Clinical Outcomes of Root-Analogue Implants Restored with Single Crowns or Fixed Dental Prostheses: A Retrospective Case Series

 ,
,  , and
, and 
Abstract
:1. Introduction
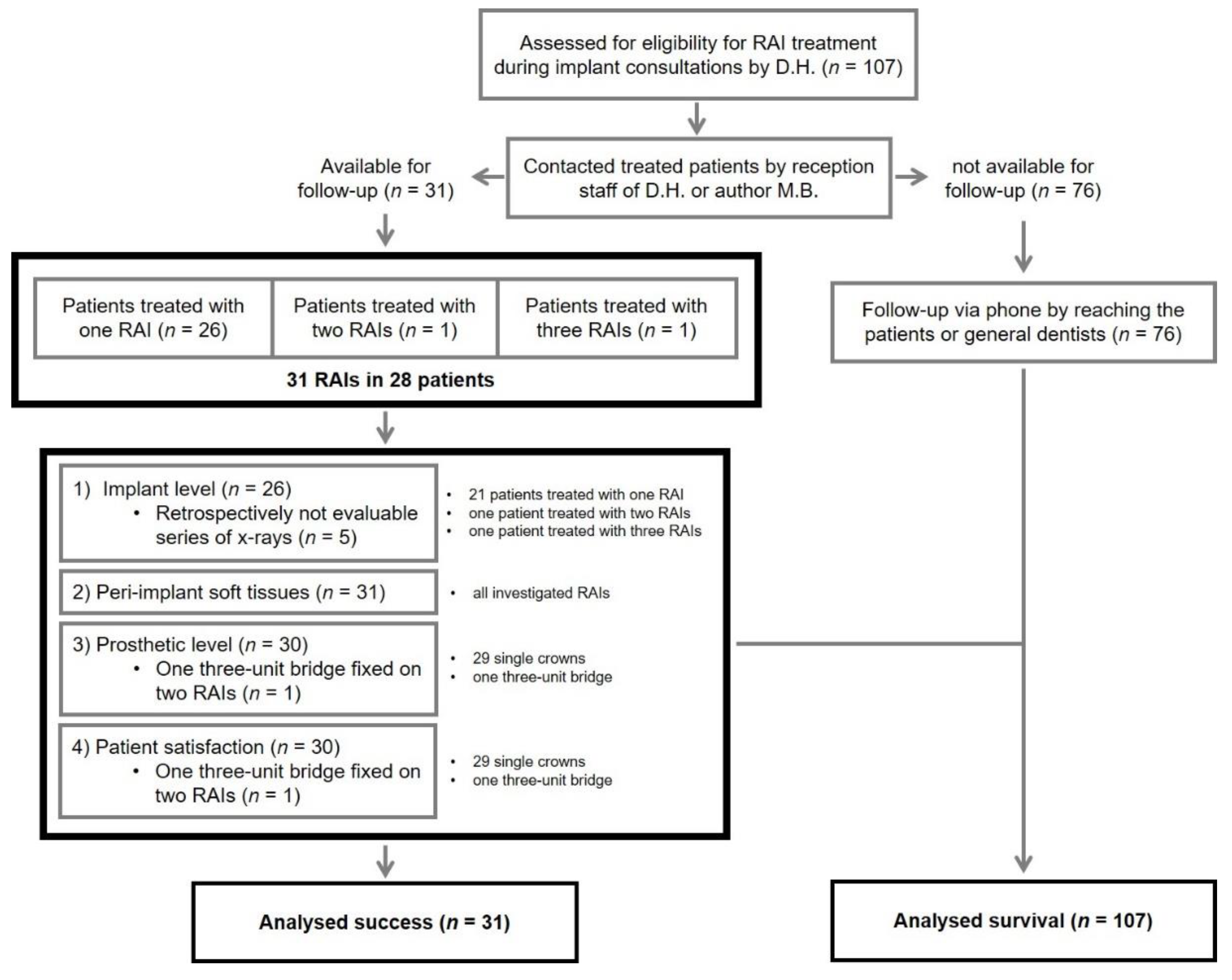
2. Experimental Section
3. Results
3.1. Demographic Data and Additional Information
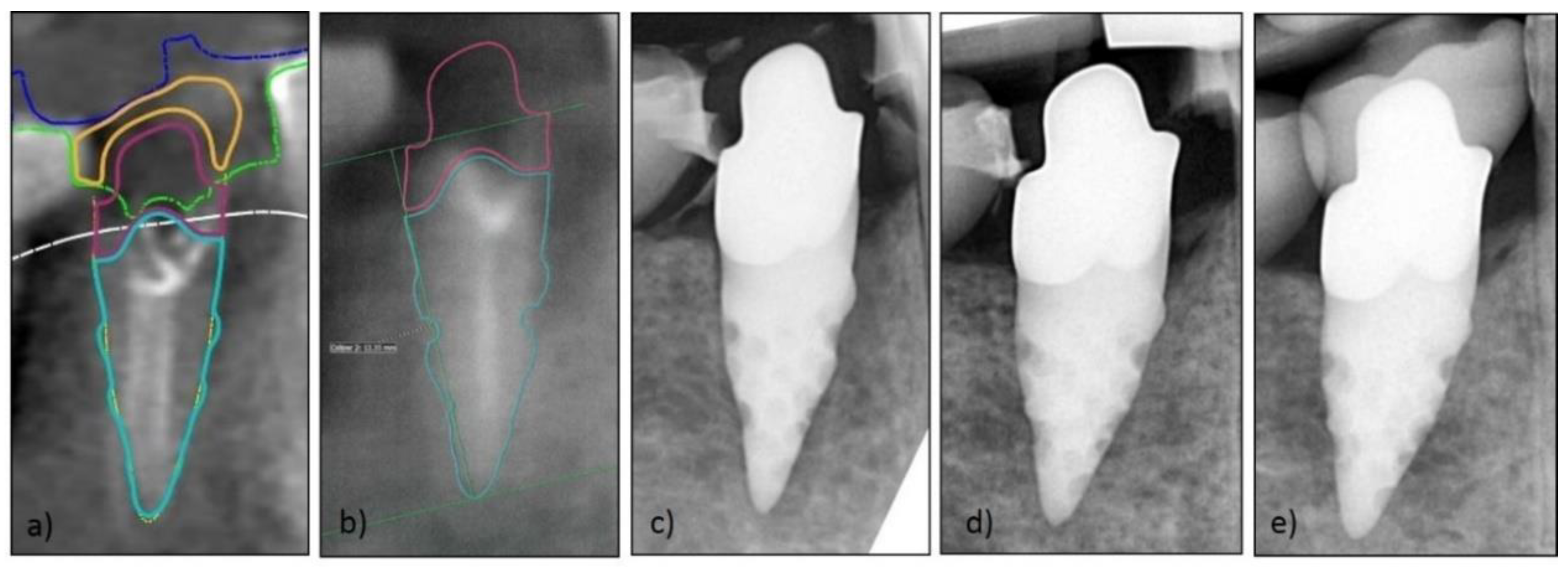
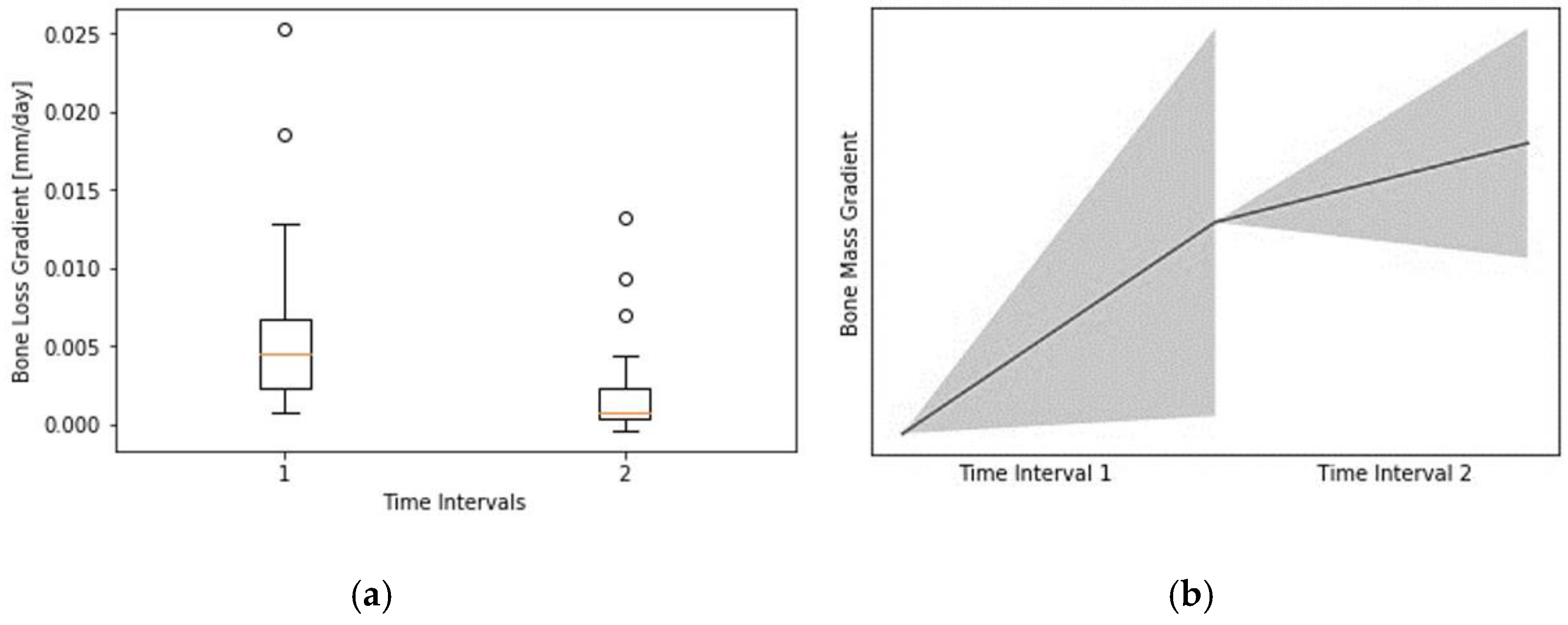
3.2. Implant Level
3.3. Peri-Implant Soft Tissues
3.4. Prosthetic Level
3.5. Patient Satisfaction
3.6. Overall Survival and Success
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Moraschini, V.; Poubel, L.D.C.; Ferreira, V.F.; Barboza, E.D.S. Evaluation of survival and success rates of dental implants reported in longitudinal studies with a follow-up period of at least 10 years: A systematic review. Int. J. Oral Maxillofac. Surg. 2015, 44, 377–388. [Google Scholar] [CrossRef]
- Tan, W.L.; Wong, T.L.T.; Wong, M.C.M.; Lang, N.P. A systematic review of post-extractional alveolar hard and soft tissue dimensional changes in humans. Clin. Oral Implant. Res. 2011, 23, 1–21. [Google Scholar] [CrossRef]
- Bhola, M.; Neely, A.L.; Kolhatkar, S. Immediate Implant Placement: Clinical Decisions, Advantages, and Disadvantages. J. Prosthodont. 2008, 17, 576–581. [Google Scholar] [CrossRef]
- Esposito, M.; Grusovin, M.G.; Polyzos, I.P.; Felice, P.; Worthington, H.V. Timing of implant placement after tooth extraction: Immediate, immediate-delayed or delayed implants? A Cochrane systematic review. Eur. J. oral Implant. 2010, 3, 189–205. [Google Scholar]
- Clementini, M.; Tiravia, L.; De Risi, V.; Orgeas, G.V.; Mannocci, A.; De Sanctis, M. Dimensional changes after immediate implant placement with or without simultaneous regenerative procedures. J. Clin. Periodontol. 2015, 42, 666–677. [Google Scholar] [CrossRef]
- Arora, H.; Khzam, N.; Roberts, D.; Bruce, W.L.; Ivanovski, S. Immediate implant placement and restoration in the anterior maxilla: Tissue dimensional changes after 2-5 year follow up. Clin. Implant. Dent. Relat. Res. 2017, 19, 694–702. [Google Scholar] [CrossRef]
- Pietrokovski, J.; Massler, M. Alveolar ridge resorption following tooth extraction. J. Prosthet. Dent. 1967, 17, 21–27. [Google Scholar] [CrossRef]
- Hodosh, M.; Povar, M.; Shklar, G. The dental polymer implant concept. J. Prosthet. Dent. 1969, 22, 371–380. [Google Scholar] [CrossRef]
- Lundgren, D.; Rylander, H.; Anderssong, M.; Johansson, C.; Albrektsson, T. Healing-in of root analogue titanium implants placed in extraction sockets. An experimental study in the beagle dog. Clin. Oral Implant. Res. 1992, 3, 136–144. [Google Scholar] [CrossRef]
- Kohal, R.; Hürzeler, M.B.; Mota, L.F.; Klaus, G.; Caffesse, R.G.; Strub, J.R. Custom-made root analogue titanium implants placed into extraction sockets. An experimental study in monkeys. Clin. Oral Implant. Res. 1997, 8, 386–392. [Google Scholar] [CrossRef]
- Kohal, R.; Klaus, G.; Gieloff, B.; Hürzeler, M.B.; Strub, J.R. Wurzelanaloge Titanimplantate (Bio-Design-Implantate) für die Sofortimplantation-Das Re-Implant-System. Implantologie 1996, 4, 99–115. [Google Scholar]
- Strub, J.R.; Klaus, G.; Ferraresso, F.; Kohal, R. The Re Implant® System for Immediate Implant Placement. J. Esthet. Restor. Dent. 1997, 9, 187–196. [Google Scholar] [CrossRef] [PubMed]
- Kohal, R.; Klaus, G.; Strub, J.R. Klinische Untersuchung eines neuen dentalen Sofort-Implantatsystems. Das ReImplant-System. Dtsch. Zahnärztliche Z. 2002, 57, 495–497. [Google Scholar]
- Pirker, W.; Kocher, A. Immediate, non-submerged, root-analogue zirconia implant in single tooth replacement. Int. J. Oral Maxillofac. Surg. 2008, 37, 293–295. [Google Scholar] [CrossRef]
- Pirker, W.; Kocher, A. Immediate, non-submerged, root-analogue zirconia implants placed into single-rooted extraction sockets: 2-year follow-up of a clinical study. Int. J. Oral Maxillofac. Surg. 2009, 38, 1127–1132. [Google Scholar] [CrossRef]
- Pirker, W.; Kocher, A. Root analog zirconia implants: True anatomical design for molar replacement—A case report. Int. J. Periodontics Restor. Dent. 2011, 31, 663–668. [Google Scholar]
- Pirker, W.; Wiedemann, D.; Lidauer, A.; Kocher, A. Immediate, single stage, truly anatomic zirconia implant in lower molar replacement: A case report with 2.5 years follow-up. Int. J. Oral Maxillofac. Surg. 2011, 40, 212–216. [Google Scholar] [CrossRef]
- Moin, D.A.; Hassan, B.; Mercelis, P.; Wismeijer, D. Designing a novel dental root analogue implant using cone beam computed tomography and CAD/CAM technology. Clin. Oral Implant. Res. 2011, 24, 25–27. [Google Scholar] [CrossRef]
- Mangano, C.; Cirotti, B.; Sammons, R.L.; Mangano, C. Custom-made, root-analogue direct laser metal forming implant: A case report. Lasers Med Sci. 2012, 27, 1241–1245. [Google Scholar] [CrossRef]
- Pour, R.; Randelzhofer, P.; Edelhoff, D.; Prandtner, O.; Rafael, C.; Liebermann, A. Innovative Single-Tooth Replacement with an Individual Root-Analog Hybrid Implant in the Esthetic Zone: Case Report. Int. J. Oral Maxillofac. Implant. 2017, 32. [Google Scholar] [CrossRef]
- Beuer, F.; Groesser, J.; Schweiger, J.; Hey, J.; Güth, J.-F.; Stimmelmayr, M. The Digital One-Abutment/One-Time Concept. A Clinical Report. J. Prosthodont. 2015, 24, 580–585. [Google Scholar] [CrossRef] [PubMed]
- Schubert, O.; Beuer, F.; Güth, J.-F.; Nold, E.; Edelhoff, D.; Metz, I. Two digital strategies in modern implantology—Root-analogue implants and the digital one-abutment/one-time concept. Int. J. Comput. Dent. 2018, 21, 115–131. [Google Scholar] [PubMed]
- Sanz, M.; Noguerol, B.; Sanz-Sánchez, I.; Hammerle, C.H.F.; Schliephake, H.; Renouard, F.; Sicilia, A.; Steering Committee; Cordaro, L.; Jung, R. European Association for Osseointegration Delphi study on the trends in Implant Dentistry in Europe for the year 2030. Clin. Oral Implant. Res. 2019, 30, 476–486. [Google Scholar] [CrossRef]
- Muska, E.; Walter, C.; Knight, A.; Taneja, P.; Bulsara, Y.; Hahn, M.; Desai, M.; Dietrich, T. Atraumatic vertical tooth extraction: A proof of principle clinical study of a novel system. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 116, e303–e310. [Google Scholar] [CrossRef] [PubMed]
- Okada, H.; Takahashi, K.; Ogura, N.; Tomoki, R.; Ito, K.; Kondoh, T. Plasma rich in growth factors stimulates proliferation, migration, and gene expression associated with bone formation in human dental follicle cells. J. Dent. Sci. 2016, 11, 245–252. [Google Scholar] [CrossRef] [Green Version]
- Papaspyridakos, P.; Chen, C.-J.; Singh, M.; Weber, H.-P.; O Gallucci, G. Success criteria in implant dentistry: A systematic review. J. Dent. Res. 2011, 91, 242–248. [Google Scholar] [CrossRef]
- Albrektsson, T.; Zarb, G.; Worthington, P.; Eriksson, A.R. The long-term efficacy of currently used dental implants: A review and proposed criteria of success. Int. J. Oral Maxillofac. Implant. 1986, 1, 11–25. [Google Scholar]
- Bra-Nemark, P.-I.; Zarb, G.A.; Albrektsson, T.; Rosen, H.M. Tissue-Integrated Prostheses. Osseointegration in Clinical Dentistry. Plast. Reconstr. Surg. 1986, 77, 496–497. [Google Scholar] [CrossRef]
- Mombelli, A.; Oosten, M.A.C.; Schürch, E.; Land, N.P.; Lang, N.P. The microbiota associated with successful or failing osseointegrated titanium implants. Oral Microbiol. Immunol. 1987, 2, 145–151. [Google Scholar] [CrossRef]
- Belser, U.C.; Grütter, L.; Vailati, F.; Bornstein, M.M.; Weber, H.-P.; Buser, D. Outcome Evaluation of Early Placed Maxillary Anterior Single-Tooth Implants Using Objective Esthetic Criteria: A Cross-Sectional, Retrospective Study in 45 Patients With a 2- to 4-Year Follow-Up Using Pink and White Esthetic Scores. J. Periodontol. 2009, 80, 140–151. [Google Scholar] [CrossRef]
- Schmalz, G.; Ryge, G. Reprint of Criteria for the clinical evaluation of dental restorative materials. Clin. Oral Investig. 2005, 9, 215–232. [Google Scholar] [CrossRef] [PubMed]
- Spies, B.C.; Kohal, R.; Balmer, M.; Vach, K.; Jung, R.E. Evaluation of zirconia-based posterior single crowns supported by zirconia implants: Preliminary results of a prospective multicenter study. Clin. Oral Implant. Res. 2016, 28, 613–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pessanha-Andrade, M.; Sordi, M.B.; Henriques, B.; Silva, F.; Teughels, W.; Souza, J.C. Custom-made root-analogue zirconia implants: A scoping review on mechanical and biological benefits. J. Biomed. Mater. Res. Part B Appl. Biomater. 2018, 106, 2888–2900. [Google Scholar] [CrossRef] [PubMed]
- Pour, R.S.; Rafael, C.F.; Engler, M.L.P.D.; Edelhoff, D.; Klaus, G.; Prandtner, O.; Berthold, M.; Liebermann, A. Historical development of root analogue implants: A review of published papers. Br. J. Oral Maxillofac. Surg. 2019, 57, 496–504. [Google Scholar] [CrossRef] [PubMed]
- Galindo-Moreno, P.; León-Cano, A.; Ortega-Oller, I.; Monje, A.; O′valle, F.; Catena, A. Marginal bone loss as success criterion in implant dentistry: Beyond 2 mm. Clin. Oral Implant. Res. 2014, 26, e28–e34. [Google Scholar] [CrossRef]
- Degidi, M.; Daprile, G.; Piattelli, A. Marginal bone loss around implants with platform-switched Morse-cone connection: A radiographic cross-sectional study. Clin. Oral Implant. Res. 2016, 28, 1108–1112. [Google Scholar] [CrossRef]
- A Malloy, K.; Wadhwani, C.; McAllister, B.; Wang, M.; A Katancik, J. Accuracy and Reproducibility of Radiographic Images for Assessing Crestal Bone Height of Implants Using the Precision Implant X-ray Locator (PIXRL) Device. Int. J. Oral Maxillofac. Implant. 2017, 32, 830–836. [Google Scholar] [CrossRef] [Green Version]
- Walton, T.R.; Layton, D. Intra- and inter-examiner agreement when assessing radiographic implant bone levels: Differences related to brightness, accuracy, participant demographics and implant characteristics. Clin. Oral Implant. Res. 2018, 29, 756–771. [Google Scholar] [CrossRef]
- Hartman, G.A.; Cochran, D.L. Initial Implant Position Determines the Magnitude of Crestal Bone Remodeling. J. Periodontol. 2004, 75, 572–577. [Google Scholar] [CrossRef]
- Hermann, J.S.; Cochran, D.L.; Nummikoski, P.V.; Buser, D. Crestal Bone Changes Around Titanium Implants. A Radiographic Evaluation of Unloaded Nonsubmerged and Submerged Implants in the Canine Mandible. J. Periodontol. 1997, 68, 1117–1130. [Google Scholar] [CrossRef]
- Capelli, M.; Testori, T.; Galli, F.; Zuffetti, F.; Motroni, A.; Weinstein, R.; Del Fabbro, M. Implant–Buccal Plate Distance as Diagnostic Parameter: A Prospective Cohort Study on Implant Placement in Fresh Extraction Sockets. J. Periodontol. 2013, 84, 1768–1774. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Misch, C.E.; Perel, M.L.; Wang, H.-L.; Sammartino, G.; Galindo-Moreno, P.; Trisi, P.; Steigmann, M.; Rebaudi, A.; Palti, A.; Pikos, M.A.; et al. Implant Success, Survival, and Failure: The International Congress of Oral Implantologists (ICOI) Pisa Consensus Conference. Implant. Dent. 2008, 17, 5–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pjetursson, B.E.; Zarauz, C.; Strasding, M.; Sailer, I.; Zwahlen, M.; Zembic, A. A systematic review of the influence of the implant-abutment connection on the clinical outcomes of ceramic and metal implant abutments supporting fixed implant reconstructions. Clin. Oral Implant. Res. 2018, 29, 160–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heitz-Mayfield, L.J.A.; Aaboe, M.; Araujo, M.; Carrión, J.B.; Cavalcanti, R.; Cionca, N.; Cochran, D.; Darby, I.; Funakoshi, E.; Gierthmuehlen, P.C.; et al. Group 4 ITI Consensus Report: Risks and biologic complications associated with implant dentistry. Clin. Oral Implant. Res. 2018, 29, 351–358. [Google Scholar] [CrossRef] [Green Version]
- Linkevicius, T.; Vindasiute, E.; Puisys, A.; Linkeviciene, L.; Maslova, N.; Puriene, A. The influence of the cementation margin position on the amount of undetected cement. A prospective clinical study. Clin. Oral Implant. Res. 2012, 24, 71–76. [Google Scholar] [CrossRef]
- Hashim, D.; Cionca, N.; Combescure, C.; Mombelli, A. The diagnosis of peri-implantitis: A systematic review on the predictive value of bleeding on probing. Clin. Oral Implant. Res. 2018, 29, 276–293. [Google Scholar] [CrossRef] [Green Version]
- Arunyanak, S.P.; Pollini, A.; Ntounis, A.; Morton, D. Clinician assessments and patient perspectives of single-tooth implant restorations in the esthetic zone of the maxilla: A systematic review. J. Prosthet. Dent. 2017, 118, 10–17. [Google Scholar] [CrossRef]
- Tettamanti, S.; Millen, C.; Gavric, J.; Buser, D.; Belser, U.C.; Bragger, U.; Wittneben, J.-G. Esthetic Evaluation of Implant Crowns and Peri-Implant Soft Tissue in the Anterior Maxilla: Comparison and Reproducibility of Three Different Indices. Clin. Implant. Dent. Relat. Res. 2015, 18, 517–526. [Google Scholar] [CrossRef] [Green Version]
- Gallucci, G.O.; Grütter, L.; Nedir, R.; Bischof, M.; Belser, U.C. Esthetic outcomes with porcelain-fused-to-ceramic and all-ceramic single-implant crowns: A randomized clinical trial. Clin. Oral Implant. Res. 2010, 22, 62–69. [Google Scholar] [CrossRef]
- Gallucci, G.O.; Doughtie, C.B.; Hwang, J.W.; Fiorellini, J.P.; Weber, H.-P. Five-year results of fixed implant-supported rehabilitations with distal cantilevers for the edentulous mandible. Clin. Oral Implant. Res. 2009, 20. [Google Scholar] [CrossRef]
- Romeo, E.; Lops, D.; Margutti, E.; Ghisolfi, M.; Chiapasco, M.; Vogel, G. Long-term survival and success of oral implants in the treatment of full and partial arches: A 7-year prospective study with the ITI dental implant system. Int. J. Oral Maxillofac. Implant. 2004, 19, 247–259. [Google Scholar]
- Romeo, E.; Tomasi, C.; Finini, I.; Casentini, P.; Lops, D. Implant-supported fixed cantilever prosthesis in partially edentulous jaws: A cohort prospective study. Clin. Oral Implant. Res. 2009, 20, 1278–1285. [Google Scholar] [CrossRef] [PubMed]
- Esposito, M.; Grusovin, M.G.; Polyzos, I.P.; Felice, P.; Worthington, H.V. Interventions for replacing missing teeth: Dental implants in fresh extraction sockets (immediate, immediate-delayed and delayed implants). Cochrane Database Syst. Rev. 2010, 9, CD005968. [Google Scholar] [CrossRef] [PubMed]
- Esposito, M.; Zucchelli, G.; Cannizzaro, G.; Checchi, L.; Barausse, C.; Trullenque-Eriksson, A.; Felice, P. Immediate, immediate-delayed (6 weeks) and delayed (4 months) post-extractive single implants: 1-year post-loading data from a randomised controlled trial. Eur. J. Oral Implant. 2017, 10, 11–26. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Alpha (A) | Bravo (B) | Charlie (C) | Delta (D) | |
|---|---|---|---|---|
| Fracture of veneering ceramic | No fracture | Minor chipping (polishable) | Major chipping (up to framework) | Fracture (loss of reconstruction) |
| Fracture of framework | No fracture | - | - | Fracture (loss of reconstruction) |
| Occlusal roughness | No roughness | Slight roughness (Ø < 2 mm) | Obvious roughness (Ø > 2 mm) | Reconstruction needs to be replaced |
| Marginal integrity | No visible or soundable gap | Marginal gap slightly soundable | Explorer penetrates a significant crevice | Reconstruction needs to be replaced |
| Contour of reconstruction | Perfectly contoured | Slightly under-/overcountoured | Pronounced under-/overcontoured | Reconstruction inacceptable |
| Esthetics of reconstruction | Good esthetics | Slight mismatch in color | Severe color mismatch | Reconstruction inacceptable |
| Discoloration of reconstruction | No discolorations | discoloration |
| Posterior (P) | Anterior (A) | Posterior (P) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| FDI | 17 | 16 | 15 | 14 | 13 | 12 | 11 | 21 | 22 | 23 | 24 | 25 | 26 | 27 |
| n (maxilla) | 1 | 1 | 3 | 0 | 0 | 1 | 6 | 5 | 0 | 1 | 3 | 1 | 0 | 0 |
| n (mandible) | 0 | 2 | 2 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 3 | 0 | 0 |
| FDI | 47 | 46 | 45 | 44 | 43 | 42 | 41 | 31 | 32 | 33 | 34 | 35 | 36 | 37 |
| n (region) | 10 | 13 | 8 | |||||||||||
| Parameter | Frequency n (%) | p-Value |
|---|---|---|
| Gender | 0.260 | |
| female | 17 (61) | |
| male | 11 (39) | |
| Age | 0.869 | |
| mean (in years) | 55.3/56.6 1 | |
| range (in years) | 31–82/33–83 1 | |
| Implant region | 0.571 | |
| anterior | 13 (42) | |
| posterior | 18 (58) | |
| Implant location | 0.691 | |
| maxilla | 22 (71) | |
| mandible | 9 (29) | |
| Implant material | 0.483 | |
| hybrid | 25 (81) | |
| all-ceramics | 6 (19) | |
| Bone quality | 0.898 | |
| I | 1 (3) | |
| II | 10 (32) | |
| III | 14 (45) | |
| IV | 6 (19) | |
| Difficulty of the operation | 0.690 | |
| easy | 0 (0) | |
| intermediate | 21 (68) | |
| complicated | 10 (32) | |
| Number of roots | 0.091 | |
| single rooted | 25 (81) | |
| multi rooted | 6 (19) |
| Length of the One-Piece Implant (in mm) | Root Portion: Length (in mm) | Abutment Portion: Length (in mm) | Implant Surface (in cm2) | |
|---|---|---|---|---|
| n | 31 | 31 | 31 | 25 1 |
| Min | 12.41 | 7.49 | 3.18 | 101 |
| Max | 26.30 | 14.79 | 14.86 | 442 |
| SD | 3.12 | 1.86 | 2.41 | 83 |
| Mean | 19.19 | 10.96 | 8.43 | 213 |
| p-values | 0.709 | 0.870 | 0.717 | 0.078 |
| RAIs | Surgery (T0) (in mm) | Loading (T1) (in mm) | Examination (T2) (in mm) | T0-T1 (in Days) | T1-T2 (in Days) | T0-T2 (in Days) | JIAP (in mm) |
|---|---|---|---|---|---|---|---|
| 1 | 0.00 | −0.50 | −1.30 | 276 | 350 | 626 | −1.00 |
| 2 | 0.00 | −1.35 | −1.55 | 276 | 350 | 626 | −1.00 |
| 3 | 0.00 | −0.20 | −0.50 | 260 | 350 | 610 | −1.00 |
| 4 | 0.00 | −1.10 | −1.30 | 281 | 272 | 553 | 0.00 |
| 5 | 0.00 | −0.90 | −0.90 | 155 | 418 | 573 | −1.50 |
| 6 | 0.00 | −1.10 | −2.20 | 86 | 509 | 595 | −1.00 |
| 7 | 0.00 | −0.50 | −0.75 | 86 | 663 | 749 | −1.00 |
| 8 | 0.00 | −1.10 | −1.25 | 153 | 750 | 903 | −1.00 |
| 9 | 0.00 | −0.30 | −0.45 | 126 | 34 | 160 | −1.00 |
| 10 | 0.00 | −0.75 | −1.00 | 254 | 358 | 612 | −1.00 |
| 11 | 0.00 | −1.70 | −1.70 | 343 | 260 | 603 | 0.00 |
| 12 | 0.00 | −0.60 | −0.85 | 291 | 369 | 660 | −1.00 |
| 13 | 0.00 | −1.70 | −2.85 | 92 | 488 | 580 | −1.00 |
| 14 | 0.00 | −0.75 | −1.40 | 132 | 182 | 314 | −1.00 |
| 15 | 0.00 | −0.95 | −2.55 | 266 | 503 | 769 | −0.75 |
| 16 | 0.00 | −0.55 | −0.85 | 228 | 32 | 260 | −1.00 |
| 17 | 0.00 | −0.40 | −0.55 | 151 | 107 | 258 | −1.00 |
| 18 | 0.00 | −0.30 | −0.75 | 135 | 34 | 169 | −1.00 |
| 19 | 0.00 | −0.40 | −0.60 | 182 | 338 | 520 | −1.00 |
| 20 | 0.00 | −0.80 | −1.15 | 124 | 50 | 174 | −1.00 |
| 21 | 0.00 | −0.35 | −0.50 | 97 | 459 | 556 | −1.00 |
| 22 | 0.00 | −2.50 | −2.90 | 99 | 598 | 697 | −1.25 |
| 23 | 0.00 | −0.45 | −1.40 | 99 | 598 | 697 | −1.25 |
| 24 | 0.00 | −0.80 | −0.80 | 102 | 584 | 686 | −1.00 |
| 25 | 0.00 | −0.65 | −1.10 | 91 | 636 | 727 | 0.00 |
| 26 | 0.00 | −0.15 | −0.15 | 141 | 288 | 429 | −1.00 |
| Min | −0.15 | −0.15 | 86.00 | 32.00 | 160.00 | −1.5 | |
| Max | −2.50 | −2.90 | 343.00 | 750.00 | 903.00 | 0.00 | |
| SD | 0.54 | 0.73 | 78.91 | 208.77 | 202.03 | 0.36 | |
| Mean | −0.82 | −1.20 | 173.56 | 368.46 | 542.54 | −0.91 |
| Implant Level | Soft tissue Parameters | Prosthetic Level | Patient Satisfaction | Overall Rating | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | n | % | |
| n | 26 | 83.9 | 31 | 100.0 | 30 | 100.0 | 30 | 100.0 | 31 | 100.0 |
| Success | 21 | 80.8 | 30 | 96.8 | 25 | 83.3 | 27 | 90.0 | 20 | 64.5 |
| Esthetic (VAS) | PES | PES/WES | WES | Total Bone Loss (T0-T2) | |
|---|---|---|---|---|---|
| Esthetic (VAS) | 1.000000 | 0.335767 | 0.358691 | 0.164237 | 0.074137 |
| PES | 0.335767 | 1.000000 | 0.666582 | 0.137687 | −0.089390 |
| PES/WES | 0.358691 | 0.666582 | 1.000000 | 0.685310 | 0.012887 |
| WES | 0.164237 | 0.137687 | 0.685310 | 1.000000 | 0.096554 |
| Total bone loss (T0-T2) | 0.074137 | −0.089390 | 0.012887 | 0.096554 | 1.000000 |
| mPI | mBI | KG (in mm) | |
|---|---|---|---|
| n | 31 | 31 | 31 |
| Min | 0 | 0 | 1.5 |
| Max | 1 | 3 | 9 |
| SD | 0.5 | 0.7 | 1.7 |
| Mean | 0.6 | 0.6 | 3.9 |
| PES | WES | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| RAIs | Mesial Papilla | Distal Papilla | Curvature of Facial Mucosa | Level of Facial Mucosa | Root Convexity/Soft Tissue Color and Texture | Total PES | Tooth Form | Outline/Volume | Color (Hue/Value) | Surface Texture | Translucency/Characterization | Total WES | Total PES + WES |
| 1 | 1 | 2 | 2 | 1 | 2 | 8 | 2 | 2 | 2 | 2 | 2 | 10 | 18 |
| 2 | 1 | 2 | 2 | 1 | 2 | 8 | 2 | 2 | 2 | 2 | 2 | 10 | 18 |
| 3 | 2 | 2 | 1 | 1 | 1 | 7 | 1 | 1 | 2 | 2 | 2 | 8 | 15 |
| 4 | 2 | 2 | 2 | 2 | 2 | 10 | 2 | 2 | 2 | 1 | 2 | 9 | 19 |
| 5 | 1 | 2 | 1 | 2 | 1 | 7 | 1 | 1 | 1 | 1 | 1 | 5 | 12 |
| 6 | 2 | 2 | 2 | 1 | 1 | 8 | 1 | 1 | 1 | 1 | 1 | 5 | 13 |
| 7 | 2 | 2 | 2 | 1 | 1 | 8 | 1 | 1 | 1 | 2 | 1 | 6 | 14 |
| 8 | 0 | 0 | 2 | 2 | 1 | 5 | 1 | 1 | 2 | 2 | 1 | 7 | 12 |
| 9 | 1 | 1 | 2 | 2 | 2 | 8 | 2 | 2 | 1 | 1 | 2 | 8 | 16 |
| 10 | 2 | 1 | 2 | 2 | 2 | 9 | 2 | 2 | 1 | 1 | 1 | 7 | 16 |
| 11 | 2 | 1 | 2 | 2 | 2 | 9 | 2 | 2 | 1 | 1 | 1 | 7 | 16 |
| 12 | 2 | 2 | 1 | 1 | 1 | 7 | 1 | 1 | 2 | 1 | 1 | 6 | 13 |
| 13 | 2 | 2 | 1 | 2 | 2 | 9 | 1 | 1 | 1 | 1 | 2 | 6 | 15 |
| 14 | 1 | 2 | 1 | 1 | 1 | 6 | 1 | 1 | 2 | 2 | 2 | 8 | 14 |
| 15 | 1 | 1 | 1 | 1 | 1 | 5 | 1 | 1 | 1 | 2 | 2 | 7 | 12 |
| 16 | 1 | 0 | 2 | 1 | 2 | 6 | 2 | 2 | 2 | 2 | 2 | 10 | 16 |
| 17 | 2 | 1 | 2 | 2 | 2 | 9 | 2 | 2 | 1 | 2 | 1 | 8 | 17 |
| 18 | 0 | 2 | 2 | 1 | 2 | 7 | 2 | 1 | 1 | 1 | 2 | 7 | 14 |
| 19 | 2 | 0 | 1 | 1 | 1 | 5 | 1 | 1 | 1 | 1 | 1 | 5 | 10 |
| 20 | 1 | 1 | 2 | 2 | 2 | 8 | 2 | 2 | 2 | 2 | 2 | 10 | 18 |
| 21 | 1 | 0 | 2 | 2 | 2 | 7 | 2 | 2 | 2 | 2 | 2 | 10 | 17 |
| 22 | 1 | 1 | 1 | 1 | 2 | 6 | 2 | 2 | 2 | 2 | 2 | 10 | 16 |
| 23 | 1 | 1 | 1 | 1 | 2 | 6 | 2 | 2 | 2 | 2 | 2 | 10 | 16 |
| 24 | 1 | 1 | 2 | 2 | 1 | 7 | 1 | 1 | 2 | 2 | 2 | 8 | 15 |
| 25 | 1 | 2 | 2 | 2 | 2 | 9 | 2 | 2 | 2 | 2 | 2 | 10 | 19 |
| 26 | 0 | 0 | 1 | 1 | 2 | 4 | 2 | 2 | 1 | 2 | 2 | 9 | 13 |
| 27 | 2 | 1 | 2 | 2 | 1 | 8 | 1 | 1 | 2 | 1 | 1 | 6 | 14 |
| 28 | 2 | 2 | 2 | 2 | 1 | 9 | 2 | 2 | 2 | 2 | 2 | 10 | 19 |
| 29 | 1 | 2 | 2 | 2 | 1 | 8 | 2 | 2 | 1 | 2 | 1 | 8 | 16 |
| 30 | 2 | 2 | 1 | 2 | 2 | 9 | 1 | 1 | 1 | 2 | 1 | 6 | 15 |
| 31 | 2 | 2 | 2 | 2 | 1 | 9 | 2 | 2 | 1 | 2 | 2 | 9 | 18 |
| Min | 0 | 0 | 1 | 1 | 1 | 4 | 1 | 1 | 1 | 1 | 1 | 5 | 10 |
| Max | 2 | 2 | 2 | 2 | 2 | 10 | 2 | 2 | 2 | 2 | 2 | 10 | 19 |
| SD | 0.66 | 0.75 | 0.49 | 0.51 | 0.51 | 1.50 | 0.50 | 0.51 | 0.51 | 0.49 | 0.50 | 1.74 | 2.33 |
| Mean | 1.35 | 1.35 | 1.65 | 1.55 | 1.55 | 7.45 | 1.58 | 1.55 | 1.52 | 1.65 | 1.61 | 7.90 | 15.35 |
| Alpha (A) | Bravo (B) | Charlie (C) | Delta (D) | |
|---|---|---|---|---|
| Fracture of veneering ceramic | 29 (96.7%) | 0 | 1 (3.3%) | 0 |
| Fracture of framework | 30 (100.0%) | 0 | 0 | 0 |
| Occlusal roughness | 26 (86.7%) | 4 (13.3%) | 0 | 0 |
| Marginal integrity | 9 (30.0%) | 17 (56.7%) | 4 (13.3%) | 0 |
| Contour of reconstruction | 22 (73.3%) | 8 (26.7%) | 0 | 0 |
| Esthetics of reconstruction | 24 (80.0%) | 6 (20.0%) | 0 | 0 |
| Discoloration of reconstruction | 30 (100.0%) | 0 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Böse, M.W.H.; Hildebrand, D.; Beuer, F.; Wesemann, C.; Schwerdtner, P.; Pieralli, S.; Spies, B.C. Clinical Outcomes of Root-Analogue Implants Restored with Single Crowns or Fixed Dental Prostheses: A Retrospective Case Series. J. Clin. Med. 2020, 9, 2346. https://doi.org/10.3390/jcm9082346
Böse MWH, Hildebrand D, Beuer F, Wesemann C, Schwerdtner P, Pieralli S, Spies BC. Clinical Outcomes of Root-Analogue Implants Restored with Single Crowns or Fixed Dental Prostheses: A Retrospective Case Series. Journal of Clinical Medicine. 2020; 9(8):2346. https://doi.org/10.3390/jcm9082346
Chicago/Turabian StyleBöse, Mats Wernfried Heinrich, Detlef Hildebrand, Florian Beuer, Christian Wesemann, Paul Schwerdtner, Stefano Pieralli, and Benedikt Christopher Spies. 2020. "Clinical Outcomes of Root-Analogue Implants Restored with Single Crowns or Fixed Dental Prostheses: A Retrospective Case Series" Journal of Clinical Medicine 9, no. 8: 2346. https://doi.org/10.3390/jcm9082346