Impact of Morphine Treatment on Infarct Size and Reperfusion Injury in Acute Reperfused ST-Elevation Myocardial Infarction

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
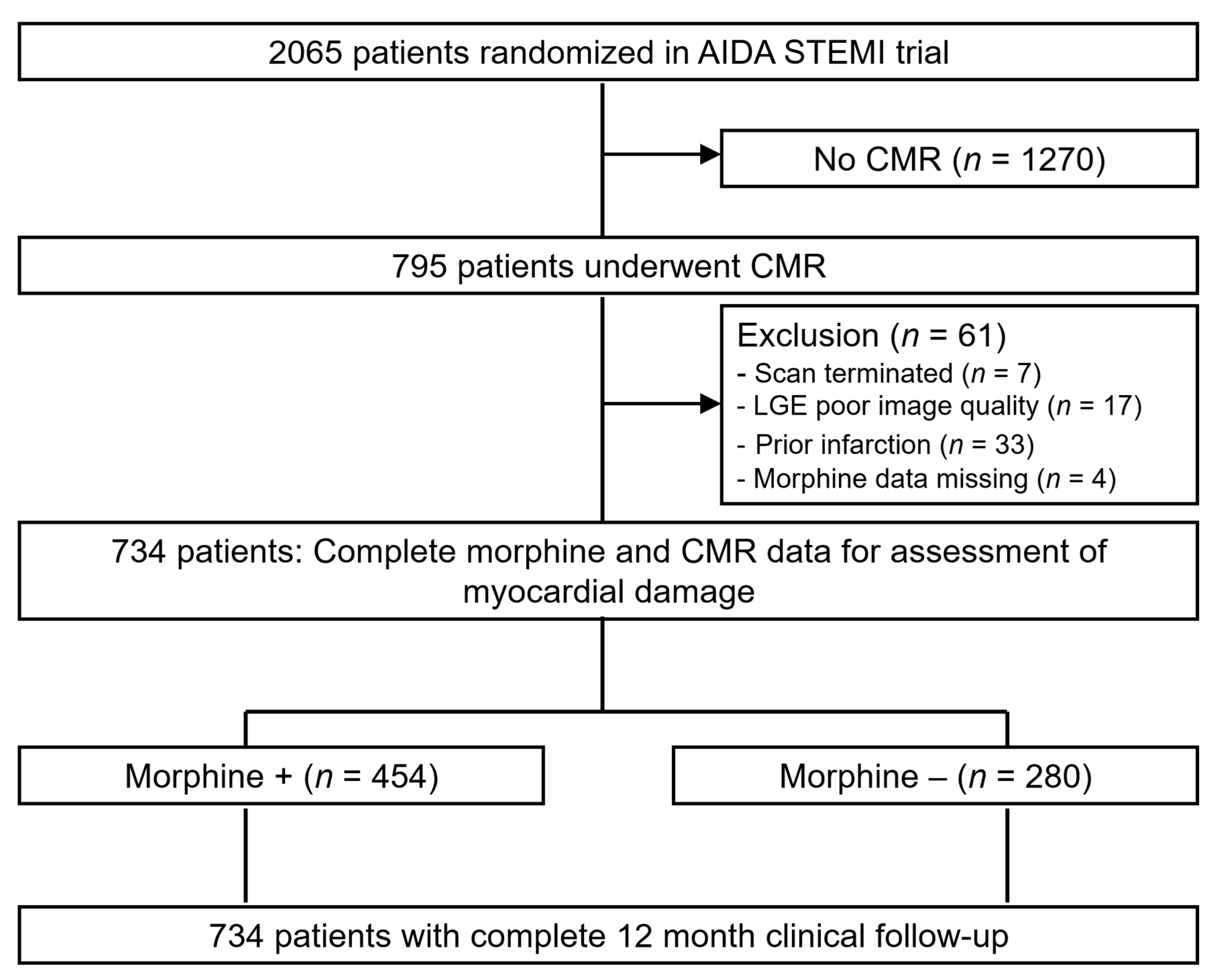
2.1. Study Design
2.2. Cardiac Magnetic Resonance Imaging
2.3. Clinical Outcome
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
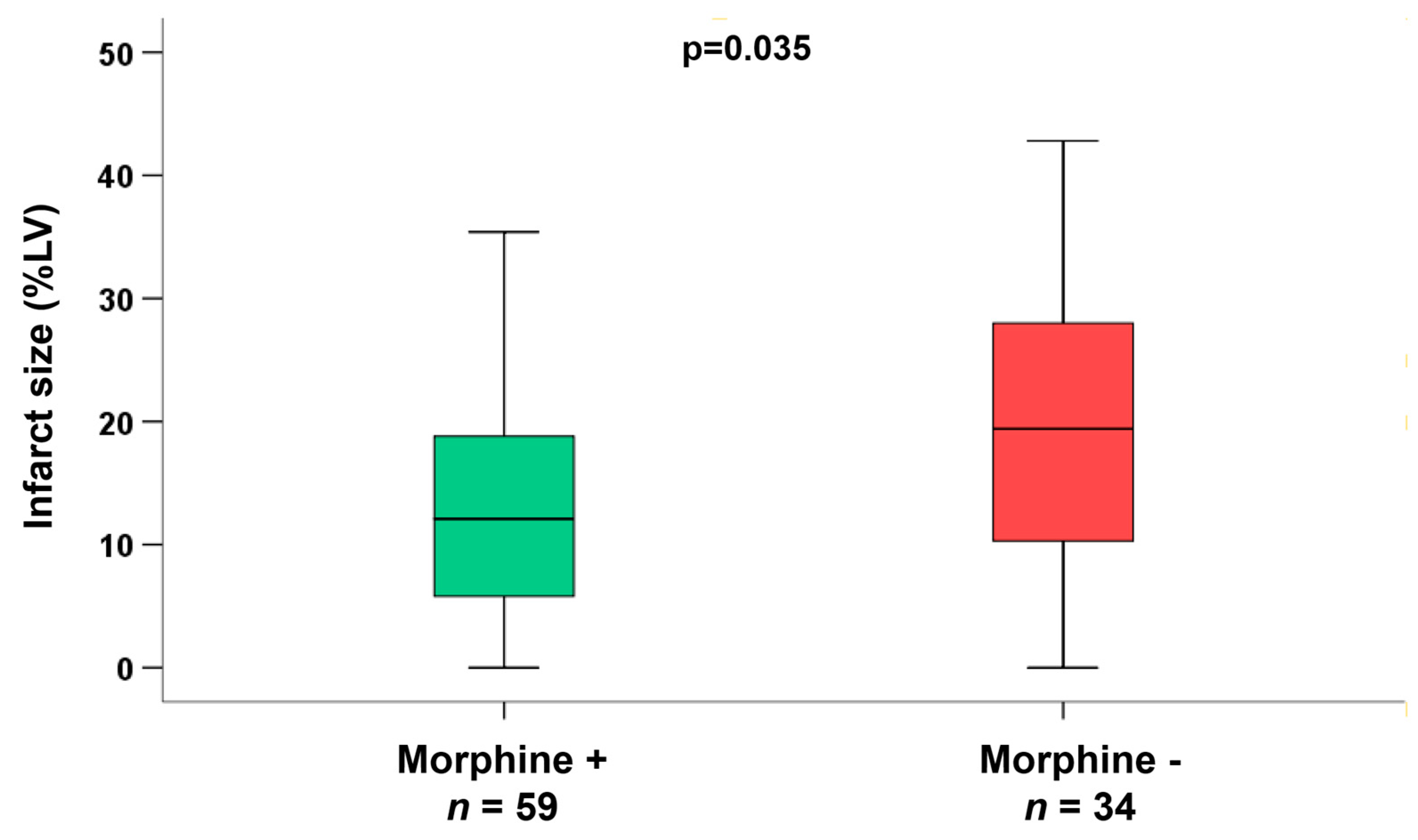
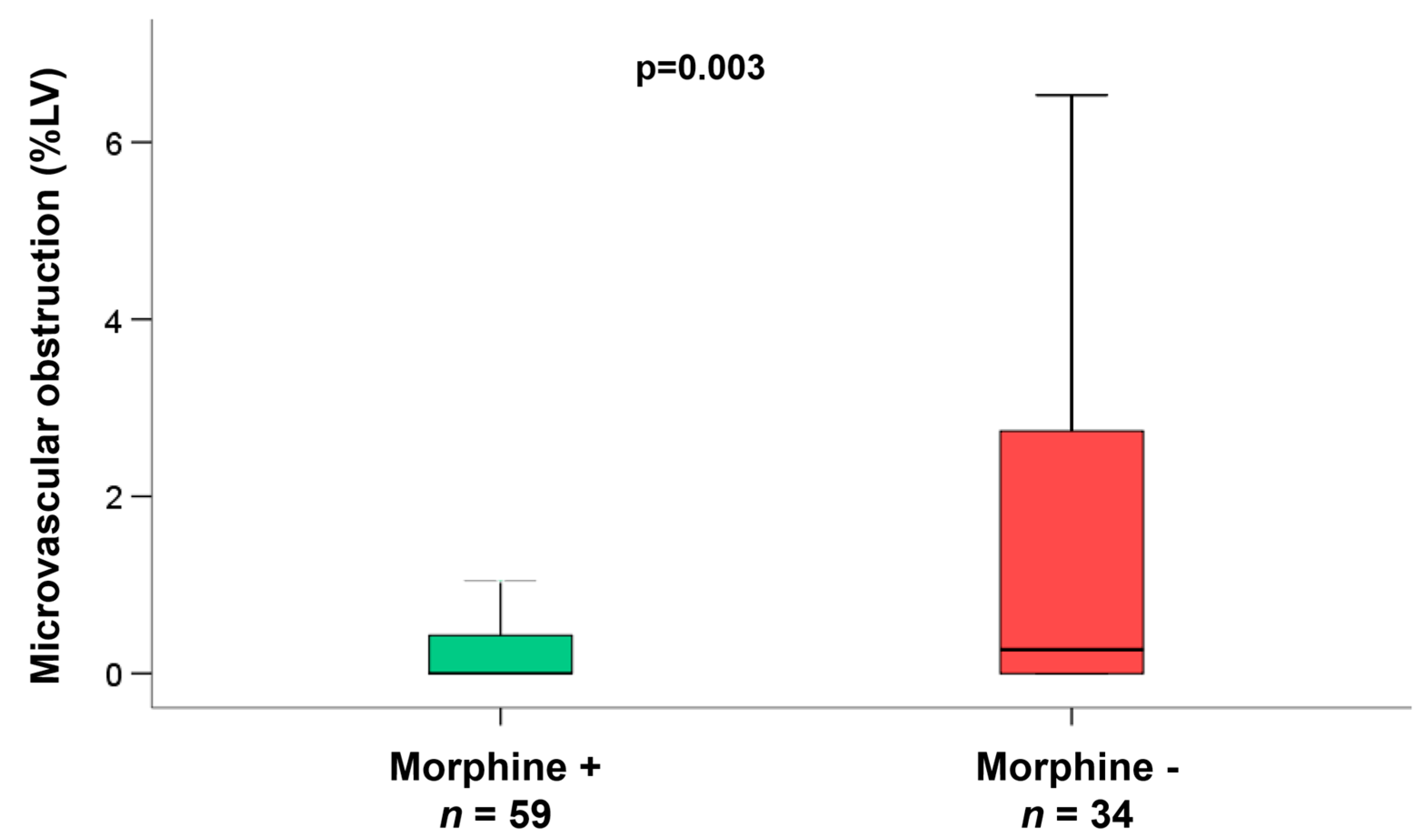
3.2. CMR Parameters
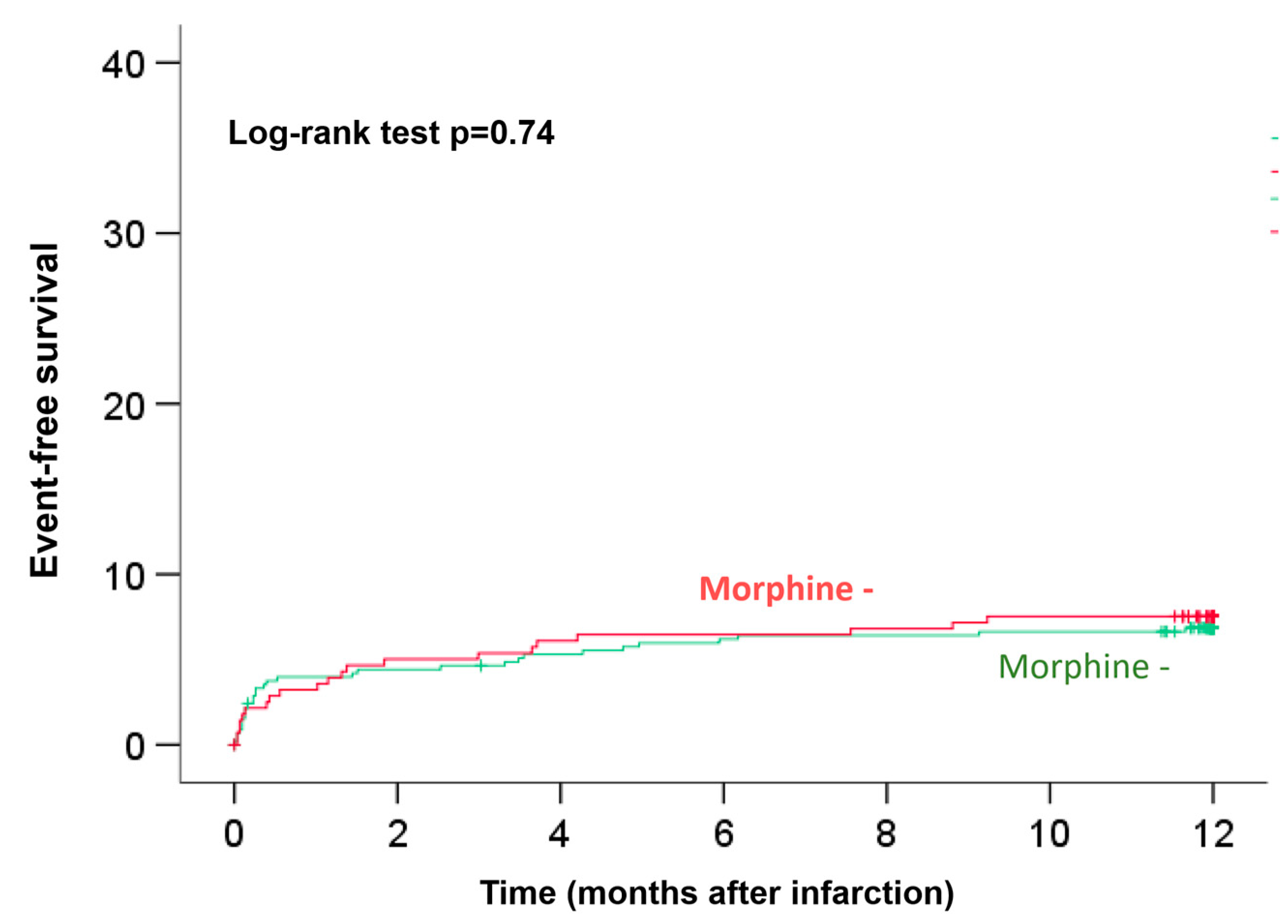
3.3. Clinical Outcome
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar]
- Roffi, M.; Patrono, C.; Collet, J.P.; Mueller, C.; Valgimigli, M.; Andreotti, F.; Bax, J.J.; Borger, M.A.; Brotons, C.; Chew, D.P.; et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2016, 37, 267–315. [Google Scholar] [PubMed]
- Wiviott, S.D.; Braunwald, E.; McCabe, C.H.; Montalescot, G.; Ruzyllo, W.; Gottlieb, S.; Neumann, F.-J.; Ardissino, D.; De Servi, S.; Murphy, S.A.; et al. Prasugrel versus clopidogrel in patients with acute coronary syndromes. N. Engl. J. Med. 2007, 357, 2001–2015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valgimigli, M.; Bueno, H.; Byrne, R.A.; Collet, J.-P.; Costa, F.; Jeppsson, A.; Jüni, P.; Kastrati, A.; Kolh, P.; Mauri, L.; et al. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS: The Task Force for dual antiplatelet therapy in coronary artery disease of the European Society of Cardiology (ESC) and of the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2018, 39, 213–260. [Google Scholar] [PubMed]
- Wallentin, L.; Becker, R.C.; Budaj, A.; Cannon, C.P.; Emanuelsson, H.; Held, C.; Horrow, J.; Husted, S.; James, S.; Katus, H.; et al. Ticagrelor versus clopidogrel in patients with acute coronary syndromes. N. Engl. J. Med. 2009, 361, 1045–1057. [Google Scholar] [CrossRef]
- Nimmo, W.S.; Heading, R.C.; Wilson, J.; Tothill, P.; Prescott, L.F. Inhibition of gastric emptying and drug absorption by narcotic analgesics. Br. J. Clin. Pharmacol. 1975, 2, 509–513. [Google Scholar] [CrossRef] [Green Version]
- Kubica, J.; Adamski, P.; Ostrowska, M.; Sikora, J.; Kubica, J.M.; Sroka, W.D.; Stankowska, K.; Buszko, K.; Navarese, E.P.; Jilma, B.; et al. Morphine delays and attenuates ticagrelor exposure and action in patients with myocardial infarction: The randomized, double-blind, placebo-controlled IMPRESSION trial. Eur. Heart J. 2016, 37, 245–252. [Google Scholar] [CrossRef]
- Silvain, J.; Storey, R.F.; Cayla, G.; Esteve, J.-B.; Dillinger, J.-G.; Rousseau, H.; Tsatsaris, A.; Baradat, C.; Salhi, N.; Hamm, C.W.; et al. P2Y12 receptor inhibition and effect of morphine in patients undergoing primary PCI for ST-segment elevation myocardial infarction. The PRIVATE-ATLANTIC study. Thromb. Haemost. 2016, 116, 369–378. [Google Scholar]
- Parodi, G.; Bellandi, B.; Xanthopoulou, I.; Capranzano, P.; Capodanno, D.; Valenti, R.; Stavrou, K.; Migliorini, A.; Antoniucci, D.; Tamburino, C.; et al. Morphine is associated with a delayed activity of oral antiplatelet agents in patients with ST-elevation acute myocardial infarction undergoing primary percutaneous coronary intervention. Circ. Cardiovasc. Interv. 2015, 8. [Google Scholar] [CrossRef] [Green Version]
- Meine, T.J.; Roe, M.T.; Chen, A.Y.; Patel, M.R.; Washam, J.B.; Ohman, E.M.; Peacock, W.F.; Pollack, C.V., Jr.; Gibler, W.B.; Peterson, E.D. Association of intravenous morphine use and outcomes in acute coronary syndromes: Results from the CRUSADE Quality Improvement Initiative. Am. Heart J. 2005, 149, 1043–1049. [Google Scholar] [CrossRef]
- de Waha, S.; Eitel, I.; Desch, S.; Fuernau, G.; Lurz, P.; Urban, D.; Schuler, G.; Thiele, H. Intravenous morphine administration and reperfusion success in ST-elevation myocardial infarction: Insights from cardiac magnetic resonance imaging. Clin. Res. Cardiol. 2015, 104, 727–734. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.L.; Chang, H.; Hung, C.R.; Tseng, Y.Z. Morphine preconditioning attenuates neutrophil activation in rat models of myocardial infarction. Cardiovasc. Res. 1998, 40, 557–563. [Google Scholar] [CrossRef] [Green Version]
- Murphy, G.S.; Szokol, J.W.; Marymont, J.H.; Avram, M.J.; Vender, J.S. Opioids and cardioprotection: The impact of morphine and fentanyl on recovery of ventricular function after cardiopulmonary bypass. J. Cardiothorac. Vasc. Anesth. 2006, 20, 493–502. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, K.; Kersten, J.R.; Riess, M.L. Opioid-induced cardioprotection. Curr. Pharm. Des. 2014, 20, 5696–5705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, C.; Dai, R.; Yu, R.; Xu, J. Morphine preconditioning, cardioprotection and left ventricular remodelling in rabbits. Acta Cardiol. 2011, 66, 341–348. [Google Scholar] [CrossRef]
- Bellandi, B.; Zocchi, C.; Xanthopoulou, I.; Scudiero, F.; Valenti, R.; Migliorini, X.; Antoniucci, D.; Marchionni, N.; Alexopoulos, D.; Parodi, G. Morphine use and myocardial reperfusion in patients with acute myocardial infarction treated with primary PCI. Int. J. Cardiol. 2016, 221, 567–571. [Google Scholar] [CrossRef]
- Bonin, M.; Mewton, N.; Roubille, F.; Morel, O.; Cayla, G.; Angoulvant, D.; Elbaz, M.; Claeys, M.J.; Garcia-Dorado, D.; Giraud, C.; et al. Effect and safety of morphine use in acute anterior st-segment elevation myocardial infarction. J. Am. Heart Assoc. 2018, 7. [Google Scholar] [CrossRef] [Green Version]
- Rentoukas, I.; Giannopoulos, G.; Kaoukis, A.; Kossyvakis, C.; Raisakis, K.; Driva, M.; Panagopoulou, V.; Tsarouchas, K.; Vavetsi, S.; Pyrgakis, V.; et al. Cardioprotective role of remote ischemic periconditioning in primary percutaneous coronary intervention: Enhancement by opioid action. JACC Cardiovasc. Interv. 2010, 3, 49–55. [Google Scholar] [CrossRef] [Green Version]
- Eitel, I.; de Waha, S.; Wohrle, J.; Fuernau, G.; Lurz, P.; Pauschinger, M.; Desch, S.; Schuler, G.; Thiele, H. Comprehensive prognosis assessment by CMR imaging after ST-segment elevation myocardial infarction. J. Am. Coll. Cardiol. 2014, 64, 1217–1226. [Google Scholar] [CrossRef]
- Thiele, H.; Wöhrle, J.; Hambrecht, R.; Rittger, H.; Birkemeyer, R.; Lauer, B.; Neuhaus, P.; Brosteanu, O.; Sick, P.; Wiemer, M.; et al. Intracoronary versus intravenous bolus abciximab during primary percutaneous coronary intervention in patients with acute ST-elevation myocardial infarction: A randomised trial. Lancet 2012, 379, 923–931. [Google Scholar] [CrossRef]
- Eitel, I.; Wohrle, J.; Suenkel, H.; Meissner, J.; Kerber, S.; Lauer, B.; Pauschinger, M.; Birkemeyer, R.; Axthelm, C.; Zimmermann, R.; et al. Intracoronary compared with intravenous bolus abciximab application during primary percutaneous coronary intervention in ST-segment elevation myocardial infarction: Cardiac magnetic resonance sub-study of the AIDA STEMI trial. J. Am. Coll. Cardiol. 2013, 61, 1447–1454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Desch, S.; Engelhardt, H.; Meissner, J.; Eitel, I.; Sareban, M.; Fuernau, G.; de Waha, S.; Grothoff, M.; Gutberlet, M.; Schuler, G.; et al. Reliability of myocardial salvage assessment by cardiac magnetic resonance imaging in acute reperfused myocardial infarction. Int. J. Cardiovasc. Imaging 2012, 28, 263–272. [Google Scholar] [CrossRef]
- Thiele, H.; Wohrle, J.; Neuhaus, P.; Brosteanu, O.; Sick, P.; Prondzinsky, R.; Birkemeyer, R.; Wiemer, M.; Kerber, S.; Schuehlen, H.; et al. Intracoronary compared with intravenous bolus abciximab application during primary percutaneous coronary intervention: Design and rationale of the Abciximab Intracoronary versus intravenously Drug Application in ST-Elevation Myocardial Infarction (AIDA STEMI) trial. Am. Heart J. 2010, 159, 547–554. [Google Scholar] [PubMed]
- Eitel, I.; Kubusch, K.; Strohm, O.; Desch, S.; Mikami, Y.; de Waha, S.; Gutberlet, M.; Schuler, G.; Friedrich, M.G.; Thiele, H. Prognostic value and determinants of a hypointense infarct core in T2-weighted cardiac magnetic resonance in acute reperfused ST-elevation-myocardial infarction. Circ. Cardiovasc. Imaging 2011, 4, 354–362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eitel, I.; Desch, S.; de Waha, S.; Fuernau, G.; Gutberlet, M.; Schuler, G.; Thiele, H. Long-term prognostic value of myocardial salvage assessed by cardiovascular magnetic resonance in acute reperfused myocardial infarction. Heart 2011, 97, 2038–2045. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, C.P.; Mullins, K.V.; Sidhu, S.S.; Schulman, S.P.; McEvoy, J.W. The on- and off-target effects of morphine in acute coronary syndrome: A narrative review. Am. Heart J. 2016, 176, 114–121. [Google Scholar] [CrossRef]
- Puymirat, E.; Lamhaut, L.; Bonnet, N.; Aissaoui, N.; Henry, P.; Cayla, G.; Cattan, S.; Steg, G.; Mock, L.; Ducrocq, G.; et al. Correlates of pre-hospital morphine use in ST-elevation myocardial infarction patients and its association with in-hospital outcomes and long-term mortality: The FAST-MI (French Registry of Acute ST-elevation and non-ST-elevation Myocardial Infarction) programme. Eur. Heart J. 2016, 37, 1063–1071. [Google Scholar]
- Chen, Z.; Spahn, D.R.; Zhang, X.; Liu, Y.; Chu, H.; Liu, Z. Morphine postconditioning protects against Reperfusion Injury: The role of protein kinase C-Epsilon, extracellular signal-regulated kinase 1/2 and mitochondrial permeability transition pores. Cell. Physiol. Biochem. 2016, 39, 1930–1940. [Google Scholar] [CrossRef] [Green Version]
- Ling, J.; Wong, G.T.; Yao, L.; Xia, Z.; Irwin, M.G. Remote pharmacological post-conditioning by intrathecal morphine: Cardiac protection from spinal opioid receptor activation. Acta Anaesthesiol. Scand. 2010, 54, 1097–1104. [Google Scholar] [CrossRef] [Green Version]
- Schultz, J.E.; Rose, E.; Yao, Z.; Gross, G.J. Evidence for involvement of opioid receptors in ischemic preconditioning in rat hearts. Am. J. Physiol. 1995, 268, H2157–H2161. [Google Scholar] [CrossRef]
- Liu, Q.; Li, Z.; Liu, Y.; Chen, Q.; Deng, R.; Gao, Z.; Yu, D.; Zhang, Y. Hydromorphine postconditioning protects isolated rat heart against ischemia-reperfusion injury via activating P13K/Akt/eNOS signaling. Cardiovasc. Ther. 2018, 36, e12481. [Google Scholar] [CrossRef] [PubMed]
- Gross, G.J.; Hsu, A.; Nithipatikom, K.; Bobrova, I.; Bissessar, E. Eribis peptide 94 reduces infarct size in rat hearts via activation of centrally located mu opioid receptors. J. Cardiovasc. Pharmacol. 2012, 59, 194–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schultz, J.E.; Gross, G.J. Opioids and cardioprotection. Pharmacol. Ther. 2001, 89, 123–137. [Google Scholar] [CrossRef]
- Zhang, Y.; Irwin, M.G.; Wong, T.M. Remifentanil preconditioning protects against ischemic injury in the intact rat heart. Anesthesiology 2004, 101, 918–923. [Google Scholar] [CrossRef] [PubMed]
- Peart, J.N.; Gross, E.R.; Reichelt, M.E.; Hsu, A.; Headrick, J.P.; Gross, G.J. Activation of kappa-opioid receptors at reperfusion affords cardioprotection in both rat and mouse hearts. Basic Res. Cardiol. 2008, 103, 454–463. [Google Scholar] [CrossRef] [PubMed]
- Peart, J.N.; Gross, E.R.; Gross, G.J. Effect of exogenous kappa-opioid receptor activation in rat model of myocardial infarction. J. Cardiovasc. Pharmacol. 2004, 43, 410–415. [Google Scholar] [CrossRef]
- Peart, J.N.; Gross, G.J. Exogenous activation of delta- and kappa-opioid receptors affords cardioprotection in isolated murine heart. Basic Res. Cardiol. 2004, 99, 29–37. [Google Scholar] [CrossRef]
- Pugsley, M.K.; Penz, W.P.; Walker, M.J.; Wong, T.M. Antiarrhythmic effects of U-50,488H in rats subject to coronary artery occlusion. Eur. J. Pharmacol. 1992, 212, 15–19. [Google Scholar] [CrossRef]
- Wang, G.Y.; Wu, S.; Pei, J.M.; Yu, X.C.; Wong, T.M. Kappa- but not delta-opioid receptors mediate effects of ischemic preconditioning on both infarct and arrhythmia in rats. Am. J. Physiol. Heart Circ. Physiol. 2001, 280, H384–H391. [Google Scholar] [CrossRef]
- Bell, S.P.; Sack, M.N.; Patel, A.; Opie, L.H.; Yellon, D.M. Delta opioid receptor stimulation mimics ischemic preconditioning in human heart muscle. J. Am. Coll. Cardiol. 2000, 36, 2296–2302. [Google Scholar] [CrossRef] [Green Version]
- Okubo, S.; Tanabe, Y.; Takeda, K.; Kitayama, M.; Kanemitsu, S.; Kukreja, R.C.; Takekoshi, N. Ischemic preconditioning and morphine attenuate myocardial apoptosis and infarction after ischemia-reperfusion in rabbits: Role of delta-opioid receptor. Am. J. Physiol. Heart Circ. Physiol. 2004, 287, H1786–H1791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peart, J.N.; Patel, H.H.; Gross, G.J. Delta-opioid receptor activation mimics ischemic preconditioning in the canine heart. J. Cardiovasc. Pharmacol. 2003, 42, 78–81. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.L.; Chang, H.; Hung, C.R.; Tseng, Y.Z. Attenuation of neutrophil and endothelial activation by intravenous morphine in patients with acute myocardial infarction. Am. J. Cardiol. 1997, 80, 1532–1535. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Total Study | Morphine + | Morphine − | p-Value | |
|---|---|---|---|---|---|
| n = 734 | n = 454 | n = 280 | |||
| Age (years) | 62 (51–71) | 61 (51–70) | 66 (52–72) | 0.03 | |
| Male sex: n (%) | 555/734 (76%) | 356/454 (78%) | 199/280 (71%) | 0.02 | |
| Cardiovascular risk factors: n (%) | |||||
| Current smoking | 316/670 (47%) | 207/415 (50%) | 109/255 (43%) | 0.07 | |
| Hypertension | 488/731 (67%) | 287/452 (64%) | 201/279 (72%) | 0.02 | |
| Hypercholesterolemia | 258/727 (36%) | 156/450 (34%) | 102/277 (37%) | 0.55 | |
| Diabetes mellitus | 146/731 (20%) | 76/453 (17%) | 70/278 (25%) | 0.01 | |
| BMI (kg/m2) | 27.3 (24.8–30.1) | 27.5 (25.0–30.2) | 27.0 (24.6–30.1) | 0.31 | |
| Anterior infarction: n (%) | 343/702 (51%) | 215/439 (49%) | 128/263 (49%) | 0.94 | |
| Heart-rate (min) | 76 (67–87) | 76 (66–86) | 77 (70–88) | 0.19 | |
| Systolic blood pressure (mmHg) | 130 (117–147) | 130 (116–145) | 134 (119–150) | 0.42 | |
| Diastolic blood pressure (mmHg) | 80 (70–88) | 80 (70–86) | 80 (70–90) | 0.82 | |
| Times (min) | |||||
| Symptom onset to PCI hospital admission | 180 (109–315) | 165 (100–276) | 200 (123–404) | <0.001 | |
| Door-to-balloon-time | 30 (22–42) | 30 (21–40) | 30 (23–45) | 0.67 | |
| Killip-class on admission: n (%) | 0.59 | ||||
| 1 | 650/734 (89%) | 405/454 (89%) | 245/280 (88%) | ||
| 2 | 50/734 (7%) | 28/454 (6%) | 22/280 (8%) | ||
| 3 | 17/734 (2%) | 9/454 (2%) | 8/280 (3%) | ||
| 4 | 17/734 (2%) | 12/454 (3%) | 5/280 (2%) | ||
| Number of diseased vessels: n (%) | 0.76 | ||||
| 1 | 398/734 (54%) | 251/454 (55%) | 147/ 280 (53%) | ||
| 2 | 206/734 (28%) | 125/454 (28%) | 81/280 (29%) | ||
| 3 | 130/734 (18%) | 78/454 (17%) | 52/280 (19%) | ||
| Infarct related artery: n (%) | 0.69 | ||||
| Left anterior descending | 328/734 (45%) | 199/454 (44%) | 129/280 (46%) | ||
| Left circumflex | 89/734 (12%) | 56/454 (12%) | 33/280 (12%) | ||
| Right coronary | 314/734 (43%) | 198/454 (44%) | 116/280 (41%) | ||
| Left main | 3/734 (0%) | 1/454 (0%) | 2/280 (1%) | ||
| TIMI-flow before PCI: n (%) | 0.47 | ||||
| TIMI-flow 0 | 412/734 (56%) | 246/454 (54%) | 166/280 (59%) | ||
| TIMI-flow I | 97/734 (13%) | 66/454 (15%) | 31/280 (11%) | ||
| TIMI-flow II | 119/734 (16%) | 75/454 (16%) | 44/280 (16%) | ||
| TIMI-flow III | 106/734 (14%) | 67/454 (15%) | 39/280 (14%) | ||
| Thrombectomy: n (%) | 111/454 (24%) | 111/454 (24%) | 68/280 (24%) | 0.96 | |
| TIMI-flow post PCI: n (%) | 0.17 | ||||
| TIMI-flow 0 | 11/734 (1%) | 7/454 (1%) | 4/280 (1%) | ||
| TIMI-flow I | 19/734 (3%) | 13/ 454 (3%) | 6/280 (2%) | ||
| TIMI-flow II | 56/734 (8%) | 27/454 (6%) | 29/280 (10%) | ||
| TIMI-flow III | 648/734 (88%) | 407/454 (90%) | 93/280 (86%) | ||
| Peak CK (µmol/l*s) | 26 (12–46) | 27 (13–48) | 26 (10–43) | 0.28 | |
| ST-segment resolution (%) | 55 (23–78) | 58 (25–79) | 51 (20–77) | 0.12 | |
| Concomitant medications: n (%) | |||||
| ß-blockers | 703/732 (96%) | 433/453 (96%) | 270/279 (97%) | 0.43 | |
| ACE-inhibitors/AT-1-antagonist | 698/732 (95%) | 433/453 (96%) | 265/279 (95%) | 0.71 | |
| Aspirin | 734/734 (100%) | 454 /454 (100%) | 280 /280 (100%) | 1 | |
| Clopidogrel, prasugrel or both | 734/734 (100%) | 454 /454 (100%) | 280 /280 (100%) | 1 | |
| Statins | 699/732 (96%) | 435/453 (96%) | 264/279 (95%) | 0.37 | |
| Aldosterone antagonist | 88/732 (12%) | 51/453 (11%) | 37/279 (14%) | 0.42 | |
| Completion of abciximab infusion | 688/733 (94%) | 429/453 (95%) | 259/280 (93%) | 0.94 | |
| Characteristic | Total Study n = 734 | Morphine + n = 454 | Morphine − n = 280 | p |
|---|---|---|---|---|
| Area at risk (edema) (%LV) | 35 (25–48) | 36 (25–48) | 35 (27–48) | 0.72 |
| Infarct size (%LV) | 17 (8–25) | 16 (8–26) | 17 (9–24) | 0.67 |
| Myocardial salvage (%LV) | 17 (9–27) | 17 (9–26) | 17 (8–27) | 0.45 |
| Myocardial salvage index | 51 (33–69) | 51 (32–69) | 52 (35–69) | 0.65 |
| Late MO (%LV) | 0.0 (0.0–1.8) | 0.0 (0.0–1.8) | 0.0 (0.0 – 1.9) | 0.92 |
| LV ejection fraction (%) | 51 (44–58) | 51 (44–58) | 50 (43–58) | 0.71 |
| LV end-diastolic volume (mL) | 146 (121–171) | 145 (124–174) | 141 (112–166) | 0.004 |
| LV end-systolic volume (mL) | 72 (54–91) | 72 (55–93) | 71 (52–88) | 0.18 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eitel, I.; Wang, J.; Stiermaier, T.; Fuernau, G.; Feistritzer, H.-J.; Joost, A.; Jobs, A.; Meusel, M.; Blodau, C.; Desch, S.; et al. Impact of Morphine Treatment on Infarct Size and Reperfusion Injury in Acute Reperfused ST-Elevation Myocardial Infarction. J. Clin. Med. 2020, 9, 735. https://doi.org/10.3390/jcm9030735
Eitel I, Wang J, Stiermaier T, Fuernau G, Feistritzer H-J, Joost A, Jobs A, Meusel M, Blodau C, Desch S, et al. Impact of Morphine Treatment on Infarct Size and Reperfusion Injury in Acute Reperfused ST-Elevation Myocardial Infarction. Journal of Clinical Medicine. 2020; 9(3):735. https://doi.org/10.3390/jcm9030735
Chicago/Turabian StyleEitel, Ingo, Juan Wang, Thomas Stiermaier, Georg Fuernau, Hans-Josef Feistritzer, Alexander Joost, Alexander Jobs, Moritz Meusel, Christian Blodau, Steffen Desch, and et al. 2020. "Impact of Morphine Treatment on Infarct Size and Reperfusion Injury in Acute Reperfused ST-Elevation Myocardial Infarction" Journal of Clinical Medicine 9, no. 3: 735. https://doi.org/10.3390/jcm9030735