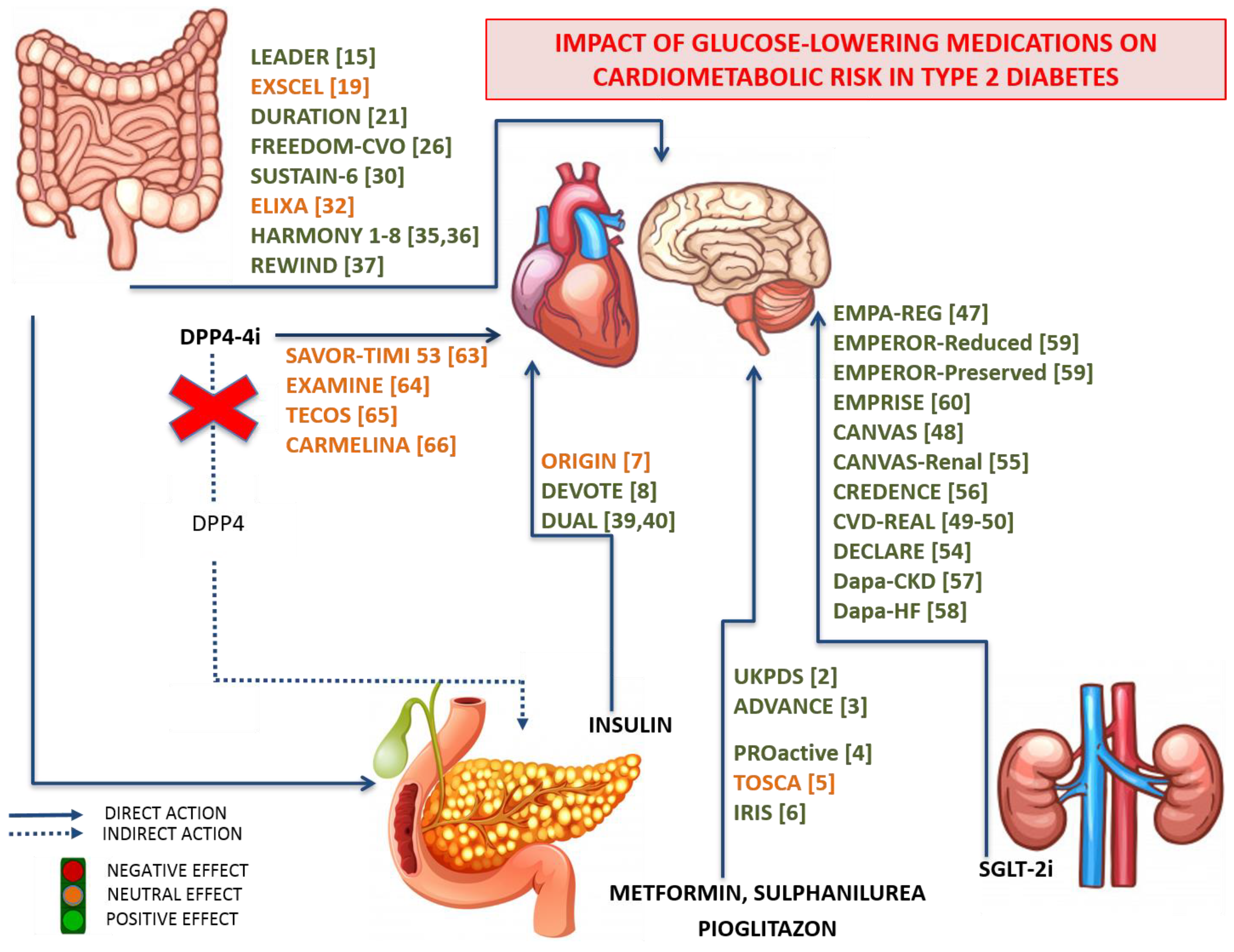
Impact of Glucose-Lowering Medications on Cardiovascular and Metabolic Risk in Type 2 Diabetes

 ,
, 
Abstract
:1. Introduction
2. Search Strategy
3. Traditional Anti-Diabetic Drugs
4. Novel Anti-Diabetic Drugs
4.1. Glucagon Like Peptide-1 Receptor Agonists (GLP-1RAs)
4.2. Sodium Glucose coTransporter-2 Inhibitors (SGLT2-is)
4.3. Dipeptidyl Peptidase-4 Inhibitors (DPP4-is)
5. Discussion and Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- García-Carro, C.; Vergara, A.; Agraz, I.; Jacobs-Cachá, C.; Espinel, E.; Seron, D.; Soler, M.J. The New Era for Reno-Cardiovascular Treatment in Type 2 Diabetes. J. Clin. Med. 2019, 8, 864. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- UK Prospective Diabetes Study (UKPDS) Group. Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). Lancet 1998, 352, 854–865. [Google Scholar] [CrossRef]
- Patel, A.; MacMahon, S.; Chalmers, J.; Neal, B.; Billot, L.; Woodward, M.; Marre, M.; Cooper, M.; Glasziou, P.; Grobbee, D.; et al. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N. Engl. J. Med. 2008, 358, 2560–2572. [Google Scholar] [PubMed] [Green Version]
- Dormandy, J.A.; Charbonnel, B.; Eckland, D.J.; Erdmann, E.; Massi-Benedetti, M.; Moules, I.K.; Skene, A.M.; Tan, M.H.; Lefebvre, P.J.; Murray, G.D.; et al. Secondary prevention of macrovascular events in patients with type 2 diabetes in the PROactive Study (PROspective pioglitAzone Clinical Trial In macroVascular Events): A randomised controlled trial. Lancet 2005, 366, 1279–1289. [Google Scholar] [CrossRef]
- Vaccaro, O.; Masulli, M.; Nicolucci, A.; Bonora, E.; Del Prato, S.; Maggioni, A.P.; Rivellese, A.A.; Squatrito, S.; Giorda, C.B.; Sesti, G.; et al. Effects on the incidence of cardiovascular events of the addition of pioglitazone versus sulfonylureas in patients with type 2 diabetes inadequately controlled with metformin (TOSCA.IT): A randomised, multicentre trial. Lancet Diabetes Endocrinol. 2017, 5, 887–897. [Google Scholar] [CrossRef] [Green Version]
- Young, L.H.; Viscoli, C.M.; Curtis, J.P.; Inzucchi, S.E.; Schwartz, G.G.; Lovejoy, A.M.; Furie, K.L.; Gorman, M.J.; Conwit, R.; Abbott, J.D.; et al. Cardiac Outcomes After Ischemic Stroke or Transient Ischemic Attack: Effects of Pioglitazone in Patients With Insulin Resistance Without Diabetes Mellitus. Circulation 2017, 135, 1882–1893. [Google Scholar] [CrossRef]
- Gerstein, H.C.; Bosch, J.; Dagenais, G.R.; Diaz, R.; Jung, H.; Maggioni, A.P.; Pogue, J.; Probstfield, J.; Ramachandran, A.; Riddle, M.C.; et al. Basal insulin and cardiovascular and other outcomes in dysglycemia. N. Engl. J. Med. 2012, 367, 319–328. [Google Scholar]
- Marso, S.P.; McGuire, D.K.; Zinman, B.; Poulter, N.R.; Emerson, S.S.; Pieber, T.R.; Pratley, R.E.; Haahr, P.M.; Lange, M.; Brown-Frandsen, K.; et al. Efficacy and Safety of Degludec versus Glargine in Type 2 Diabetes. N. Engl. J. Med. 2017, 377, 723–732. [Google Scholar] [CrossRef]
- Kim, W.; Egan, J.M. The role of incretins in glucose homeostasis and diabetes treatment. Pharmacol. Rev. 2008, 60, 470–512. [Google Scholar] [CrossRef] [Green Version]
- O’Brien, M.J.; Karam, S.L.; Wallia, A.; Kang, R.H.; Cooper, A.J.; Lancki, N.; Moran, M.R.; Liss, D.T.; Prospect, T.A.; Ackermann, R.T. Association of Second-line Antidiabetic Medications With Cardiovascular Events Among Insured Adults With Type 2 Diabetes. JAMA Netw. Open. 2018, 1, e186125. [Google Scholar] [CrossRef]
- Kant, R.; Munir, K.M.; Kaur, A.; Verma, V. Prevention of macrovascular complications in patients with type 2 diabetes mellitus: Review of cardiovascular safety and efficacy of newer diabetes medications. World J. Diabetes 2019, 10, 324–332. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Zheng, J.; Wang, S.; Lau, H.K.; Fathi, A.; Wang, Q. Cardiovascular Benefits of Native GLP-1 and its Metabolites: An Indicator for GLP-1-Therapy Strategies. Front. Physiol. 2017, 8, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rizzo, M.; Nikolic, D.; Patti, A.M.; Mannina, C.; Montalto, G.; McAdams, B.S.; Rizvi, A.A.; Cosentino, F. GLP-1 receptor agonists and reduction of cardiometabolic risk: Potential underlying mechanisms. Biochim. Biophys. Acta Mol. Basis Dis. 2018, 1864, 2814–2821. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Khismatullin, D.B. Oxidized low-density lipoprotein contributes to atherogenesis via co-activation of macrophages and mast cells. PLoS ONE 2015, 10, e0123088. [Google Scholar] [CrossRef]
- Marso, S.P.; Daniels, G.H.; Brown-Frandsen, K.; Kristensen, P.; Mann, J.F.; Nauck, M.A.; Nissen, S.E.; Pocock, S.; Poulter, N.R.; Ravn, L.S.; et al. Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2016, 375, 311–322. [Google Scholar] [CrossRef] [Green Version]
- Rizzo, M.; Chandalia, M.; Patti, A.M.; Di Bartolo, V.; Rizvi, A.A.; Montalto, G.; Abate, N. Liraglutide decreases carotid intima-media thickness in patients with type 2 diabetes: 8-month prospective pilot study. Cardiovasc. Diabetol. 2014, 13, 49. [Google Scholar] [CrossRef] [Green Version]
- Rizvi, A.A.; Patti, A.M.; Giglio, R.V.; Nikolic, D.; Amato, A.; Al-Busaidi, N.; Al-Rasadi, K.; Soresi, M.; Banach, M.; Montalto, G.; et al. Liraglutide improves carotid intima-media thickness in patients with type 2 diabetes and non-alcoholic fatty liver disease: An 8-month prospective pilot study. Expert Opin. Biol. Ther. 2015, 15, 1391–1397. [Google Scholar] [CrossRef]
- Rizzo, M.; Rizvi, A.A.; Patti, A.M.; Nikolic, D.; Giglio, R.V.; Castellino, G.; Li Volti, G.; Caprio, M.; Montalto, G.; Provenzano, V.; et al. Liraglutide improves metabolic parameters and carotid intima-media thickness in diabetic patients with the metabolic syndrome: An 18-month prospective study. Cardiovasc. Diabetol. 2016, 15, 162. [Google Scholar] [CrossRef] [Green Version]
- Holman, R.R.; Bethel, M.A.; Mentz, R.J.; Thompson, V.P.; Lokhnygina, Y.; Buse, J.B.; Chan, J.C.; Choi, J.; Gustavson, S.M.; Iqbal, N.; et al. Effects of Once-Weekly Exenatide on Cardiovascular Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2017, 377, 1228–1239. [Google Scholar] [CrossRef]
- Torimoto, K.; Okada, Y.; Mori, H.; Otsuka, T.; Kawaguchi, M.; Matsuda, M.; Kuno, F.; Sugai, K.; Sonoda, S.; Hajime, M.; et al. Effects of exenatide on postprandial vascular endothelial dysfunction in type 2 diabetes mellitus. Cardiovasc. Diabetol. 2015, 14, 25. [Google Scholar] [CrossRef] [Green Version]
- Grimm, M.; Han, J.; Weaver, C.; Griffin, P.; Schulteis, C.T.; Dong, H.; Malloy, J. Efficacy, safety, and tolerability of exenatide once weekly in patients with type 2 diabetes mellitus: An integrated analysis of the DURATION trials. Postgrad. Med. 2013, 125, 47–57. [Google Scholar] [CrossRef] [PubMed]
- Diamant, M.; Van Gaal, L.; Guerci, B.; Stranks, S.; Han, J.; Malloy, J.; Boardman, M.K.; Trautmann, M.E. Exenatide once weekly versus insulin glargine for type 2 diabetes (DURATION-3): 3-year results of an open-label randomised trial. Lancet Diabetes Endocrinol. 2014, 2, 464–473. [Google Scholar] [CrossRef]
- Bhushan, R.; Elkind-Hirsch, K.E.; Bhushan, M.; Butler, W.J.; Duncan, K.; Marrioneaux, O. Improved glycemic control and reduction of cardiometabolic risk factors in subjects with type 2 diabetes and metabolic syndrome treated with exenatide in a clinical practice setting. Diabetes Technol. Ther. 2009, 11, 353–359. [Google Scholar] [CrossRef] [PubMed]
- Patti, A.M.; Nikolic, D.; Magan-Fernandez, A.; Giglio, R.V.; Castellino, G.; Chianetta, R.; Citarrella, R.; Corrado, E.; Provenzano, F.; Provenzano, V.; et al. Exenatide once-weekly improves metabolic parameters, endothelial dysfunction and carotid intima-media thickness in patients with type-2 diabetes: An 8-month prospective study. Diabetes Res. Clin. Pract. 2019, 149, 163–169. [Google Scholar] [CrossRef]
- Henry, R.R.; Rosenstock, J.; Logan, D.; Alessi, T.; Luskey, K.; Baron, M.A. Continuous subcutaneous delivery of exenatide via ITCA 650 leads to sustained glycemic control and weight loss for 48 weeks in metformin-treated subjects with type 2 diabetes. J. Diabetes Complicat. 2014, 28, 393–398. [Google Scholar] [CrossRef] [Green Version]
- Rosenstock, J.; Buse, J.B.; Azeem, R.; Prabhakar, P.; Kjems, L.; Huang, H.; Baron, M.A. Efficacy and Safety of ITCA 650, a Novel Drug-Device GLP-1 Receptor Agonist, in Type 2 Diabetes Uncontrolled With Oral Antidiabetes Drugs: The FREEDOM-1 Trial. Diabetes Care 2018, 41, 333–340. [Google Scholar] [CrossRef] [Green Version]
- Sun, F.; Wu, S.; Wang, J.; Guo, S.; Chai, S.; Yang, Z.; Li, L.; Zhang, Y.; Ji, L.; Zhan, S. Effect of glucagon-like peptide-1 receptor agonists on lipid profiles among type 2 diabetes: A systematic review and network meta-analysis. Clin. Ther. 2015, 37, 225–241.e228. [Google Scholar] [CrossRef]
- Soran, H.; Dent, R.; Durrington, P. Evidence-based goals in LDL-C reduction. Clin. Res. Cardiol. 2017, 106, 237–248. [Google Scholar] [CrossRef] [Green Version]
- El Abd Aziz, M.S.; Kahle, M.; Meier, J.J.; Nauck, M.A. A meta-analysis comparing clinical effects of short- or long-acting GLP-1 receptor agonists versus insulin treatment from head-to-head studies in type 2 diabetic patients. Diabetes Obes. Metab. 2017, 19, 216–227. [Google Scholar] [CrossRef]
- Marso, S.P.; Bain, S.C.; Consoli, A.; Eliaschewitz, F.G.; Jodar, E.; Leiter, L.A.; Lingvay, I.; Rosenstock, J.; Seufert, J.; Warren, M.L.; et al. Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N. Engl. J. Med. 2016, 375, 1834–1844. [Google Scholar] [CrossRef] [Green Version]
- Peterson, S.C.; Barry, A.R. Effect of Glucagon-like Peptide-1 Receptor Agonists on All-cause Mortality and Cardiovascular Outcomes: A Meta-analysis. Curr. Diabetes Rev. 2018, 14, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Pfeffer, M.A.; Claggett, B.; Diaz, R.; Dickstein, K.; Gerstein, H.C.; Kober, L.V.; Lawson, F.C.; Ping, L.; Wei, X.; Lewis, E.F.; et al. Lixisenatide in Patients with Type 2 Diabetes and Acute Coronary Syndrome. N. Engl. J. Med. 2015, 373, 2247–2257. [Google Scholar] [CrossRef] [PubMed]
- Bentley-Lewis, R.; Aguilar, D.; Riddle, M.C.; Claggett, B.; Diaz, R.; Dickstein, K.; Gerstein, H.C.; Johnston, P.; Kober, L.V.; Lawson, F.; et al. Rationale, design, and baseline characteristics in Evaluation of LIXisenatide in Acute Coronary Syndrome, a long-term cardiovascular end point trial of lixisenatide versus placebo. Am. Heart J. 2015, 169, 631–638.e637. [Google Scholar] [CrossRef] [PubMed]
- Bush, M.A.; Matthews, J.E.; De Boever, E.H.; Dobbins, R.L.; Hodge, R.J.; Walker, S.E.; Holland, M.C.; Gutierrez, M.; Stewart, M.W. Safety, tolerability, pharmacodynamics and pharmacokinetics of albiglutide, a long-acting glucagon-like peptide-1 mimetic, in healthy subjects. Diabetes Obes. Metab. 2009, 11, 498–505. [Google Scholar] [CrossRef]
- Lovshin, J.A. Glucagon-like Peptide-1 Receptor Agonists: A Class Update for Treating Type 2 Diabetes. Can. J. Diabetes 2017, 41, 524–535. [Google Scholar] [CrossRef]
- Rendell, M.S. Albiglutide: A unique GLP-1 receptor agonist. Expert Opin. Biol. Ther. 2016, 16, 1557–1569. [Google Scholar] [CrossRef]
- Gerstein, H.C.; Colhoun, H.M.; Dagenais, G.R.; Diaz, R.; Lakshmanan, M.; Pais, P.; Probstfield, J.; Riddle, M.C.; Rydén, L.; Xavier, D.; et al. Design and baseline characteristics of participants in the Researching cardiovascular Events with a Weekly INcretin in Diabetes (REWIND) trial on the cardiovascular effects of dulaglutide. Diabetes Obes. Metab. 2018, 20, 42–49. [Google Scholar] [CrossRef] [Green Version]
- Ferdinand, K.C.; Botros, F.T.; Atisso, C.M.; Sager, P.T. Cardiovascular safety for once-weekly dulaglutide in type 2 diabetes: A pre-specified meta-analysis of prospectively adjudicated cardiovascular events. Cardiovasc. Diabetol. 2016, 15, 38. [Google Scholar] [CrossRef] [Green Version]
- Meneghini, L.; Doshi, A.; Gouet, D.; Vilsbøll, T.; Begtrup, K.; Őrsy, P.; Ranthe, M.F.; Lingvay, I. Insulin degludec/liraglutide (IDegLira) maintains glycaemic control and improves clinical outcomes, regardless of pre-trial insulin dose, in people with type 2 diabetes that is uncontrolled on basal insulin. Diabet. Med. J. Br. Diabet. Assoc. 2019. [Google Scholar] [CrossRef]
- Davidson, J.A.; Desouza, C.; Fonseca, V.; Frias, J.P.; Van Gaal, L.; Giorgino, F.; Chao, J.; Dex, T.A.; Roberts, M.; Saremi, A.; et al. Glycaemic target attainment in people with Type 2 diabetes treated with insulin glargine/lixisenatide fixed-ratio combination: A post hoc analysis of the LixiLan-O and LixiLan-L trials. Diabet. Med. J. Br. Diabet. Assoc. 2019. [Google Scholar] [CrossRef] [Green Version]
- Inzucchi, S.E.; Zinman, B.; Wanner, C.; Ferrari, R.; Fitchett, D.; Hantel, S.; Espadero, R.M.; Woerle, H.J.; Broedl, U.C.; Johansen, O.E. SGLT-2 inhibitors and cardiovascular risk: Proposed pathways and review of ongoing outcome trials. Diabetes Vasc. Dis. Res. 2015, 12, 90–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ptaszynska, A.; Hardy, E.; Johnsson, E.; Parikh, S.; List, J. Effects of dapagliflozin on cardiovascular risk factors. Postgrad. Med. 2013, 125, 181–189. [Google Scholar] [CrossRef] [PubMed]
- Fadini, G.P.; Bonora, B.M.; Zatti, G.; Vitturi, N.; Iori, E.; Marescotti, M.C.; Albiero, M.; Avogaro, A. Effects of the SGLT2 inhibitor dapagliflozin on HDL cholesterol, particle size, and cholesterol efflux capacity in patients with type 2 diabetes: A randomized placebo-controlled trial. Cardiovasc. Diabetol. 2017, 16, 42. [Google Scholar] [CrossRef] [Green Version]
- Bays, H.E.; Sartipy, P.; Xu, J.; Sjostrom, C.D.; Underberg, J.A. Dapagliflozin in patients with type II diabetes mellitus, with and without elevated triglyceride and reduced high-density lipoprotein cholesterol levels. J. Clin. Lipidol. 2017, 11, 450–458.e451. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, T.; Fukui, T.; Nakanishi, N.; Yamamoto, S.; Tomoyasu, M.; Osamura, A.; Ohara, M.; Yamamoto, T.; Ito, Y.; Hirano, T. Dapagliflozin decreases small dense low-density lipoprotein-cholesterol and increases high-density lipoprotein 2-cholesterol in patients with type 2 diabetes: Comparison with sitagliptin. Cardiovasc. Diabetol. 2017, 16, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cha, S.A.; Park, Y.M.; Yun, J.S.; Lim, T.S.; Song, K.H.; Yoo, K.D.; Ahn, Y.B.; Ko, S.H. A comparison of effects of DPP-4 inhibitor and SGLT2 inhibitor on lipid profile in patients with type 2 diabetes. Lipids Health Dis. 2017, 16, 58. [Google Scholar] [CrossRef] [Green Version]
- Zinman, B.; Wanner, C.; Lachin, J.M.; Fitchett, D.; Bluhmki, E.; Hantel, S.; Mattheus, M.; Devins, T.; Johansen, O.E.; Woerle, H.J.; et al. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N. Engl. J. Med. 2015, 373, 2117–2128. [Google Scholar] [CrossRef]
- Neal, B.; Perkovic, V.; Mahaffey, K.W.; de Zeeuw, D.; Fulcher, G.; Erondu, N.; Shaw, W.; Law, G.; Desai, M.; Matthews, D.R. Canagliflozin and Cardiovascular and Renal Events in Type 2 Diabetes. N. Engl. J. Med. 2017, 377, 644–657. [Google Scholar] [CrossRef]
- Birkeland, K.I.; Jorgensen, M.E.; Carstensen, B.; Persson, F.; Gulseth, H.L.; Thuresson, M.; Fenici, P.; Nathanson, D.; Nystrom, T.; Eriksson, J.W.; et al. Cardiovascular mortality and morbidity in patients with type 2 diabetes following initiation of sodium-glucose co-transporter-2 inhibitors versus other glucose-lowering drugs (CVD-REAL Nordic): A multinational observational analysis. Lancet Diabetes Endocrinol. 2017, 5, 709–717. [Google Scholar] [CrossRef]
- Persson, F.; Nyström, T.; Jørgensen, M.E.; Carstensen, B.; Gulseth, H.L.; Thuresson, M.; Fenici, P.; Nathanson, D.; Eriksson, J.W.; Norhammar, A.; et al. Dapagliflozin is associated with lower risk of cardiovascular events and all-cause mortality in people with type 2 diabetes (CVD-REAL Nordic) when compared with dipeptidyl peptidase-4 inhibitor therapy: A multinational observational study. Diabetes Obes. Metab. 2018, 20, 344–351. [Google Scholar] [CrossRef]
- Berneis, K.; Rizzo, M.; Stettler, C.; Chappuis, B.; Braun, M.; Diem, P.; Christ, E.R. Comparative effects of rosiglitazone and pioglitazone on fasting and postprandial low-density lipoprotein size and subclasses in patients with Type 2 diabetes. Expert Opin. Pharmacother. 2008, 9, 343–349. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, M.; Christ, E.R.; Rini, G.B.; Spinas, G.A.; Berneis, K. The differential effects of thiazolidindiones on atherogenic dyslipidemia in type 2 diabetes: What is the clinical significance? Expert Opin. Pharmacother. 2008, 9, 2295–2303. [Google Scholar] [CrossRef] [PubMed]
- Liebson, P.R. The thiazolidinedione controversy in cardiovascular risk. Prev. Cardiol. 2010, 13, 209–212. [Google Scholar] [CrossRef] [PubMed]
- Wiviott, S.D.; Raz, I.; Bonaca, M.P.; Mosenzon, O.; Kato, E.T.; Cahn, A.; Silverman, M.G.; Zelniker, T.A.; Kuder, J.F.; Murphy, S.A.; et al. Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2018, 380, 347–357. [Google Scholar] [CrossRef] [PubMed]
- Neal, B.; Perkovic, V.; Matthews, D.R.; Mahaffey, K.W.; Fulcher, G.; Meininger, G.; Erondu, N.; Desai, M.; Shaw, W.; Vercruysse, F.; et al. Rationale, design and baseline characteristics of the CANagliflozin cardioVascular Assessment Study-Renal (CANVAS-R): A randomized, placebo-controlled trial. Diabetes Obes. Metab. 2017, 19, 387–393. [Google Scholar] [CrossRef] [Green Version]
- Jardine, M.J.; Mahaffey, K.W.; Neal, B.; Agarwal, R.; Bakris, G.L.; Brenner, B.M.; Bull, S.; Cannon, C.P.; Charytan, D.M.; de Zeeuw, D.; et al. The Canagliflozin and Renal Endpoints in Diabetes with Established Nephropathy Clinical Evaluation (CREDENCE) Study Rationale, Design, and Baseline Characteristics. Am. J. Nephrol. 2017, 46, 462–472. [Google Scholar] [CrossRef]
- AstraZeneca. A Study to Evaluate the Effect of Dapagliflozin on Renal Outcomes and Cardiovascular Mortality in Patients with Chronic Kidney Disease (Dapa-CKD). Available online: https://clinicaltrials.gov/show/NCT03036150 (accessed on 4 April 2017).
- McMurray, J.J.V.; DeMets, D.L.; Inzucchi, S.E.; Kober, L.; Kosiborod, M.N.; Langkilde, A.M.; Martinez, F.A.; Bengtsson, O.; Ponikowski, P.; Sabatine, M.S.; et al. A trial to evaluate the effect of the sodium-glucose co-transporter 2 inhibitor dapagliflozin on morbidity and mortality in patients with heart failure and reduced left ventricular ejection fraction (DAPA-HF). Eur. J. Heart Fail. 2019, 21, 665–675. [Google Scholar] [CrossRef] [Green Version]
- Boehringer Ingelheim. Empagliflozin Outcome Trial in Patients with Chronic Heart Failure with Reduced Ejection Fraction (EMPEROR-Reduced). Available online: https://clinicaltrials.gov/show/NCT03057977 (accessed on 6 April 2017).
- Patorno, E.; Pawar, A.; Franklin, J.M.; Najafzadeh, M.; Deruaz-Luyet, A.; Brodovicz, K.G.; Sambevski, S.; Bessette, L.G.; Santiago Ortiz, A.J.; Kulldorff, M.; et al. Empagliflozin and the Risk of Heart Failure Hospitalization in Routine Clinical Care. Circulation 2019, 139, 2822–2830. [Google Scholar] [CrossRef]
- Cefalo, C.M.A.; Cinti, F.; Moffa, S.; Impronta, F.; Sorice, G.P.; Mezza, T.; Pontecorvi, A.; Giaccari, A. Sotagliflozin, the first dual SGLT inhibitor: Current outlook and perspectives. Cardiovasc. Diabetol. 2019, 18, 20. [Google Scholar] [CrossRef] [Green Version]
- Yandrapalli, S.; Aronow, W.S. Cardiovascular benefits of the newer medications for treating type 2 diabetes mellitus. J. Thorac. Dis. 2017, 9, 2124–2134. [Google Scholar] [CrossRef] [Green Version]
- Scirica, B.M.; Bhatt, D.L.; Braunwald, E.; Steg, P.G.; Davidson, J.; Hirshberg, B.; Ohman, P.; Frederich, R.; Wiviott, S.D.; Hoffman, E.B.; et al. Saxagliptin and cardiovascular outcomes in patients with type 2 diabetes mellitus. N. Engl. J. Med. 2013, 369, 1317–1326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- White, W.B.; Cannon, C.P.; Heller, S.R.; Nissen, S.E.; Bergenstal, R.M.; Bakris, G.L.; Perez, A.T.; Fleck, P.R.; Mehta, C.R.; Kupfer, S.; et al. Alogliptin after acute coronary syndrome in patients with type 2 diabetes. N. Engl. J. Med. 2013, 369, 1327–1335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green, J.B.; Bethel, M.A.; Armstrong, P.W.; Buse, J.B.; Engel, S.S.; Garg, J.; Josse, R.; Kaufman, K.D.; Koglin, J.; Korn, S.; et al. Effect of Sitagliptin on Cardiovascular Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2015, 373, 232–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenstock, J.; Perkovic, V.; Johansen, O.E.; Cooper, M.E.; Kahn, S.E.; Marx, N.; Alexander, J.H.; Pencina, M.; Toto, R.D.; Wanner, C.; et al. Effect of Linagliptin vs Placebo on Major Cardiovascular Events in Adults With Type 2 Diabetes and High Cardiovascular and Renal Risk: The CARMELINA Randomized Clinical Trial. JAMA 2019, 321, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Home, P.; Shankar, R.R.; Gantz, I.; Iredale, C.; O’Neill, E.A.; Jain, L.; Pong, A.; Suryawanshi, S.; Engel, S.S.; Kaufman, K.D.; et al. A randomized, double-blind trial evaluating the efficacy and safety of monotherapy with the once-weekly dipeptidyl peptidase-4 inhibitor omarigliptin in people with type 2 diabetes. Diabetes Res. Clin. Pract. 2018, 138, 253–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gantz, I.; Chen, M.; Suryawanshi, S.; Ntabadde, C.; Shah, S.; O’Neill, E.A.; Engel, S.S.; Kaufman, K.D.; Lai, E. A randomized, placebo-controlled study of the cardiovascular safety of the once-weekly DPP-4 inhibitor omarigliptin in patients with type 2 diabetes mellitus. Cardiovasc. Diabetol. 2017, 16, 112. [Google Scholar] [CrossRef] [Green Version]
- McMurray, J.J.; Gerstein, H.C.; Holman, R.R.; Pfeffer, M.A. Heart failure: A cardiovascular outcome in diabetes that can no longer be ignored. Lancet Diabetes Endocrinol. 2014, 2, 843–851. [Google Scholar] [CrossRef]
- Fitchett, D.; Zinman, B.; Wanner, C.; Lachin, J.M.; Hantel, S.; Salsali, A.; Johansen, O.E.; Woerle, H.J.; Broedl, U.C.; Inzucchi, S.E. Heart failure outcomes with empagliflozin in patients with type 2 diabetes at high cardiovascular risk: Results of the EMPA-REG OUTCOME(R) trial. Eur. Heart J. 2016, 37, 1526–1534. [Google Scholar] [CrossRef] [Green Version]
- Wanner, C.; Inzucchi, S.E.; Lachin, J.M.; Fitchett, D.; von Eynatten, M.; Mattheus, M.; Johansen, O.E.; Woerle, H.J.; Broedl, U.C.; Zinman, B. Empagliflozin and Progression of Kidney Disease in Type 2 Diabetes. N. Engl. J. Med. 2016, 375, 323–334. [Google Scholar] [CrossRef]
- Ferrannini, E.; Mark, M.; Mayoux, E. CV Protection in the EMPA-REG OUTCOME Trial: A “Thrifty Substrate” Hypothesis. Diabetes Care 2016, 39, 1108–1114. [Google Scholar] [CrossRef] [Green Version]
- Mudaliar, S.; Alloju, S.; Henry, R.R. Can a Shift in Fuel Energetics Explain the Beneficial Cardiorenal Outcomes in the EMPA-REG OUTCOME Study? A Unifying Hypothesis. Diabetes Care 2016, 39, 1115–1122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zannad, F.; Cannon, C.P.; Cushman, W.C.; Bakris, G.L.; Menon, V.; Perez, A.T.; Fleck, P.R.; Mehta, C.R.; Kupfer, S.; Wilson, C.; et al. Heart failure and mortality outcomes in patients with type 2 diabetes taking alogliptin versus placebo in EXAMINE: A multicentre, randomised, double-blind trial. Lancet 2015, 385, 2067–2076. [Google Scholar] [CrossRef]


{kind=link}
| Class Drug | Agent | Administration | Mechanism of Action | Reference |
|---|---|---|---|---|
| Biguanides | Metformin | oral | ↑ Insulin sensitivity by activating Adenosine Mono Phosphate-activated protein kinase (AMP-k) ↓ Hepatic glucose production | [2] |
| Thiazolidinediones | Pioglitazone | oral | ↑ Insulin sensitivity by activation of Peroxisome Proliferator Activated Receptor gamma (PPAR-γ) ↓ Peripheral glucose uptake | [4,5,6] |
| Sulfonylureas | Glimepiride Gliclazide | oral oral | ↑ Insulin secretion | [1,5] |
| Insulin | Glargine Degludec | injective | ↑ Glucose disposal ↓ Hepatic glucose production | [7,8] |
| Dipeptidyl Peptidase-4 Inhibitors (DPP4-is) | Sitagliptin Linagliptin Omarigliptin | Oral oral oral | ↓ Half-life and promoting the insulinotropism of Glucagon Like Peptide-1(GLP-1) ↑ Insulin secretion (glucose-dependent) ↓ Glucagon secretion (glucose-dependent) Enzymatic activities against chemotactic molecules and hormones modulating the intricate inflammatory, vascular and immune processes Improving glycemic control ↓ Total cholesterol and triglyceride levels Improve weight neutrality ↓ Risk factors Ameliorating cardiac function and vascular repair Block cleavage of many circulating peptides | [9,10] |
| Glucagon Like Peptide-1 Receptor Agonists (GLP-1RAs) | Liraglutide Exenatide Semaglutide Lixisenatide Albiglutide Dulaglutide | Injective Injective oral / injective Injective Injective Injective | ↑ Insulin secretion (glucose-dependent) ↑ ß-cell proliferation ↑ Insulin biosynthesis ↓ ß-cell apoptosis ↓ Glucagon secretion (glucose-dependent) from pancreatic α-cells ↓ Rate of endogenous glucose production ↓ Gastric emptying ↑ Satiety ↓ Food intake ↓ Weight loss Improved blood pressure ↑ Control of cholesterol/dyslipidemia ↑ Low Density Lipoproteins particles oxidised (ox-LDL) ↓ Carotid Intima Media Thickness (CIMT) ↓ Flow-Mediated Dilation (FMD) ↓ Artery endothelial dysfunctions ↓ Atherosclerotic risk factors direct effects on both plaque initiation/formation and progression | [11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40] |
| Sodium Glucose coTransporter-2 Inhibitors (SGLT2-is) | Empagliflozin Canagliflozin Dapagliflozin | Oral oral oral | ↓ Renal threshold for glucose reabsorption increasing glycosuria Modify insulin sensitivity lower insulin requirements ↓ Body weight ↓ Blood pressure ↓ Extracellular volume little changes in High Density Lipoprotein-Cholesterol (HDL-C), triglyceride, and Low Density Lipoproteins-Cholesterol (LDL-C) ↓ Small dense LDL-C | [41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73] |
| Agent | Study | Patients (N. and Type) | CVD-Reduction (Hazard Ratio HR, Confidence Interval CI, and p-Value) | Reference |
|---|---|---|---|---|
| Metformin | UK Prospective Diabetes Study (UKPDS study) | 4075 overweight patients with newly diagnosed type 2 diabetes recruited in 15 centres | −32% HR (95% CI 13-47) p = 0.002 | [2] |
| Pioglitazone | Prospective Pioglitazone Clinical Trial in Macrovascular Events (PROactive) | 5238 patients with type 2 diabetes who had evidence of macrovascular disease | −16% HR 0.84 (95% CI 0.72–0.98) p = 0.027 | [4] |
| Pioglitazone | Thiazolidinediones or Sulfonylureas Cardiovascular Accidents Intervention (TOSCA) | 3028 patients with type 2 diabetes inadequately controlled with metformin monotherapy | HR 0.96 (95% CI 0.74–1.26) p = 0.79 | [5] |
| Pioglitazone | Insulin Resistance Intervention After Stroke (IRIS) | 3876 participants and 12% with a history of coronary artery disease | −24% HR 0.71 (95% CI 0.54–0.94) p = 0.02 | [6] |
| Degludec | Efficacy and Safety of Degludec versus Glargine in Type 2 Diabetes (DEVOTE) | 7637 patients with type 2 diabetes; 3818 patients with insulin degludec and 3819 patients with insulin glargine U100 | HR 0.91 (95% CI 0.78–1.06) p = 0.21 | [8] |
| Liraglutide | Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results-A Long Term Evaluation (LEADER) | 9340 patients with type 2 diabetes with a previous cardiovascular problem or chronic heart failure or at least one cardiovascular risk factor | −13.9% HR 0.87 (95% CI 0.78–0.97) p < 0.001 | [15] |
| Exenatide LAR | Exenatide Study of Cardiovascular Event Lowering (EXSCEL) | 14,752 patients; 10,782 had previous cardiovascular disease | −12% HR 0.91 (95% CI 0.83–1.00) p = 0.061 | [19] |
| Semaglutide | Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes CardioVascular Outcome Trial-CVOT (SUSTAIN-6) | 3297 patients with type 2 diabetes | −6.6% HR 0.74 (95% CI 0.58–0.95) p < 0.001 | [30] |
| Lixisenatide | Evaluation of Lixisenatide in Acute Coronary Syndrome (ELIXA) | 6068 patients with type 2 diabetes who had had a myocardial infarction or who had been hospitalized for unstable angina within the previous 180 days | HR 1.02 (95% CI 0.89–1.17) p = 0.81 | [32] |
| Albiglutide | Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (HARMONY 1-8 trials) | 21,135 patients. Most patients had, or were at high risk for, cardiovascular disease. | −25% HR 0.78 (95% CI 0.68–0.90) p < 0.0001 | [35,36] |
| Dulaglutide | Dulaglutide on Major Cardiovascular Events in Patients with Type 2 Diabetes: Researching Cardiovascular Events with a Weekly INcretin in Diabetes (REWIND) | 9901 participants occurred in 370 sites located in 24 countries with type 2 diabetes; 31% had prior cardiovascular disease | HR 0.88 (95% CI 0.79–0.99) p = 0.026 | [37] |
| Empagliflozin | Empagliflozin Cardiovascular Outcome Event Trial in Type 2 Diabetes Mellitus Patients (EMPA-REG CT) | 22,830 diabetic patients | −38%; HR 0.62 (95% CI, 0.49–0.77) p < 0.001 | [47] |
| Canagliflozin | Canagliflozin Cardiovascular Assessment Study (CANVAS) | 10,142 participants with type 2 diabetes and high cardiovascular risk | HR 0.86 (95% CI, 0.75–0.97) p < 0.001 | [48] |
| Dapagliflozin | Comparative Effectiveness of Cardiovascular Outcomes in New Users of SGLT-2 Inhibitors (CVD-REAL Nordic trial) | 40,908 patients with type 2 diabetes; 23% had cardiovascular disease | HR 0.59 (95% CI, 0.49–0.72) p < 0.001 | [49,50] |
| Dapagliflozin | Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes (DECLARE) | 17,160 patients, including 10,186 without atherosclerotic cardiovascular disease | HR 0.83 (95% CI, 0.73–0.95) p = 0.005 | [54] |
| Sitagliptin | Sitagliptin Cardiovascular Outcomes (TECOS) | 14,671 patients with type 2 diabetes and cardiovascular disease | HR 0.98 (95% CI, 0.88–1.09) p < 0.001 | [65] |
| Linagliptin | Cardiovascular and Renal Microvascular Outcome Study with Linagliptin (CARMELINA) | 6991 diabetic patients with high cardiovascular risk | HR 1.02 (95% CI, 0.89–1.17) p < 0.001 | [66] |
| Omarigliptin | A Study to Assess Cardiovascular Outcomes Following Treatment with Omarigliptin (OMNeON study) | 4202 patients with type 2 diabetes mellitus and established cardiovascular disease | HR 1.00 (95% CI 0.77–1.29) p = 0.77 | [67,68] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patti, A.M.; Rizvi, A.A.; Giglio, R.V.; Stoian, A.P.; Ligi, D.; Mannello, F. Impact of Glucose-Lowering Medications on Cardiovascular and Metabolic Risk in Type 2 Diabetes. J. Clin. Med. 2020, 9, 912. https://doi.org/10.3390/jcm9040912
Patti AM, Rizvi AA, Giglio RV, Stoian AP, Ligi D, Mannello F. Impact of Glucose-Lowering Medications on Cardiovascular and Metabolic Risk in Type 2 Diabetes. Journal of Clinical Medicine. 2020; 9(4):912. https://doi.org/10.3390/jcm9040912
Chicago/Turabian StylePatti, Angelo Maria, Ali A Rizvi, Rosaria Vincenza Giglio, Anca Pantea Stoian, Daniela Ligi, and Ferdinando Mannello. 2020. "Impact of Glucose-Lowering Medications on Cardiovascular and Metabolic Risk in Type 2 Diabetes" Journal of Clinical Medicine 9, no. 4: 912. https://doi.org/10.3390/jcm9040912