al. [52] | 2001 | Stroke | 90-day | OR 1.79 (1.51–2.12), p < 0.0001 |
| MI | OR 2.93 (1.60–2.33), p < 0.0001 | |||
| AF | OR 1.39 (1.65–2.19), p < 0.0001 | |||
| Corrales-Medina et al. [54] | 2012 | Overall cardiac complications | 30-day | OR 1.6 (1.04–2.5), p < 0.001 |
| Viasus et al. [55] | 2013 | Overall cardiac complications | 30-day | OR 2.18 (1.38–3.42) |
| Aliberti et al. [57] | 2015 | ACS | In-hospital | OR 3.57 (1.32–9.69), p = 0.02 |
| Other events | OR 2.63 (1.43–4.84), p = NS | |||
| Cangemi et al. [58] | 2015 | Overall cardiac complications | 6-60 months | OR 1.759 (1.099–2.816), p = 0.019 |
| Violi et al. [61] | 2017 | Overall cardiac complications | 30-day | HR 5.49, p < 0.001 |
| Cilli et al. [63] | 2018 | Overall cardiac complications | In-hospital | OR 2.18 (1.03–4.61), p = 0.04 |
| 90-day | NS |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tralhão, A.; Póvoa, P. Cardiovascular Events after Community-Acquired Pneumonia: A Global Perspective with Systematic Review and Meta-Analysis of Observational Studies. J. Clin. Med. 2020, 9, 414. https://doi.org/10.3390/jcm9020414
Tralhão A, Póvoa P. Cardiovascular Events after Community-Acquired Pneumonia: A Global Perspective with Systematic Review and Meta-Analysis of Observational Studies. Journal of Clinical Medicine. 2020; 9(2):414. https://doi.org/10.3390/jcm9020414
Chicago/Turabian StyleTralhão, António, and Pedro Póvoa. 2020. "Cardiovascular Events after Community-Acquired Pneumonia: A Global Perspective with Systematic Review and Meta-Analysis of Observational Studies" Journal of Clinical Medicine 9, no. 2: 414. https://doi.org/10.3390/jcm9020414