Frailty Parameters, Morbidity and Mortality in Older Adults with Cancer: A Structural Equation Modelling Approach Based on the Fried Phenotype

 and
and
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Population
2.2. Cancer-Related and Demographic Data
2.3. Geriatric Assessment (GA)
2.4. Definition of Frailty
3. Covariates
3.1. Adverse Health Outcomes
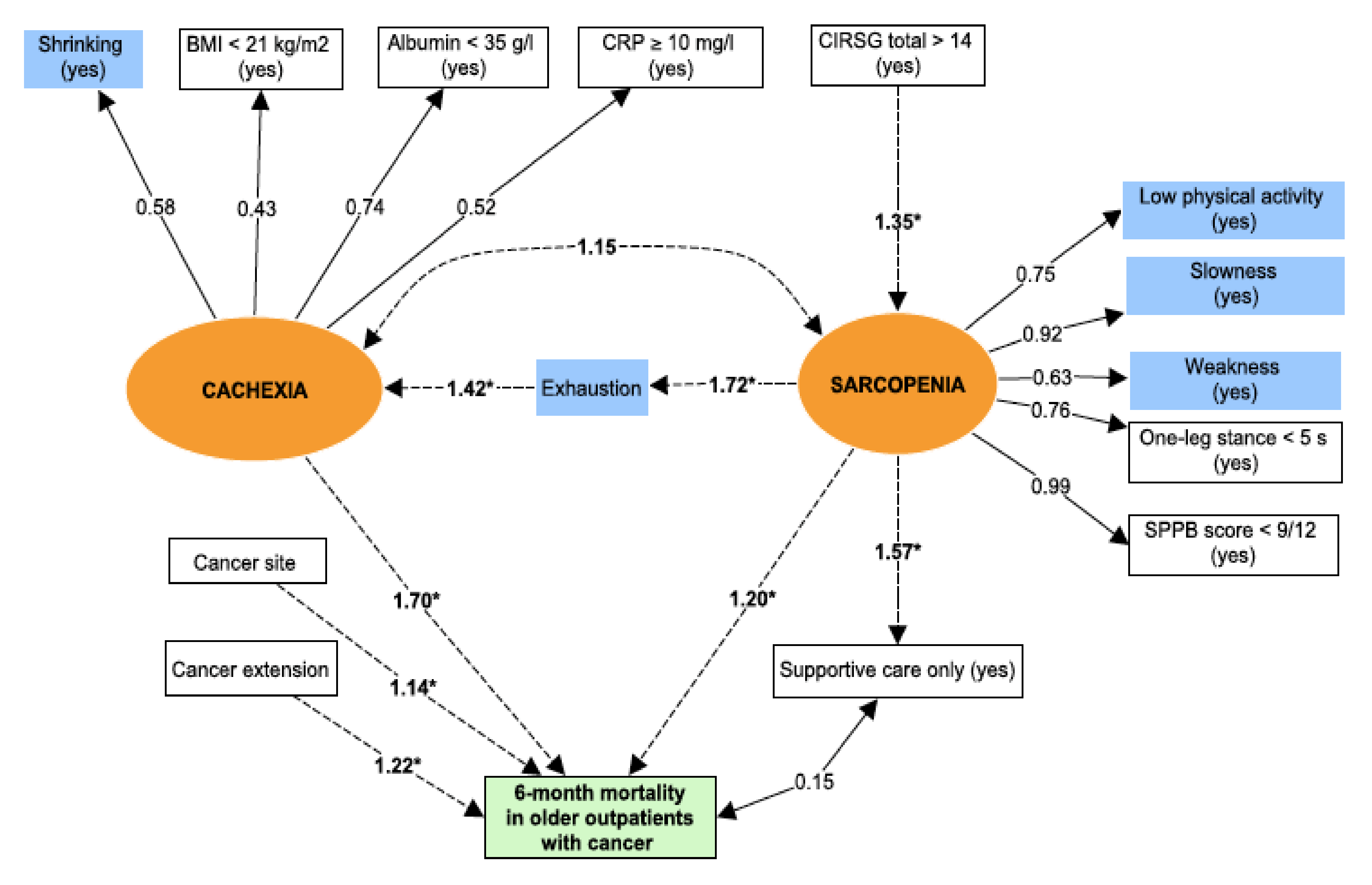
3.2. Prespecified Structural Equation Modelling (SEM) of the Frailty Phenotype
3.3. Statistical Analyses
4. Results
4.1. Patients
4.2. Baseline Characteristics of Patients and the Frailty Phenotype
4.3. Correlations between Frailty Criteria and the Other Observed Variables
4.4. Goodness of Fit
4.5. Pathways of the Frailty Phenotype Leading to Mortality
4.6. Frailty Phenotype Pathways Leading to Morbidity
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Walston, J.; Hadley, E.C.; Ferrucci, L.; Guralnik, J.M.; Newman, A.B.; Studenski, S.A.; Ershler, W.B.; Harris, T.; Fried, L.P. Research Agenda for Frailty in Older Adults: Toward a Better Understanding of Physiology and Etiology: Summary from the American Geriatrics Society/National Institute on Aging Research Conference on Frailty in Older Adults. J. Am. Geriatr. Soc. 2006, 54, 991–1001. [Google Scholar] [CrossRef] [PubMed]
- Buta, B.J.; Walston, J.D.; Godino, J.G.; Park, M.; Kalyani, R.R.; Xue, Q.-L.; Bandeen-Roche, K.; Varadhan, R. Frailty assessment instruments: Systematic characterization of the uses and contexts of highly-cited instruments. Ageing Res. Rev. 2016, 26, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M157. [Google Scholar] [CrossRef] [PubMed]
- Tsutsumimoto, K.; Doi, T.; Makizako, H.; Hotta, R.; Nakakubo, S.; Makino, K.; Suzuki, T.; Shimada, H. Aging-related anorexia and its association with disability and frailty. J. Cachexia Sarcopenia Muscle 2018, 9, 834–843. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [Green Version]
- Fearon, K.; Strasser, F.; Anker, S.D.; Bosaeus, I.; Bruera, E.; Fainsinger, R.L.; Jatoi, A.; Loprinzi, C.; MacDonald, N.; Mantovani, G.; et al. Definition and classification of cancer cachexia: An international consensus. Lancet Oncol. 2011, 12, 489–495. [Google Scholar] [CrossRef]
- Ethun, C.G.; Bilen, M.A.; Jani, A.B.; Maithel, S.K.; Ogan, K.; Master, V.A. Frailty and cancer: Implications for oncology surgery, medical oncology, and radiation oncology. CA. Cancer J. Clin. 2017, 67, 362–377. [Google Scholar] [CrossRef] [Green Version]
- Pamoukdjian, F.; Aparicio, T.; Zebachi, S.; Zelek, L.; Paillaud, E.; Canoui-Poitrine, F. Comparison of Mobility Indices for Predicting Early Death in Older Patients With Cancer: The Physical Frailty in Elderly Cancer Cohort Study. J. Gerontol. A Biol. Sci. Med. Sci. 2020, 75, 189–196. [Google Scholar] [CrossRef]
- Miller, M.D.; Paradis, C.F.; Houck, P.R.; Mazumdar, S.; Stack, J.A.; Rifai, A.H.; Mulsant, B.; Reynolds, C.F. Rating chronic medical illness burden in geropsychiatric practice and research: Application of the Cumulative Illness Rating Scale. Psychiatry Res. 1992, 41, 237–248. [Google Scholar] [CrossRef]
- Katz, S.; Downs, T.D.; Cash, H.R.; Grotz, R.C. Progress in development of the index of ADL. Gerontologist 1970, 10, 20–30. [Google Scholar] [CrossRef]
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Raynaud-Simon, A.; Revel-Delhom, C.; Hébuterne, X. French Nutrition and Health Program, French Health High Authority Clinical practice guidelines from the French Health High Authority: Nutritional support strategy in protein-energy malnutrition in the elderly. Clin. Nutr. Edinb. Scotl. 2011, 30, 312–319. [Google Scholar] [CrossRef] [PubMed]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A Short Physical Performance Battery Assessing Lower Extremity Function: Association With Self-Reported Disability and Prediction of Mortality and Nursing Home Admission. J. Gerontol. 1994, 49, M85–M94. [Google Scholar] [CrossRef] [PubMed]
- Vellas, B.J.; Wayne, S.J.; Romero, L.; Baumgartner, R.N.; Rubenstein, L.Z.; Garry, P.J. One-leg balance is an important predictor of injurious falls in older persons. J. Am. Geriatr. Soc. 1997, 45, 735–738. [Google Scholar] [CrossRef] [PubMed]
- Clément, J.P.; Nassif, R.F.; Léger, J.M.; Marchan, F. Development and contribution to the validation of a brief French version of the Yesavage Geriatric Depression Scale. L’Encéphale 1997, 23, 91–99. [Google Scholar] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Lahousse, L.; Maes, B.; Ziere, G.; Loth, D.W.; Verlinden, V.J.A.; Zillikens, M.C.; Uitterlinden, A.G.; Rivadeneira, F.; Tiemeier, H.; Franco, O.H.; et al. Adverse outcomes of frailty in the elderly: The Rotterdam Study. Eur. J. Epidemiol. 2014, 29, 419–427. [Google Scholar] [CrossRef]
- Avila-Funes, J.A.; Helmer, C.; Amieva, H.; Barberger-Gateau, P.; Goff, M.L.; Ritchie, K.; Portet, F.; Carrière, I.; Tavernier, B.; Gutiérrez-Robledo, L.M.; et al. Frailty among community-dwelling elderly people in france: The three-city study. J. Gerontol. A Biol. Sci. Med. Sci. 2008, 63, 1089. [Google Scholar] [CrossRef]
- Shine, B.; de Beer, F.C.; Pepys, M.B. Solid phase radioimmunoassays for human C-reactive protein. Clin. Chim. Acta Int. J. Clin. Chem. 1981, 117, 13–23. [Google Scholar] [CrossRef]
- Schreiber, J.B. Core reporting practices in structural equation modeling. Res. Soc. Adm. Pharm. 2008, 4, 83–97. [Google Scholar] [CrossRef]
- Ryan, A.M.; Power, D.G.; Daly, L.; Cushen, S.J.; Bhuachalla, Ē.N.; Prado, C.M. Cancer-associated malnutrition, cachexia and sarcopenia: The skeleton in the hospital closet 40 years later. Proc. Nutr. Soc. 2016, 75, 199–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pamoukdjian, F.; Bouillet, T.; Lévy, V.; Soussan, M.; Zelek, L.; Paillaud, E. Prevalence and predictive value of pre-therapeutic sarcopenia in cancer patients: A systematic review. Clin. Nutr. 2018, 37, 1101–1113. [Google Scholar] [CrossRef] [PubMed]
- Sur, M.D.; Namm, J.P.; Hemmerich, J.A.; Buschmann, M.M.; Roggin, K.K.; Dale, W. Radiographic Sarcopenia and Self-reported Exhaustion Independently Predict NSQIP Serious Complications After Pancreaticoduodenectomy in Older Adults. Ann. Surg. Oncol. 2015, 22, 3897–3904. [Google Scholar] [CrossRef] [PubMed]
- Gill, T.M.; Gahbauer, E.A.; Allore, H.G.; Han, L. Transitions between frailty states among community-living older persons. Arch. Intern. Med. 2006, 166, 418–423. [Google Scholar] [CrossRef]
- Marzetti, E.; Calvani, R.; Tosato, M.; Cesari, M.; Di Bari, M.; Cherubini, A.; Broccatelli, M.; Savera, G.; D’Elia, M.; Pahor, M.; et al. Physical activity and exercise as countermeasures to physical frailty and sarcopenia. Aging Clin. Exp. Res. 2017, 29, 35–42. [Google Scholar] [CrossRef]
- Minnella, E.M.; Awasthi, R.; Loiselle, S.-E.; Agnihotram, R.V.; Ferri, L.E.; Carli, F. Effect of Exercise and Nutrition Prehabilitation on Functional Capacity in Esophagogastric Cancer Surgery: A Randomized Clinical Trial. JAMA Surg. 2018, 153, 1081–1089. [Google Scholar] [CrossRef] [Green Version]
- Davis, M.P.; Panikkar, R. Sarcopenia associated with chemotherapy and targeted agents for cancer therapy. Ann. Palliat. Med. 2018, 8, 86–101. [Google Scholar] [CrossRef]
- Deimling, G.T.; Arendt, J.A.; Kypriotakis, G.; Bowman, K.F. Functioning of Older, Long-Term Cancer Survivors: The Role of Cancer and Comorbidities. J. Am. Geriatr. Soc. 2009, 57, S289–S292. [Google Scholar] [CrossRef]
- Van der Leeden, M.; Huijsmans, R.J.; Geleijn, E.; de Rooij, M.; Konings, I.R.; Buffart, L.M.; Dekker, J.; Stuiver, M.M. Tailoring exercise interventions to comorbidities and treatment-induced adverse effects in patients with early stage breast cancer undergoing chemotherapy: A framework to support clinical decisions. Disabil. Rehabil. 2018, 40, 486–496. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | n (%) or Median [IQR] |
|---|---|
| Age (year) | 82 [77–86] |
| Sex (female) | 323 (54) |
| Frailty phenotype (yes) | 352 (58) |
| Cancer site | |
| Colorectal | 109 (18) |
| Breast | 105 (17) |
| Lung | 92 (15) |
| Liver | 85 (14) |
| Digestive tract other than colorectal a | 79 (13) |
| Genito-urinary tract | 40 (7) |
| Haematological malignancies | 34 (6) |
| Skin with melanoma | 16 (2.5) |
| Prostatic | 16 (2.5) |
| Others b | 27 (5) |
| Cancer extension | |
| Local | 104 (17) |
| Locally advanced | 228 (38) |
| Metastatic | 271 (45) |
| Supportive care only (yes) | 124 (20.5) |
| Comorbidities (CIRS(G)): | |
| Total >14 | 269 (45) |
| Dependence | |
| ADL £ 5/6 | 204 (34) |
| IADL £ 3/4 | 386 (64) |
| Nutrition | |
| BMI < 21 kg/m2 | 84 (14) |
| Serum albumin level < 35 g/L | 221 (37) |
| Serum CRP ≥ 10 mg/L | 267 (44) |
| Mobility | |
| SPPB < 9/12 | 314 (52) |
| One-leg stance balance < 5 s | 448 (74) |
| Mood | |
| Mini-GDS ≥ 1/4 | 261 (44) |
| Missing data | 6 (1) |
| Cognition | |
| MMSE < 24/30 | 217 (51) |
| Missing data | 174 (29) |
| Shrinking (Yes) | Exhaustion (Yes) | Low Physical Activity (Yes) | Slowness (Yes) | Weakness (Yes) | One-Leg Stance < 5 s (Yes) | SPPB < 9/12 (Yes) | BMI < 21 kg/m2 (Yes) | Albumin < 35 g/L (Yes) | CRP ≥ 10 mg/L (Yes) | Age ≥ 82 Years (Yes) | CIRS(G) Total > 14 (Yes) | Cancer Site | Cancer Extension | Supportive Care Only (Yes) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Shrinking (yes) | 1 | ||||||||||||||
| Exhaustion (yes) | 0.24 * | 1 | |||||||||||||
| Low physical Activity (yes) | 0.13 * | 0.13 * | 1 | ||||||||||||
| Slowness (yes) | 0.10 * | 0.31 * | 0.27 * | 1 | |||||||||||
| Weakness (yes) | 0.06 | 0.18 * | 0.23 * | 0.34 * | 1 | ||||||||||
| One-leg stance < 5 s (yes) | 0.06 | 0.15 * | 0.33 * | 0.37 * | 0.35 * | 1 | |||||||||
| SPPB < 9/12 (yes) | 0.09 * | 0.29 * | 0.29 * | 0.75 * | 0.38 * | 0.50 * | 1 | ||||||||
| BMI < 21 kg/m2 (yes) | 0.18 * | 0.18 * | 0.04 | 0.05 | 0.03 | 0.06 | 0.03 | 1 | |||||||
| Serum albumin < 35 g/L (yes) | 0.22 * | 0.20 * | 0.10 * | 0.21 * | 0.14 * | 0.13 * | 0.20 * | 0.17 * | 1 | ||||||
| Serum CRP ≥ 10 mg/L (yes) | 0.20 * | 0.12 * | 0.08 * | 0.05 | 0.05 | 0.06 | 0.06 | 0.09 * | 0.30 * | 1 | |||||
| Age ≥ 82 years (yes) | 0.06 | 0.05 | 0.08 * | 0.16 * | 0.15 * | 0.20 * | 0.24 * | 0.09 * | 0.04 | 0.003 | 1 | ||||
| CIRS(G) total > 14 (yes) | 0.01 | 0.05 | 0.11 * | 0.25 * | 0.15 * | 0.19 * | 0.25 * | 0.11 * | 0.11 * | 0.10 * | 0.14 * | 1 | |||
| Cancer site | 0.30 * | 0.12 | 0.15 | 0.21 * | 0.14 | 0.14 | 0.20 * | 0.15 | 0.20 * | 0.25 * | 0.19 * | 0.12 | 1 | ||
| Cancer extension | 0.08 | 0.05 | 0.02 | 0.02 | 0.02 | 0.04 | 0.02 | 0.02 | 0.04 | 0.15 * | 0.09 | 0.02 | 0.24 * | 1 | |
| Supportive care only (yes) | 0.03 | 0.15 * | 0.08 * | 0.25 * | 0.17 * | 0.14 * | 0.23 * | 0.09 * | 0.13 * | 0.05 | 0.14 * | 0.09 * | 0.23 * | 0.08 | 1 |
| Models | Estimate | Standard Error | Standardized Coefficient (β Coefficient) | p Value |
|---|---|---|---|---|
| Model 1 | ||||
| Sarcopenia~CIRS(G) total > 14 | 0.64 | 0.1 | 0.30 | <0.0001 |
| Exhaustion~sarcopenia | 0.47 | 0.06 | 0.47 | <0.0001 |
| Cachexia~exhaustion | 0.16 | 0.05 | 0.37 | 0.001 |
| Mortality * | ||||
| ~ sarcopenia | 0.18 | 0.07 | 0.18 | 0.01 |
| ~ cachexia | 1.30 | 0.29 | 0.52 | <0.0001 |
| ~ cancer site | 0.05 | 0.02 | 0.13 | 0.03 |
| ~ cancer extension | 0.23 | 0.07 | 0.20 | <0.0001 |
| Supportive care only ~ sarcopenia | 0.44 | 0.06 | 0.45 | <0.0001 |
| Model 2 | ||||
| Sarcopenia ~ CIRS(G) total > 14 | 0.64 | 0.1 | 0.30 | <0.0001 |
| Exhaustion ~ sarcopenia | 0.47 | 0.06 | 0.48 | <0.0001 |
| Cachexia ~ exhaustion | 0.17 | 0.05 | 0.41 | <0.0001 |
| Morbidity * | ||||
| ~ sarcopenia | 0.36 | 0.06 | 0.37 | <0.0001 |
| ~ cachexia | 0.46 | 0.20 | 0.19 | 0.02 |
| ~ cancer site | 0.05 | 0.02 | 0.14 | 0.01 |
| ~ cancer extension | 0.06 | 0.06 | 0.06 | 0.28 |
| Supportive care only ~ sarcopenia | 0.44 | 0.06 | 0.45 | <0.0001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pamoukdjian, F.; Laurent, M.; Martinez-Tapia, C.; Rolland, Y.; Paillaud, E.; Canoui-Poitrine, F. Frailty Parameters, Morbidity and Mortality in Older Adults with Cancer: A Structural Equation Modelling Approach Based on the Fried Phenotype. J. Clin. Med. 2020, 9, 1826. https://doi.org/10.3390/jcm9061826
Pamoukdjian F, Laurent M, Martinez-Tapia C, Rolland Y, Paillaud E, Canoui-Poitrine F. Frailty Parameters, Morbidity and Mortality in Older Adults with Cancer: A Structural Equation Modelling Approach Based on the Fried Phenotype. Journal of Clinical Medicine. 2020; 9(6):1826. https://doi.org/10.3390/jcm9061826
Chicago/Turabian StylePamoukdjian, Frederic, Marie Laurent, Claudia Martinez-Tapia, Yves Rolland, Elena Paillaud, and Florence Canoui-Poitrine. 2020. "Frailty Parameters, Morbidity and Mortality in Older Adults with Cancer: A Structural Equation Modelling Approach Based on the Fried Phenotype" Journal of Clinical Medicine 9, no. 6: 1826. https://doi.org/10.3390/jcm9061826