The Need for Red Cell Support During Non-Cardiac Surgery Is Associated to Pre-Transfusion Levels of FXIII and the Platelet Count


Abstract
:1. Introduction
2. Background
3. Patients and Methods
4. Results
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Okamura, R.; Hida, K.; Hasegawa, S.; Yoshiharu, S.; Hamada, M.; Yasui, M.; Takao, H.; Watanabe, M. The Japan Society of Laparoscopic Colorectal Surgery. Impact of intraoperative blood loss on morbidity and survival after radical surgery for colorectal cancer patients aged 80 years or older. Int. J. Colorectal Dis. 2016, 31, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Wedel, C.; Møller, C.M.; Budtz-Lilly, J.; Eldrup, N. Red blood cell transfusion associated with increased morbidity and mortality in patients undergoing elective open abdominal aortic aneurysm repair. PLoS ONE 2019, 14, e0219263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goodnough, L.T.; Panigrahi, A.K. Blood Transfusion Therapy. Med. Clin. 2017, 101, 431–447. [Google Scholar] [CrossRef] [PubMed]
- Carson, J.L.; Duff, A.; Poses, R.M.; Berlin, J.A.; Spence, R.K.; Trout, R.; Noveck, H.; Strom, B.L. Effect of anemia and cardiovascular disease on surgical mortality and morbidity. Lancet 1996, 348, 1055–1060. [Google Scholar] [CrossRef]
- Spandorfer, J. The management of anticoagulation before and after procedures. Med. Clin. N. Am. 2001, 85, 1109–1116. [Google Scholar] [CrossRef]
- Smilowitz, N.R.; Oberweis, B.S.; Nukala, S.; Rosenberg, A.; Zhao, S.; Xu, J.; Stuchin, S.A.; Iorio, R.; Errico, T.J.; Radford, M.J.; et al. Association between anemia, bleeding and transfusion with long-term mortality following noncardiac surgery. Am. J. Med. 2016, 129, 315–323. [Google Scholar] [CrossRef] [Green Version]
- Shander, A.; Knight, K.; Thurer, R.; Adamson, J.; Spence, R. Prevalence and outcomes of anemia in surgery: A systematic review of the literature. Am. J. Med. 2004, 116, 58S–69S. [Google Scholar] [CrossRef]
- Gomez-Ramirez, S.; Jerico, C.; Muñoz, M. Perioperative anemia: Prevalence, consequences and pathophysiology. Transfus. Apher. Sci. 2019, 58, 369–374. [Google Scholar] [CrossRef]
- Stammers, A.H.; Tesdahl, E.A.; Mongero, L.B.; Stasko, A. Gender and intraoperative blood transfusion: Analysis of 54,122 non-reoperative coronary revascularization procedures. Perfusion 2019, 34, 236–245. [Google Scholar] [CrossRef]
- Hsieh, L.; Nugent, D. Factor XIII deficiency. Haemophilia 2008, 14, 1190–1200. [Google Scholar] [CrossRef]
- Thalan, A.; Ahluwalia, J. Factor XIII. Arch. Pathol. Lab. Med. 2014, 138, 278–281. [Google Scholar] [CrossRef] [PubMed]
- Mosesson, M.W.; Siebenlist, K.R.; Hernandez, I.; Lee, K.N.; Christiansen, V.J.; Mc Kee, P.A. Evidence that alpha2 –antiplasmin becomes covalently ligated to plasma fibrinogen in the circulation: A new role for plasma factor XIII in fibrinolysis regulation. J. Thromb. Haemost. 2008, 6, 1565–1570. [Google Scholar] [CrossRef] [PubMed]
- Palla, R.; Peyvandi, F.; Shapiro, A.D. Rare bleeding disorders: Diagnosis and treatment. Blood 2015, 125, 2052–2061. [Google Scholar] [CrossRef] [PubMed]
- Mangla, A.; Hamad, H.; Kumar, A. Factor XIII Deficiency. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Souri, M.; Osaki, T.; Ichinose, A. Anti-factor XIII A subunit (FXIII-A) autoantibodies block FXIII-A2 B2 assembly and steal FXIII-A from native FXIII-A2 B2. J. Thromb. Haemost. 2015, 13, 802–814. [Google Scholar] [CrossRef]
- Von Rappard, S.; Hinnen, C.; Lussmann, R.; Rechsteiner, M. Factor XIII Deficiency and Thrombocytopenia Are Frequent Modulators of Postoperative Clot Firmness in a Surgical Intensive Care Unit. Transfus. Med. Hemother. 2017, 44, 85–92. [Google Scholar] [CrossRef] [Green Version]
- Wettstein, P.; Haeberli, A.; Stutz, M.; Rohner, M.; Corbetta, C.; Gabi, K.; Schnider, T.; Korte, W. Decreased Factor XIII Availability for Thrombin and early Loss of Clot Firmness in Patients with Unexplained Intraoperative Bleeding. Anesth. Analg. 2004, 99, 1564–1569. [Google Scholar] [CrossRef]
- Korte, W.; Truttmann, B.; Heim, C.; Stangl, U.; Schmid, L.; Kreienbühl, G. Preoperative values of molecular coagulation markers identify patients at low risk for intraoperative haemostatic disorders and excessive blood loss. Clin. Chem. Lab. Med. 1998, 36, 235–240. [Google Scholar] [CrossRef]
- Godje, O.; Gallmeier, U.; Schelian, M.; Grunewald, M.; Mair, H. Coagulation factor XIII reduces postoperative bleeding after coronary surgery with extracorporeal circulation. Thorac. Cardiovasc. Surg. 2006, 54, 26–33. [Google Scholar] [CrossRef]
- Godje, O.; Haushofer, M.; Lamm, P.; Reichart, B. The effect of factor XIII on bleeding in coronary surgery. Thorac. Cardiovasc. Surg. 1998, 46, 263–267. [Google Scholar] [CrossRef]
- Gerlach, R.; Tolle, F.; Raabe, A.; Zimmermann, M.; Siegemund, A.; Seifert, V. Increased risk for postoperative hemorrhage after intracranial surgery in patients with decreased factor XIII activity: Implications of a prospective study. Stroke 2002, 33, 1618–1623. [Google Scholar] [CrossRef] [Green Version]
- Korte, W.; Szadkowski, C.; Gähler, A.; Gabi, K.; Kownacki, E.; Eder, M.; Degiacomi, P.; Zoller, N.; DeVay, J.; Lange, J.; et al. Factor XIII substitution in surgical cancer patients at high risk for intraoperative bleeding. Anesthesiology 2009, 110, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Beyerle, A.; Solomon, C.; Dickneite, G.; Herzog, E. Nonclinical analysis of the safety, pharmacodynamnics, and pharmacokinetics of plasma-derived human FXIII concentrate in animals. Pharmacol. Res. Perspect. 2016, 4, e00227. [Google Scholar] [CrossRef] [PubMed]
- Oswald, E.; Stalzer, B.; Heitz, E.; Weiss, M.; Schmugge, M.; Strasak, A.; Innerhofer, P.; Haas, T. Thromboelastrometry (ROTEM) in children: Age–related reference ranges and correlations with standard coagulation tests. Br. J. Anaesth. 2010, 105, 827–835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karlsson, M.; Ternström, L.; Hyllner, M.; Baghaei, F.; Nilsson, S.; Jeppsson, A. Plasma fibrinogen level, bleeding, and transfusion after on-pump coronary artery bypass grafting surgery: A prospective observational study. Transfusion 2008, 48, 2152–2158. [Google Scholar] [CrossRef] [PubMed]
- Chandler, W.L.; Patel, M.A.; Gravelle, L.; Soltow, L.O.; Bishop, P.D.; Spiess, B.D. Factor XIIIA and clot strength after cardiopulmonary bypass. Blood Coagul. Fibrinolysis 2001, 12, 101–108. [Google Scholar] [CrossRef]
- Theussinger, O.M.; Schröder, C.M.; Eismon, J.; Emmert, M.Y.; Seifert, B.; Spahn, D.R.; Baulig, B.W.; Baulig, W.T. The influence of laboratory coagulation tests and clotting factor levels on Rotation Thromboelastometry (ROTEM®) during major surgery with hemorrhage. Anesth. Analg. 2013, 117, 314–321. [Google Scholar] [CrossRef]
- Lison, S.; Weiss, G.; Spannagl, M.; Heindl, B. Postoperative changes in procoagulant factors after major surgery. Blood Coagul. Fibrinolyses 2011, 22, 190–196. [Google Scholar] [CrossRef]
- MedCalc Software Ltd. MedCalc Statistical Software Version 19.4.0. Available online: https://www.medcalc.org (accessed on 6 July 2020).
- Koscielny, J.; Ziemer, S.; Radtke, H.; Schmutzler, M.; Pruss, A.; Sinha, P.; Salama, A.; Kesewetter, H.; Latza, R. A practical concept for preoperative identification of patients with impaired primary hemostasis. Clin. Appl. Thromb. Hemost. 2004, 10, 195–204. [Google Scholar] [CrossRef]
- Vries, M.J.; van der Meijden, P.E.; Kuiper, G.J.; Nelemans, P.J.; Wetzels, R.J.; van Oerle, R.G.; Lance, M.D.; ten Cate, H.; Henskens, Y.M. Preoperative screening for bleeding disorders: A comprehensive laboratory assessment of clinical practice. Res. Pract. Thromb. Haemost. 2018, 2, 767–777. [Google Scholar] [CrossRef]
- Gabi, K.; Rohner, M.; Gähler, A.; Szadkowski, C.; Schnider, T.W.; Lange, J.; Riesen, W.; Korte, W. Preoperative fibrin monomer measurement allows risk stratification for high intraoperative blood loss in elective surgery. Thromb. Haemost. 2005, 94, 211–215. [Google Scholar] [CrossRef]
- Haslinger, C.; Korte, W.; Hothorn, T.; Brun, R.; Greenberg, C.; Zimmermann, R. The impact of prepartum factor XIII activity on postpartum blood loss. J. Thromb. Haemost. 2020. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Karkouti, K.; von Heymann, C.; Jespersen, C.M.; Korte, W.; Levy, J.H.; Ranucci, M.; Selke, F.W.; Song, H.K. Efficacy and safety of recombinant factor XIII on reducing blood transfusions in cardiac surgery: A randomized, placebo-controlled, multicenter clinical trial. J. Thorac. Cardiovasc. Surg. 2013, 146, 927–939. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| FXIII Activity (%) | Fibrinogen (g/L) | Platelets (G/L) | n | Proportion |
|---|---|---|---|---|
| <70 | any | any | 515 | 50% |
| <60 | any | any | 399 | 39% |
| any | <1.5 | any | 93 | 9% |
| any | <1.0 | any | 25 | 2% |
| any | any | <150 | 503 | 49% |
| any | any | <100 | 249 | 24% |
| FXIII Activity (%) | Fibrinogen (g/L) | Platelets (G/L) | n | Proportion | |||
|---|---|---|---|---|---|---|---|
| A | ≥70 | and | ≥1.5 | and | ≥150 | 302 | 30% |
| B | <70 | and | ≥1.5 | and | <150 | 229 | 22% |
| C | <70 | and | ≥1.5 | and | ≥150 | 204 | 20% |
| D | ≥70 | and | ≥1.5 | and | <150 | 195 | 19% |
| E | <70 | and | <1.5 | and | <150 | 72 | 7% |
| F | <70 | and | <1.5 | and | ≥150 | 10 | <1% |
| G | ≥70 | and | <1.5 | and | <150 | 7 | <1% |
| H | ≥70 | and | <1.5 | and | ≥150 | 4 | <1% |
| Variables Evaluated | OR | OR 95% CI |
|---|---|---|
| FXIII activity < 70% | 4.62 | 3.49–6.11 |
| Platelet count < 150 G/L | 1.96 | 1.48–2.59 |
| Fibrinogen < 1.5 g/L | 1.08 | 0.67–1.76 |
| FXIII < 70% AND platelets < 150 G/L | 3.18 | 2.35–4.31 |
| FXIII < 70% AND fibrinogen < 1.5 g/L | 2.51 | 0.89–7.07 |
| Platelets < 150 G/L AND fibrinogen < 1.5 g/L | 0.60 | 0.20–1.76 |
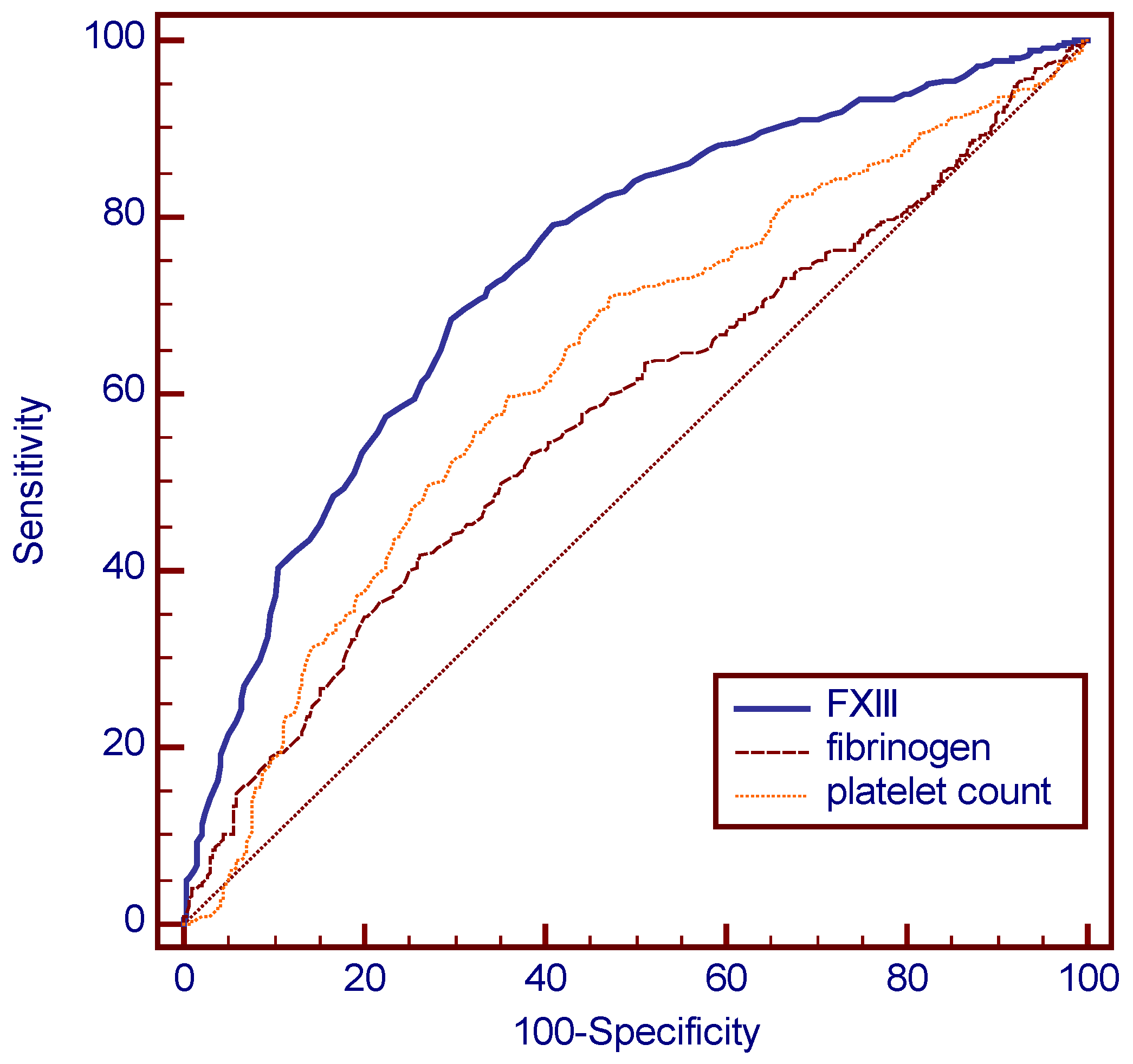
| Variables Evaluated | AUC | AUC 95% CI |
|---|---|---|
| FXIII activity < 70% | 0.744 | 0.716–0.770 |
| Platelet Count < 150 G/L | 0.632 | 0.601–0.661 |
| Fibrinogen Concentration < 1.5 g/L | 0.578 | 0.547–0.609 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Listyo, S.; Forrest, E.; Graf, L.; Korte, W. The Need for Red Cell Support During Non-Cardiac Surgery Is Associated to Pre-Transfusion Levels of FXIII and the Platelet Count. J. Clin. Med. 2020, 9, 2456. https://doi.org/10.3390/jcm9082456
Listyo S, Forrest E, Graf L, Korte W. The Need for Red Cell Support During Non-Cardiac Surgery Is Associated to Pre-Transfusion Levels of FXIII and the Platelet Count. Journal of Clinical Medicine. 2020; 9(8):2456. https://doi.org/10.3390/jcm9082456
Chicago/Turabian StyleListyo, Silke, Eric Forrest, Lukas Graf, and Wolfgang Korte. 2020. "The Need for Red Cell Support During Non-Cardiac Surgery Is Associated to Pre-Transfusion Levels of FXIII and the Platelet Count" Journal of Clinical Medicine 9, no. 8: 2456. https://doi.org/10.3390/jcm9082456