Sequential Combination of FIB-4 Followed by M2BPGi Enhanced Diagnostic Performance for Advanced Hepatic Fibrosis in an Average Risk Population

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
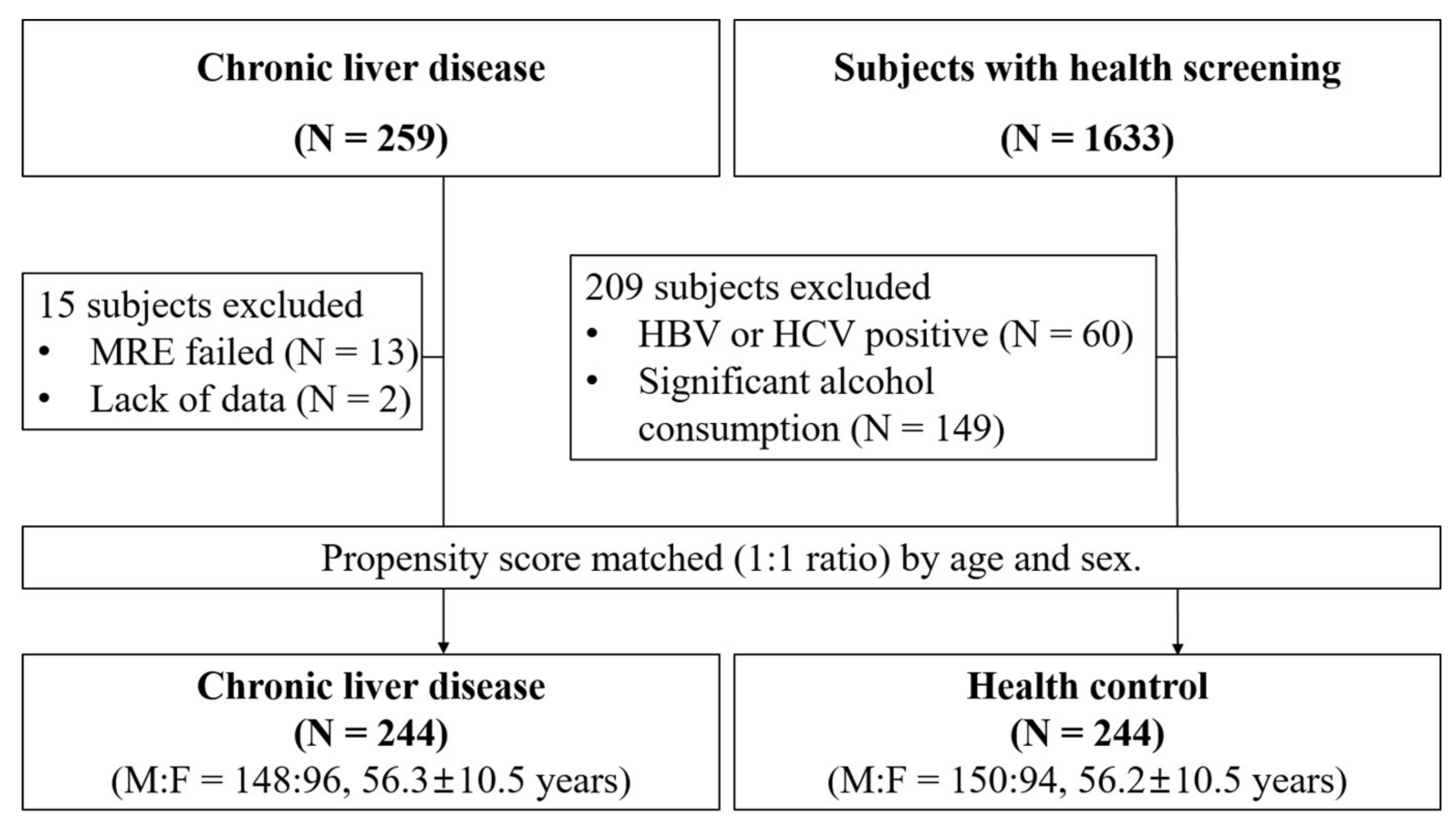
2.2. Healthy Cohort and Propensity Score Matching
2.3. Chronic Liver Disease Cohort
2.4. Inclusion and Exclusion Criteria
2.5. Clinical Parameters and Estimated Formulae For Hepatic Fibrosis
2.6. Measurement of Serum Mac-2 Binding Protein Glycan Isomer Value
2.7. Acquisitions of Magnetic Resonance Elastography (MRE)
2.8. Liver Stiffness and Liver Fat Measurement
2.9. Statistical Analysis
3. Results
3.1. Baseline Characteristics
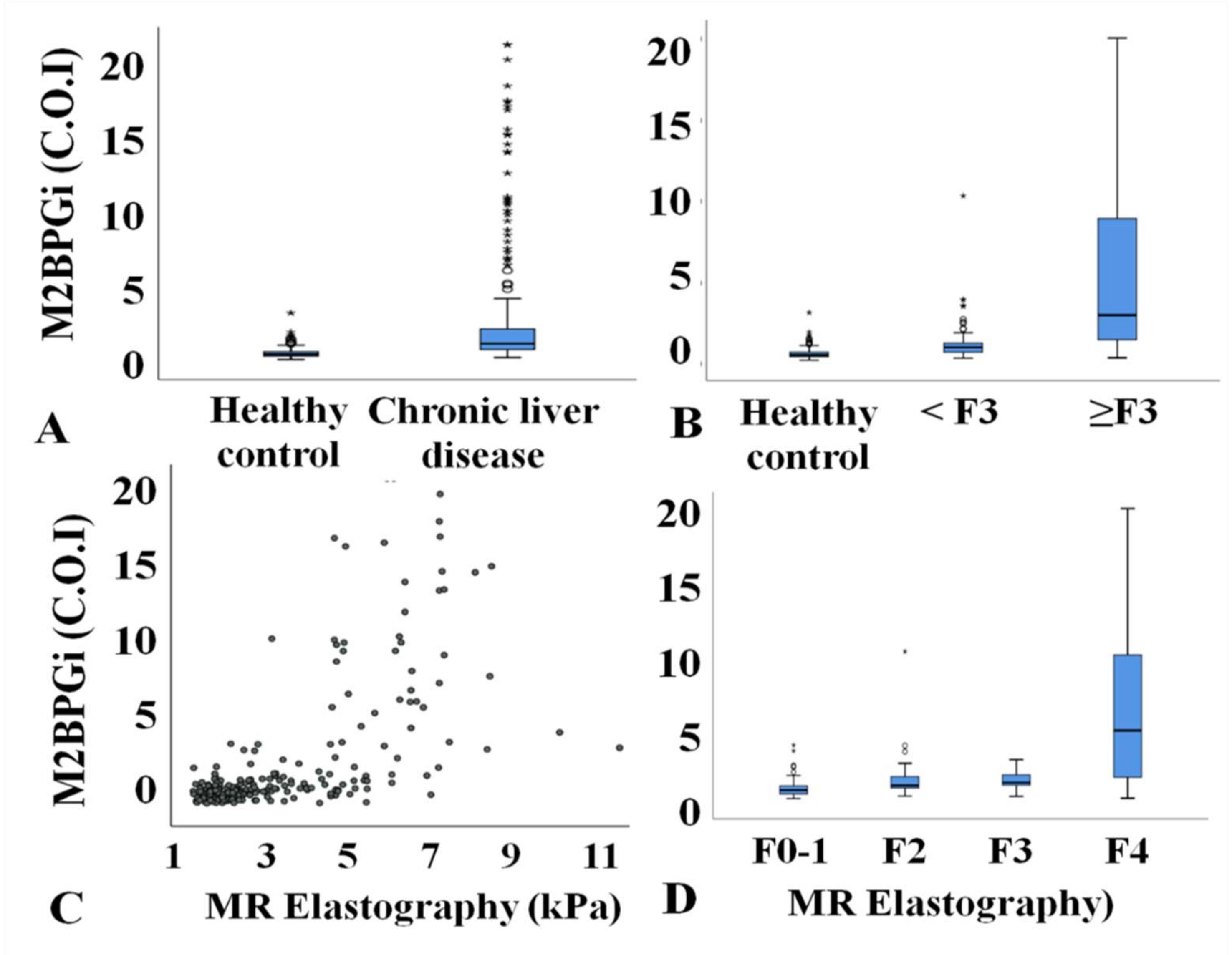
3.2. Clinical Parameters According to Disease Severity
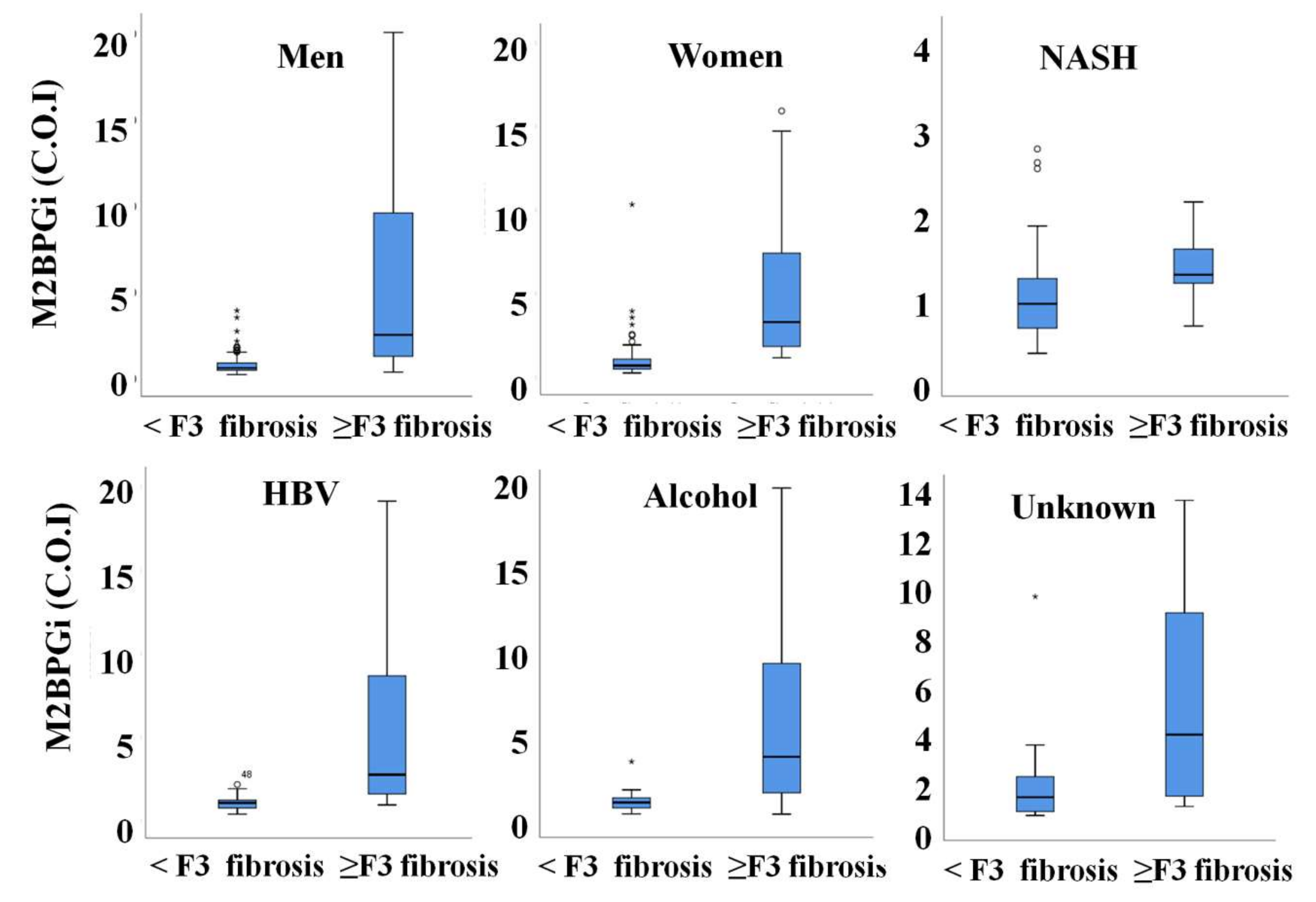
3.3. M2BPGi Value in Advanced Hepatic Fibrosis According to Sex and Cause of Disease
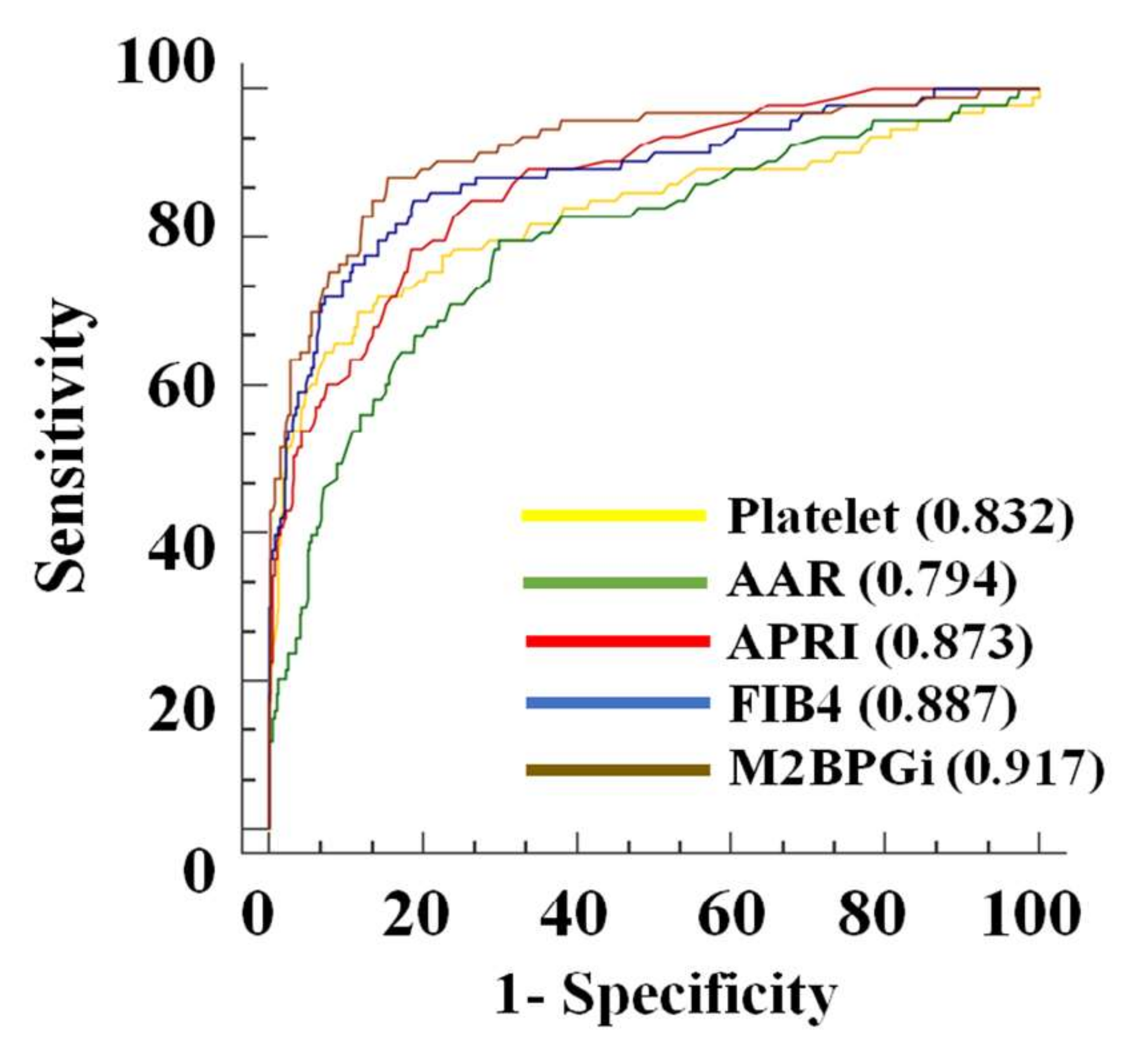
3.4. M2BPGi Performance for Diagnosis of Advanced Hepatic Fibrosis
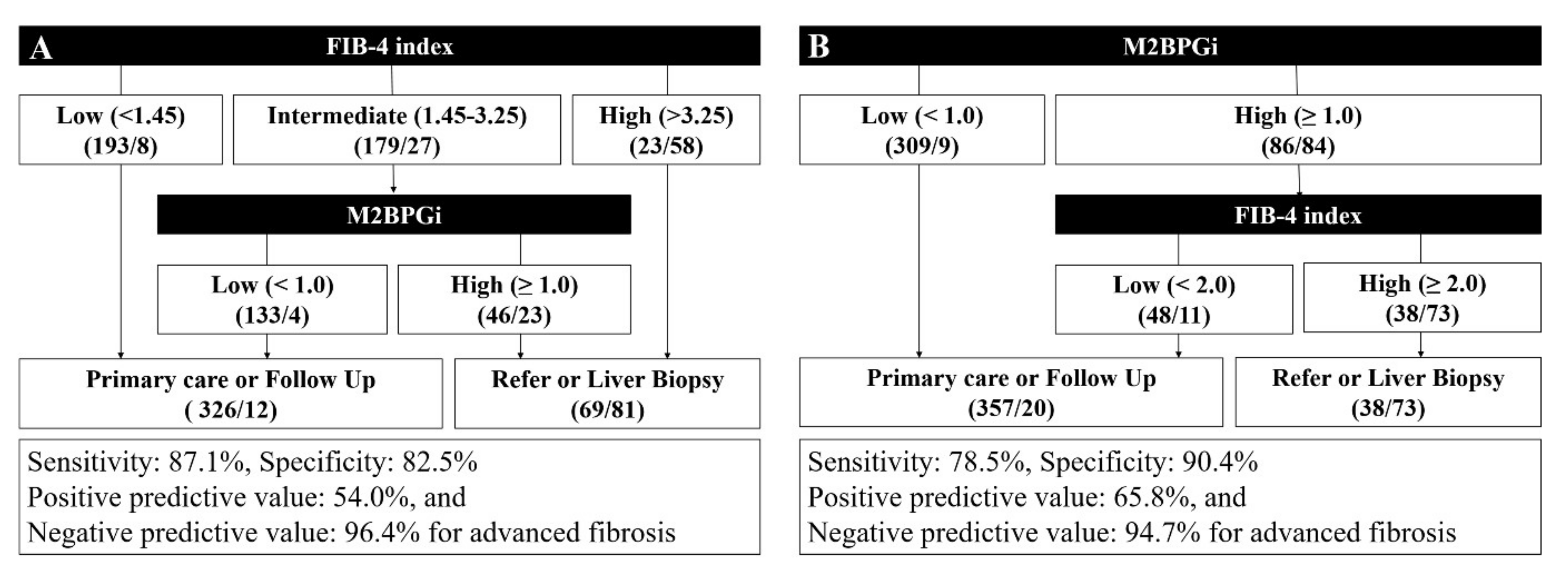
3.5. Proposal of a Diagnostic Algorithm for Advanced Liver Fibrosis in an Average Risk Group
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Informed consent statement
References
- Kang, K.A.; Jun, D.W.; Kim, M.S.; Kwon, H.-J.; Nguyen, M.H. Prevalence of significant hepatic fibrosis using magnetic resonance elastography in a health check-up clinic population. Aliment. Pharmacol. Ther. 2020, 51, 388–396. [Google Scholar] [CrossRef] [PubMed]
- Martínez, S.M.; Crespo, G.; Navasa, M.; Forns, X. Noninvasive assessment of liver fibrosis. Hepatology 2010, 53, 325–335. [Google Scholar] [CrossRef] [PubMed]
- Sumida, Y.; Nakajima, A.; Itoh, Y. Limitations of liver biopsy and non-invasive diagnostic tests for the diagnosis of nonalcoholic fatty liver disease/nonalcoholic steatohepatitis. World J. Gastroenterol. 2014, 20, 475–485. [Google Scholar] [CrossRef] [PubMed]
- Xiao, G.; Zhu, S.; Xiao, X.; Yan, L.; Yang, J.; Wu, G. Comparison of laboratory tests, ultrasound, or magnetic resonance elastography to detect fibrosis in patients with nonalcoholic fatty liver disease: A meta-analysis. Hepatology 2017, 66, 1486–1501. [Google Scholar] [CrossRef] [PubMed]
- McPherson, S.; Henderson, E.; Stewart, S.; Burt, A.; Day, C.P. Simple non-invasive fibrosis scoring systems can reliably exclude advanced fibrosis in patients with non-alcoholic fatty liver disease. Gut 2010, 59, 1265–1269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sumida, Y.; Yoneda, M.; Hyogo, H.; Itoh, Y.; Ono, M.; Fujii, H.; Eguchi, Y.; Suzuki, Y.; Aoki, N.; Kanemasa, K.; et al. Validation of the FIB4 index in a Japanese nonalcoholic fatty liver disease population. BMC Gastroenterol. 2012, 12, 2. [Google Scholar] [CrossRef] [Green Version]
- Vilar-Gomez, E.; Chalasani, N. Non-invasive assessment of non-alcoholic fatty liver disease: Clinical prediction rules and blood-based biomarkers. J. Hepatol. 2018, 68, 305–315. [Google Scholar] [CrossRef]
- Davyduke, T.; Tandon, P.; Al-Karaghouli, M.; Abraldes, J.G.; Ma, M.M. Impact of Implementing a “FIB-4 First” Strategy on a Pathway for Patients With NAFLD Referred From Primary Care. Hepatol. Commun. 2019, 3, 1322–1333. [Google Scholar] [CrossRef] [Green Version]
- Demir, M.; Lang, S.; Schlattjan, M.; Drebber, U.; Wedemeyer, I.; Nierhoff, D.; Kaul, I.; Sowa, J.; Canbay, A.; Töx, U.; et al. NIKEI: A New Inexpensive and Non-Invasive Scoring System to Exclude Advanced Fibrosis in Patients with NAFLD. PLoS ONE 2013, 8, e58360. [Google Scholar] [CrossRef]
- Kuno, A.; Ikehara, Y.; Tanaka, Y.; Ito, K.; Matsuda, A.; Sekiya, S.; Hige, S.; Sakamoto, M.; Kage, M.; Mizokami, M.; et al. A serum “sweet-doughnut” protein facilitates fibrosis evaluation and therapy assessment in patients with viral hepatitis. Sci. Rep. 2013, 3, 1065. [Google Scholar] [CrossRef]
- Toshima, T.; Shirabe, K.; Ikegami, T.; Yoshizumi, T.; Kuno, A.; Togayachi, A.; Gotoh, M.; Narimatsu, H.; Korenaga, M.; Mizokami, M.; et al. A novel serum marker, glycosylated Wisteria floribunda agglutinin-positive Mac-2 binding protein (WFA+-M2BP), for assessing liver fibrosis. J. Gastroenterol. 2014, 50, 76–84. [Google Scholar] [CrossRef]
- Kamada, Y.; Ono, M.; Hyogo, H.; Fujii, H.; Sumida, Y.; Yamada, M.; Mori, K.; Tanaka, S.; Maekawa, T.; Ebisutani, Y.; et al. Use of Mac-2 binding protein as a biomarker for nonalcoholic fatty liver disease diagnosis. Hepatol. Commun. 2017, 1, 780–791. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, H.; Enomoto, H.; Yoh, K.; Iwata, Y.; Sakai, Y.; Kishino, K.; Ikeda, N.; Takashima, T.; Aizawa, N.; Takata, R.; et al. Combined albumin-bilirubin grade and Mac-2 binding protein glycosylation isomer as a useful predictor in compensated liver cirrhosis. Medicine 2019, 98, e18366. [Google Scholar] [CrossRef] [PubMed]
- Sato, S.; Genda, T.; Ichida, T.; Amano, N.; Sato, S.; Murata, A.; Tsuzura, H.; Narita, Y.; Kanemitsu, Y.; Hirano, K.; et al. Prediction of Hepatocellular Carcinoma Development after Hepatitis C Virus Eradication Using Serum Wisteria floribunda Agglutinin-Positive Mac-2-Binding Protein. Int. J. Mol. Sci. 2016, 17, 2143. [Google Scholar] [CrossRef]
- Nishikawa, H.; Hasegawa, K.; Ishii, A.; Takata, R.; Enomoto, H.; Yoh, K.; Kishino, K.; Shimono, Y.; Iwata, Y.; Nakano, C.; et al. A proposed predictive model for advanced fibrosis in patients with chronic hepatitis B and its validation. Medicine 2016, 95, e4679. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, H.; Takata, R.; Enomoto, H.; Kazunori, Y.; Kishino, K.; Shimono, Y.; Iwata, Y.; Hasegawa, K.; Nakano, C.; Nishimura, T.; et al. Proposal of a predictive model for advanced fibrosis containing Wisteria floribunda agglutinin-positive Mac-2-binding protein in chronic hepatitis C. Hepatol. Res. 2016, 47, 74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeh, M.-L.; Dai, C.-Y.; Lin, I.-H.; Liang, P.-C.; Hsieh, M.-H.; Lin, Z.-Y.; Chen, S.-C.; Huang, J.-F.; Chen, J.-J.; Yu, M.-L.; et al. Wisteria floribunda agglutinin-positive Mac-2-binding protein in the prediction of disease severity in chronic hepatitis B patients. PLoS ONE 2019, 14, e0220663. [Google Scholar] [CrossRef] [Green Version]
- Hsu, C.; Caussy, C.; Imajo, K.; Chen, J.; Singh, S.; Kaulback, K.; Le, M.-D.; Hooker, J.; Tu, X.; Bettencourt, R.; et al. Magnetic Resonance vs Transient Elastography Analysis of Patients With Nonalcoholic Fatty Liver Disease: A Systematic Review and Pooled Analysis of Individual Participants. Clin. Gastroenterol. Hepatol. 2019, 17, 630–637.e8. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.; Jun, D.W.; Kang, B.-K.; Nam, E.; Chang, M.; Kim, M.; Song, S.; Yoon, B.C.; Lee, H.L.; Lee, O.Y.; et al. Estimating of hepatic fat amount using MRI proton density fat fraction in a real practice setting. Medicine 2017, 96, e7778. [Google Scholar] [CrossRef]
- Shima, T.; Sakai, K.; Oya, H.; Katayama, T.; Mitsumoto, Y.; Mizuno, M.; Kanbara, Y.; Okanoue, T. Diagnostic accuracy of combined biomarker measurements and vibration-controlled transient elastography (VCTE) for predicting fibrosis stage of non-alcoholic fatty liver disease. J. Gastroenterol. 2019, 55, 100–112. [Google Scholar] [CrossRef]
- Jiang, Z.G.; Tapper, E.B. Cost Saving or Cost Effective? Unanswered Questions in the Screening of Patients With Nonalcoholic Fatty Liver Disease. Hepatol. Commun. 2019, 3, 1293–1295. [Google Scholar] [CrossRef]
- Srivastava, A.; Gailer, R.; Tanwar, S.; Trembling, P.; Parkes, J.; Rodger, A.; Suri, D.; Thorburn, U.; Sennett, K.; Morgan, S.; et al. Prospective evaluation of a primary care referral pathway for patients with non-alcoholic fatty liver disease. J. Hepatol. 2019, 71, 371–378. [Google Scholar] [CrossRef] [Green Version]
- Anstee, Q.M.; Lawitz, E.J.; Alkhouri, N.; Wong, V.W.-S.; Romero-Gomez, M.; Okanoue, T.; Trauner, M.; Kersey, K.; Li, G.; Han, L.; et al. Noninvasive Tests Accurately Identify Advanced Fibrosis due to NASH: Baseline Data From the STELLAR Trials. Hepatology 2019, 70, 1521–1530. [Google Scholar] [CrossRef] [PubMed]
- Boursier, J.; Guillaume, M.; Leroy, V.; Irlès, M.; Roux, M.; Lannes, A.; Foucher, J.; Zuberbuhler, F.; Delabaudière, C.; Barthelon, J.; et al. New sequential combinations of non-invasive fibrosis tests provide an accurate diagnosis of advanced fibrosis in NAFLD. J. Hepatol. 2019, 71, 389–396. [Google Scholar] [CrossRef] [PubMed]
- Imajo, K.; Kessoku, T.; Honda, Y.; Tomeno, W.; Ogawa, Y.; Mawatari, H.; Fujita, K.; Yoneda, M.; Taguri, M.; Hyogo, H.; et al. Magnetic Resonance Imaging More Accurately Classifies Steatosis and Fibrosis in Patients With Nonalcoholic Fatty Liver Disease Than Transient Elastography. Gastroenterology 2016, 150, 626–637.e7. [Google Scholar] [CrossRef] [Green Version]
- Morisaka, H.; Motosugi, U.; Ichikawa, S.; Nakazawa, T.; Kondo, T.; Funayama, S.; Matsuda, M.; Ichikawa, T.; Onishi, H. Magnetic resonance elastography is as accurate as liver biopsy for liver fibrosis staging. J. Magn. Reson. Imaging 2017, 47, 1268–1275. [Google Scholar] [CrossRef] [PubMed]
- Newsome, P.N.; Cramb, R.; Davison, S.M.; Dillon, J.; Foulerton, M.; Godfrey, E.M.; Hall, R.; Harrower, U.; Hudson, M.; Langford, A.; et al. Guidelines on the management of abnormal liver blood tests. Gut 2017, 67, 6–19. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Age-Sex Matched Healthy Subject (Group 1) | Chronic Hepatitis without Advanced Fibrosis (Group 2) | Chronic Hepatitis with Advanced Fibrosis (Group 3) | p-Value | |||
|---|---|---|---|---|---|---|---|
| All | Group 1 vs. 2 | Group 1 vs. 3 | Group 2 vs. 3 | ||||
| Number | 244 | 151 | 93 | ||||
| Age (years) | 56 ± 10.5 | 56 ± 10.3 | 57 ± 10.7 | 0.420 | NA | NA | NA |
| Sex | 0.006 | ||||||
| Male | 150 | 81 | 69 | ||||
| Female | 97 | 70 | 24 | ||||
| Albumin (g/㎗) | 4.4 (4.3–4.6) | 4.4 (4.2–4.5) | 3.8 (3.3–4.3) | <0.001 | 0.222 | <0.001 | <0.001 |
| Total bilirubin (mg/㎗) | 0.82 (0.65–1.03) | 0.73 (0.58–0.97) | 1.30 (0.84–2.32) | <0.001 | 0.015 | <0.001 | <0.001 |
| AST (U/L) | 26 (21–32) | 35 (26–52) | 52 (34–83) | <0.001 | <0.001 | <0.001 | <0.001 |
| ALT (U/L) | 21 (16–33) | 28 (19–41) | 26 (17–37) | 0.001 | <0.001 | 0.099 | 0.174 |
| PT (INR) | NA | 1.50 (1.00–1.08) | 1.19 (1.07–1.38) | <0.001 | NA | NA | NA |
| Liver fat fraction (%) | NA | 3.9 (2.1–12.3) | 3.0 (1.9–6.7) | 0.015 | NA | NA | NA |
| Liver stiffness (kPa) | NA | 2.40 (2.05–2.77) | 5.59 (4.78–7.00) | <0.001 | NA | NA | NA |
| Platelet count (x109/L) | 235 (206–270) | 219 (177–258) | 127 (83–189) | <0.001 | 0.002 | <0.001 | <0.001 |
| AAR | 1.17 (0.95–1.44) | 1.26 (0.94–1.70) | 1.90 (1.48–2.57) | <0.001 | 0.037 | <0.001 | <0.001 |
| APRI | 0.22 (0.17–0.29) | 0.53 (0.24–0.52) | 0.80 (0.44–1.89) | <0.001 | <0.001 | <0.001 | <0.001 |
| FIB4 | 1.33 (1.02–1.72) | 1.81 (1.35–2.45) | 4.55 (2.66–8.63) | <0.001 | <0.001 | <0.001 | <0.001 |
| M2BPGi (C.O.I) | 0.48 (0.37–0.65) | 0.94 (0.65–1.21) | 2.93 (1.42–8.89) | <0.001 | <0.001 | <0.001 | <0.001 |
| Univariate Analysis | Multivariable Analysis | |||||
|---|---|---|---|---|---|---|
| Odds Ratio | 95% CI | p-Value | Odds Ratio | 95% CI | p-Value | |
| Age | 1.01 | 0.99–1.04 | 0.251 | |||
| Sex [male] | 2.08 | 1.26–3.46 | 0.004 | 2.04 | 1.02–5.23 | 0.046 |
| Albumin | 0.05 | 0.03–0.10 | <0.001 | 0.24 | 0.09–0.62 | 0.003 |
| Total bilirubin | 8.97 | 5.01–16.04 | <0.001 | 2.90 | 1.20–7.04 | 0.018 |
| AST | 1.03 | 1.02–1.04 | <0.001 | 1.01 | 1.00–1.02 | 0.016 |
| ALT | 1.00 | 0.99–1.01 | 0.371 | |||
| Platelet | 0.98 | 0.97–0.98 | <0.001 | 0.99 | 0.99–1.00 | <0.001 |
| M2BPGi | 3.74 | 2.61–5.37 | <0.001 | 2.40 | 1.55–3.71 | <0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, M.; Jun, D.W.; Park, H.; Kang, B.-K.; Sumida, Y. Sequential Combination of FIB-4 Followed by M2BPGi Enhanced Diagnostic Performance for Advanced Hepatic Fibrosis in an Average Risk Population. J. Clin. Med. 2020, 9, 1119. https://doi.org/10.3390/jcm9041119
Kim M, Jun DW, Park H, Kang B-K, Sumida Y. Sequential Combination of FIB-4 Followed by M2BPGi Enhanced Diagnostic Performance for Advanced Hepatic Fibrosis in an Average Risk Population. Journal of Clinical Medicine. 2020; 9(4):1119. https://doi.org/10.3390/jcm9041119
Chicago/Turabian StyleKim, Mimi, Dae Won Jun, Huiyul Park, Bo-Kyeong Kang, and Yoshio Sumida. 2020. "Sequential Combination of FIB-4 Followed by M2BPGi Enhanced Diagnostic Performance for Advanced Hepatic Fibrosis in an Average Risk Population" Journal of Clinical Medicine 9, no. 4: 1119. https://doi.org/10.3390/jcm9041119