Results of PCI with Drug-Eluting Stents in an All-Comer Population Depending on Vessel Diameter

 , , and
, , and
Abstract
:1. Introduction
2. Experimental Section
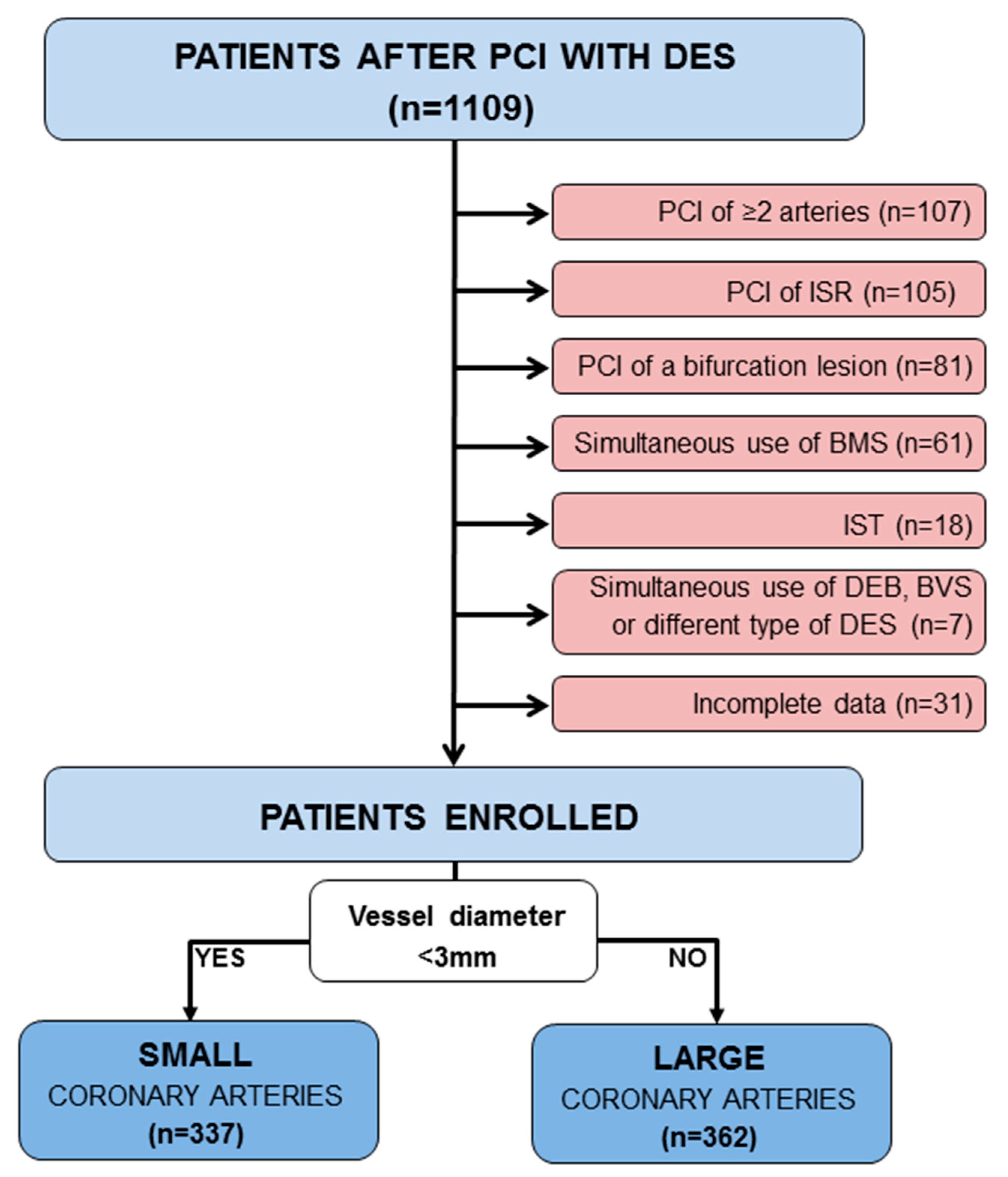
2.1. Study Design
2.2. Coronary Stenting
2.3. Follow-Up
2.4. Statistics
3. Results
3.1. Study Population
3.2. Clinical Characteristics
3.3. Procedural Characteristics
3.4. Follow-Up
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Morice, M.C.; Serruys, P.W.; Sousa, J.E.; Fajadet, J.; Ban Hayashi, E.; Perin, M.; Molnar, F. A randomized comparison of a sirolimus-eluting stent with a standard stent for coronary revascularization. N. Engl. J. Med. 2002, 346, 1773–1780. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moses, J.W.; Leon, M.B.; Popma, J.J.; Fitzgerald, P.J.; Holmes, D.R.; O’Shaughnessy, C.; Jaeger, J.L. Sirolimus-eluting stents versus standard stents in patients with stenosis in a native coronary artery. N. Engl. J. Med. 2003, 349, 1315–1323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stone, G.W.; Lansky, A.J.; Pocock, S.J.; Gersh, B.J.; Dangas, G.; Wong, S.C.; Dudek, D. Paclitaxel-eluting stents versus bare-metal stents in acute myocardial infarction. N. Engl. J. Med. 2009, 360, 1946–1959. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stone, G.W.; Moses, J.W.; Ellis, S.G.; Schofer, J.; Dawkins, K.D.; Morice, M.C.; Cutlip, D.E. Safety and efficacy of sirolimus- and paclitaxel-eluting coronary stents. N. Engl. J. Med. 2007, 356, 998–1008. [Google Scholar] [CrossRef] [PubMed]
- Lagerqvist, B.; James, S.K.; Stenestrand, U.; Lindbäck, J.; Nilsson, T.; Wallentin, L. Long-term outcomes with drug-eluting stents versus bare-metal stents in Sweden. N. Engl. J. Med. 2007, 356, 1009–1019. [Google Scholar] [CrossRef]
- Mauri, L.; Hsieh, W.H.; Massaro, J.M.; Ho, K.K.; D’Agostino, R.; Cutlip, D.E. Stent thrombosis in randomized clinical trials of drug-eluting stents. N. Engl. J. Med. 2007, 356, 1020–1029. [Google Scholar] [CrossRef]
- Nordmann, A.J.; Briel, M.; Bucher, H.C. Mortality in randomized controlled trials comparing drug-eluting vs. bare metal stents in coronary artery disease: A meta-analysis. Eur. Heart J. 2006, 27, 2784–2814. [Google Scholar] [CrossRef] [Green Version]
- Pfisterer, M.; Brunner-La Rocca, H.P.; Buser, P.T.; Rickenbacher, P.; Hunziker, P.; Mueller, C. Basket-Late Investigators. Late clinical events after clopidogrel discontinuation may limit the benefit of drug-eluting stents: An observational study of drug-eluting versus bare-metal stents. J. Am. Coll. Cardiol. 2006, 48, 2584–2591. [Google Scholar] [CrossRef] [Green Version]
- Stettler, C.; Wandel, S.; Allemann, S.; Kastrati, A.; Morice, M.C.; Schömig, A.; Goy, J.J. Outcomes associated with drug-eluting and bare-metal stents: A collaborative network meta-analysis. Lancet 2007, 370, 937–948. [Google Scholar] [CrossRef]
- Palmerini, T.; Biondi-Zoccai, G.; Della Riva, D.; Stettler, C.; Sangiorgi, D.; D’Ascenzo, F.; De Waha, A. Stent thrombosis with drug-eluting and bare-metal stents: Evidence from a comprehensive network meta-analysis. Lancet 2012, 379, 1393–1402. [Google Scholar] [CrossRef]
- Stefanini, G.G.; Baber, U.; Windecker, S.; Morice, M.C.; Sartori, S.; Leon, M.B.; Camenzind, E. Safety and efficacy of drug-eluting stents in women: A patient-level pooled analysis of randomised trials. Lancet 2013, 382, 1879–1888. [Google Scholar] [CrossRef]
- Stefanini, G.G.; Byrne, R.A.; Serruys, P.W.; de Waha, A.; Meier, B.; Massberg, S.; Kastrati, A. Biodegradable polymer drug-eluting stents reduce the risk of stent thrombosis at 4 years in patients undergoing percutaneous coronary intervention: A pooled analysis of individual patient data from the ISAR-TEST 3, ISAR-TEST 4, and LEADERS randomized trials. Eur. Heart J. 2012, 33, 1214–1222. [Google Scholar] [PubMed] [Green Version]
- Stefanini, G.G.; Kalesan, B.; Serruys, P.W.; Heg, D.; Buszman, P.; Linke, A.; Morice, M.C. Long-term clinical outcomes of biodegradable polymer biolimus-eluting stents versus durable polymer sirolimus-eluting stents in patients with coronary artery disease (LEADERS): 4 year follow-up of a randomised non-inferiority trial. Lancet 2011, 378, 1940–1948. [Google Scholar] [CrossRef] [Green Version]
- Kaiser, C.; Brunner-La Rocca, H.P.; Buser, P.T.; Bonetti, P.O.; Osswald, S.; Linka, A.; Pfisterer, M.E. Incremental cost-effectiveness of drug-eluting stents compared with a third-generation bare-metal stent in a real-world setting: Randomised Basel Stent Kosten Effektivitats Trial (BASKET). Lancet 2005, 366, 921–929. [Google Scholar] [CrossRef]
- Pfisterer, M.; Brunner-La Rocca, H.P.; Rickenbacher, P.; Hunziker, P.; Mueller, C.; Nietlispach, F.; Kaiser, C. Long-term benefit-risk balance of drug-eluting vs. bare-metal stents in daily practice: Does stent diameter matter? Three-year follow-up of BASKET. Eur. Heart J. 2009, 30, 16–24. [Google Scholar] [CrossRef] [Green Version]
- Tcheng, J.E.; Lim, I.H.; Srinivasan, S.; Jozic, J.; Gibson, C.M.; O’Shea, J.C.; Simon, D.I. Stent parameters predict major adverse clinical events and the response to platelet glycoprotein IIb/IIIa blockade: Findings of the ESPRIT trial. Circ. Cardiovasc. Interv. 2009, 2, 43–51. [Google Scholar] [CrossRef] [Green Version]
- Cortese, B.; Bertoletti, A.; De Matteis, S.; Danzi, G.B.; Kastrati, A. Drug-eluting stents perform better than bare metal stents in small coronary vessels: A meta-analysis of randomised and observational clinical studies with mid-term follow up. Int. J. Cardiol. 2012, 161, 73–82. [Google Scholar] [CrossRef]
- Parikh, S.V.; Luna, M.; Selzer, F.; Marroquin, O.C.; Mulukutla, S.R.; Abbott, J.D.; Holper, E.M. Outcomes of small coronary artery stenting with bare-metal stents versus drug-eluting stents: Results from the NHLBI Dynamic Registry. Catheter Cardiovasc. Interv. 2014, 83, 192–200. [Google Scholar] [CrossRef] [Green Version]
- Puymirat, E.; Mangiacapra, F.; Peace, A.; Sharif, F.; Conte, M.; Bartunek, J.; Barbato, E. Long-term clinical outcome in patients with small vessel disease treated with drug-eluting versus bare-metal stenting. Am. Heart J. 2011, 162, 907–913. [Google Scholar] [CrossRef]
- Elezi, S.; Kastrati, A.; Neumann, F.J.; Hadamitzky, M.; Dirschinger, J.; Schömig, A. Vessel size and long-term outcome after coronary stent placement. Circulation 1998, 98, 1875–1880. [Google Scholar] [CrossRef] [Green Version]
- Schunkert, H.; Harrell, L.; Palacios, I.F. Implications of small reference vessel diameter in patients undergoing percutaneous coronary revascularization. J. Am. Coll. Cardiol. 1999, 34, 40–48. [Google Scholar] [CrossRef] [Green Version]
- Kuramitsu, S.; Ohya, M.; Shinozaki, T.; Otake, H.; Horie, K.; Kawamoto, H.; Ando, K. Risk Factors and Long-Term Clinical Outcomes of Second-Generation Drug-Eluting Stent Thrombosis. Circ. Cardiovasc. Interv. 2019, 12, e007822. [Google Scholar] [CrossRef] [PubMed]
- Stoicescu, C.; Vintila, V.; Udroiu, C.; Florescu, N.; Dawood, A.; Cinteza, M.; Vinereanu, D. Outcome and Predictors of Stent Thrombosis in the First Romanian Registry of Drug Eluting Stent (RODESINO EXTENSION). Maedica 2013, 8, 153–163. [Google Scholar] [PubMed]
- Claessen, B.E.; Smits, P.C.; Kereiakes, D.J.; Parise, H.; Fahy, M.; Kedhi, E.; Sood, P. Impact of lesion length and vessel size on clinical outcomes after percutaneous coronary intervention with everolimus-versus paclitaxel-eluting stents pooled analysis from the SPIRIT (Clinical Evaluation of the XIENCE V Everolimus Eluting Coronary Stent System) and COMPARE (Second-generation everolimus-eluting and paclitaxel-eluting stents in real-life practice) Randomized Trials. JACC Cardiovasc. Interv. 2011, 4, 1209–1215. [Google Scholar]
- Mauri, L.; Orav, E.J.; O’Malley, A.J.; Moses, J.W.; Leon, M.B.; Holmes, D.R., Jr.; Kereiakes, D.J. Relationship of late loss in lumen diameter to coronary restenosis in sirolimus-eluting stents. Circulation 2005, 111, 321–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stone, G.W.; Midei, M.; Newman, W.; Sanz, M.; Hermiller, J.B.; Williams, J.; Sood, P. Comparison of an everolimus-eluting stent and a paclitaxel-eluting stent in patients with coronary artery disease: A randomized trial. JAMA 2008, 299, 1903–1913. [Google Scholar] [CrossRef]
- Van Der Heijden, L.C.; Kok, M.M.; Danse, P.W.; Schramm, A.R.; Hartmann, M.; Löwik, M.M.; von Birgelen, C. Small-vessel treatment with contemporary newer-generation drug-eluting coronary stents in all-comers: Insights from 2-year DUTCH PEERS (TWENTE II) randomized trial. Am. Heart J. 2016, 176, 28–35. [Google Scholar] [CrossRef]
- Jolly, S.S.; Cairns, J.A.; Yusuf, S.; Meeks, B.; Pogue, J.; Rokoss, M.J.; Gershlick, A. Randomized trial of primary PCI with or without routine manual thrombectomy. N. Engl. J. Med. 2015, 372, 1389–1398. [Google Scholar] [CrossRef] [Green Version]
- Levine, G.N.; Bates, E.R.; Blankenship, J.C.; Bailey, S.R.; Bittl, J.A.; Cercek, B.; Chambers, C.E.; Ellis, S.G.; Guyton, R.A.; Hollenberg, S.M.; et al. 2015 ACC/AHA/SCAI Focused Update on Primary Percutaneous Coronary Intervention for Patients With ST-Elevation Myocardial Infarction: An Update of the 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention and the 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction. J. Am. Coll. Cardiol. 2016, 67, 1235–1250. [Google Scholar]
- Marmagkiolis, K.; Hakeem, A.; Cilingiroglu, M.; Feldman, D.N.; Charitakis, K. Efficacy and safety of routine aspiration thrombectomy during primary PCI for ST-segment elevation myocardial infarction: A meta-analysis of large randomized controlled trials. Hell. J. Cardiol. 2018, 59, 168–173. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 699) | Large Vessels (n = 362) | Small Vessels (n = 337) | p Value 1 | |
|---|---|---|---|---|
| Male sex | 437 (63%) | 232 (64%) | 205 (61%) | 0.39 |
| Age [years] | 65 (58;72) | 65 (58;72) | 64 (58;72) | 0.95 |
| Risk Factors for coronary artery disease | ||||
| Obesity | 281 (40%) | 159 (44%) | 122 (36%) | 0.045 |
| Hypertension | 574 (82%) | 293 (81%) | 281 (83%) | 0.43 |
| Diabetes mellitus | 298 (43%) | 153 (42%) | 145 (43%) | 0.88 |
| Dyslipidemia | 503 (72%) | 265 (73%) | 238 (71%) | 0.45 |
| Smoking | 292 (42%) | 160 (44%) | 132 (39%) | 0.19 |
| Familial History of CAD | 189 (27%) | 97 (27%) | 92 (27%) | 0.93 |
| Comorbidities | ||||
| Coronary artery disease | 16 (2.3%) | 6 (1.7%) | 10 (3.0%) | 0.31 |
| Peripheral artery disease | 55 (7.9%) | 22 (6.1%) | 33 (9.8%) | 0.09 |
| Chronic renal disease | 88 (13%) | 44 (12%) | 44 (13%) | 0.73 |
| Prior AMI | 180 (26%) | 82 (23%) | 98 (29%) | 0.06 |
| Prior PCI | 239 (34%) | 117 (32%) | 122 (36%) | 0.30 |
| Prior CABG | 35 (5.0%) | 15 (4.1%) | 20 (5.9%) | 0.30 |
| Diagnosis | ||||
| STEMI | 49 (7.0) | 26 (7.2%) | 23 (6.8%) | 0.88 |
| NSTEMI | 189 (27%) | 97 (27%) | 92 (27%) | 0.93 |
| Unstable angina | 165 (24%) | 93 (26%) | 72 (21%) | 0.18 |
| LVEF ≤30% | 80 (11%) | 35 (9.7%) | 45 (13%) | 0.15 |
| All Patients (n = 699) | Large Vessels (n = 362) | Small Vessels (n = 337) | p Value 1 | |
|---|---|---|---|---|
| Angiographic characteristics | ||||
| ACC/AHA lesion B2-C | 377 (55) | 199 (55) | 178 (53) | 0.86 |
| Stenosis severity [%] | 80 (70;95) | 80 (70;95) | 90 (70;95) | 0.005 |
| Significant calcification | 75 (11) | 38 (11) | 37 (11) | 0.90 |
| Ostial lesion | 46 (6.6) | 27 (7.5) | 19 (5.6) | 0.36 |
| Thrombus | 30 (4.3) | 18 (5.0) | 12 (3.6) | 0.46 |
| Multivessel disease | 345 (49) | 174 (48) | 171 (51) | 0.50 |
| Procedural characteristics | ||||
| DES 2 | 451 (65) | 218 (60) | 233 (69) | 0.014 |
| Stented artery | ||||
| LM | 22 (3.1) | 22 (6.1) | 0 (0) | <0.001 |
| LAD | 331 (47) | 180 (50) | 151 (45) | 0.20 |
| Cx | 124 (18) | 47 (13) | 77 (23) | 0.001 |
| RCA | 183 (26) | 109 (30) | 74 (22) | 0.02 |
| Bypass | 2 (0.3) | 2 (0.6) | 0 (0) | 0.50 |
| Number of DESs per lesion | <0.001 | |||
| 1 | 576 (82) | 316 (87) | 260 (77) | |
| 2 | 106 (15) | 41 (11) | 65 (19) | |
| 3 | 14 (2.0) | 5 (1.4) | 9 (2.7) | |
| 4 | 3 (0.4) | 0 (0) | 3 (0.9) | |
| DES length per lesion [mm] | 22 (15;29) | 22 (15;29) | 22 (15;30) | 0.036 |
| DES diameter [mm] | 3.0 (2.5;3.25) | 3.25 (3.0;3.5) | 2.5 (2.25;2.75) | <0.001 |
| Primary PCI | 402 (58) | 212 (59) | 190 (56) | 0.59 |
| Predilatation | 376 (54) | 164 (45) | 212 (63) | <0.001 |
| Dilatation pressure [atm] | 12 (12;16) | 14 (12;16) | 12 (12;14) | 0.001 |
| TIMI 3 flow post PCI | 632 (90) | 329 (91) | 303 (90) | 0.70 |
| GPIIb/IIIa inhibitors | 47 (6.7) | 27 (7.5) | 20 (5.9) | 0.45 |
| Thrombectomy | 15 (2.1) | 8 (2.2) | 7 (2.1) | 1.0 |
| Residual stenosis >10% | 20 (2.9) | 10 (2.8) | 10 (3.0) | 1.0 |
| Total Population, n = 699 | Large Vessels, n = 362 | Small Vessels, n = 337 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Small Vessels n = 337 | Large Vessels n = 362 | p Value | DES 1 n = 144 | DES 2 n = 218 | p Value | DES 1 n = 104 | DES 2 n = 233 | p Value | |
| Efficacy | |||||||||
| MACCE | 68 (20%) | 50 (14%) | 0.025 | 30 (21%) | 20 (9.2%) | 0.002 | 27 (26%) | 41 (18%) | 0.08 |
| Death | 13 (3.9%) | 6 (1.7%) | 0.074 | 3 (2.1%) | 3 (1.4%) | 0.67 | 7 (6.7%) | 6 (2.6%) | 0.07 |
| Non-fatal AMI | 31 (9.2%) | 29 (8.0%) | 0.58 | 16 (11%) | 13 (6.0%) | 0.08 | 12 (12%) | 19 (8.2%) | 0.32 |
| Re-PCI (TVR) | 34 (10%) | 34 (9.4%) | 0.76 | 21 (15%) | 13 (6.0%) | 0.006 | 13 (13%) | 21 (9.0%) | 0.33 |
| Stroke | 12 (3.6%) | 5 (1.4%) | 0.062 | 4 (2.8%) | 1 (0.5%) | 0.08 | 4 (3.8%) | 8 (3.4%) | 1.00 |
| Safety | |||||||||
| Stent thrombosis 1 | 3 (0.9%) | 6 (1.7%) | 0.51 | 5 (3.5%) | 1 (0.5%) | 0.04 | 2 (1.9%) | 1 (0.4%) | 0.23 |
| acute | 1 (0.3%) | 3 (0.8%) | 0.63 | 3 (2.1%) | 0 (0%) | 0.06 | 1 (1%) | 0 (0%) | 0.31 |
| subacute | 1 (0.3%) | 2 (0.6%) | 1.0 | 1 (0.7%) | 1 (0.5%) | 1.00 | 0 (0%) | 1 (0.4%) | 1.00 |
| late | 1 (0.3%) | 1 (0.3%) | 1.0 | 1 (0.7%) | 0 (0%) | 0.39 | 1 (0.96%) | 0 (0%) | 0.31 |
| Very late | 0 (0%) | 0 (0%) | - | 0 (0%) | 0 (0%) | - | 0 (0%) | 0 (0%) | - |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dola, J.; Morawiec, B.; Wańha, W.; Nowalany-Kozielska, E.; Wojakowski, W.; Kawecki, D. Results of PCI with Drug-Eluting Stents in an All-Comer Population Depending on Vessel Diameter. J. Clin. Med. 2020, 9, 524. https://doi.org/10.3390/jcm9020524
Dola J, Morawiec B, Wańha W, Nowalany-Kozielska E, Wojakowski W, Kawecki D. Results of PCI with Drug-Eluting Stents in an All-Comer Population Depending on Vessel Diameter. Journal of Clinical Medicine. 2020; 9(2):524. https://doi.org/10.3390/jcm9020524
Chicago/Turabian StyleDola, Janusz, Beata Morawiec, Wojciech Wańha, Ewa Nowalany-Kozielska, Wojciech Wojakowski, and Damian Kawecki. 2020. "Results of PCI with Drug-Eluting Stents in an All-Comer Population Depending on Vessel Diameter" Journal of Clinical Medicine 9, no. 2: 524. https://doi.org/10.3390/jcm9020524