New Ultrasound Technologies for Ischemic Heart Disease Assessment and Monitoring in Cardiac Rehabilitation

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
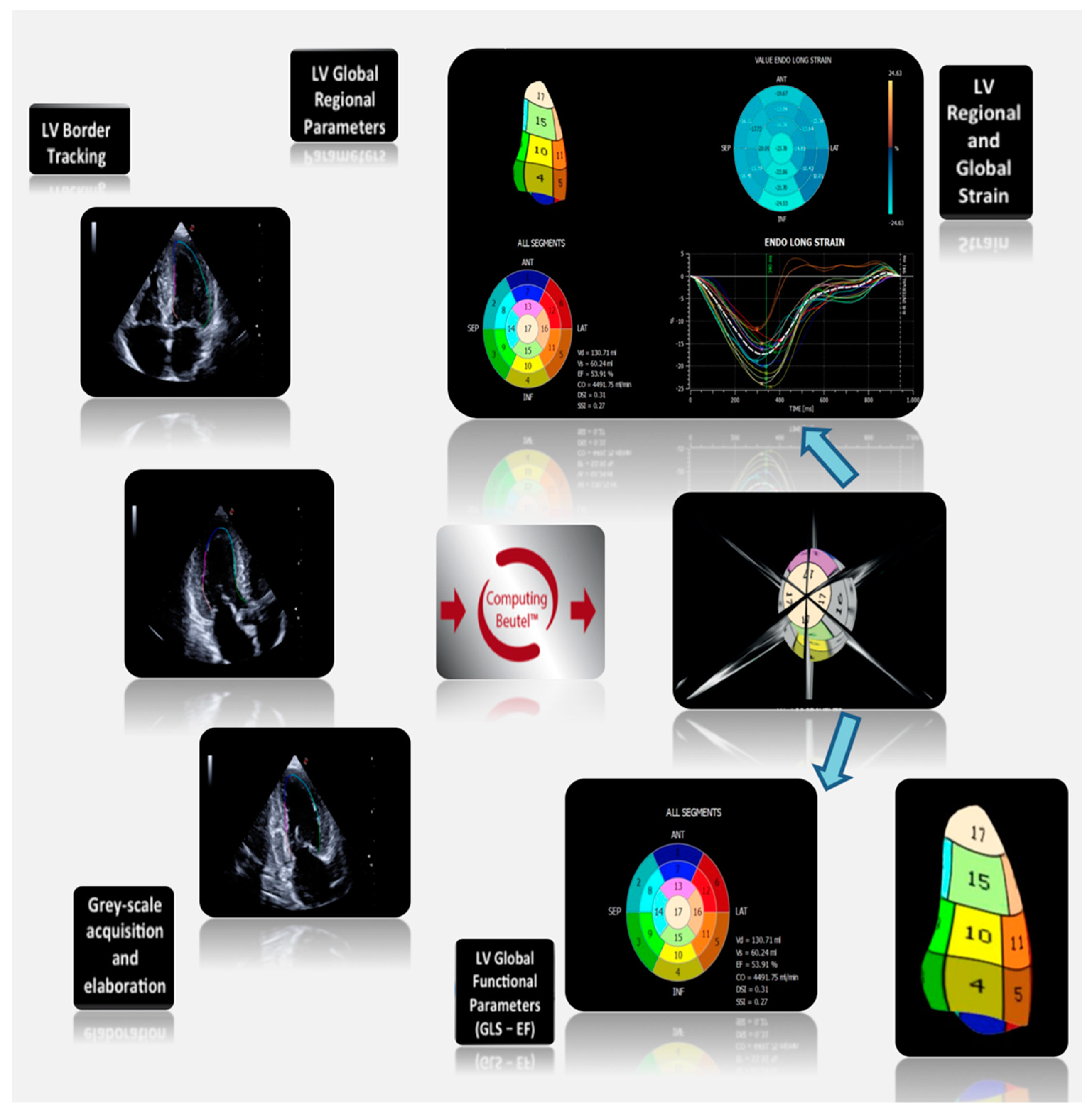
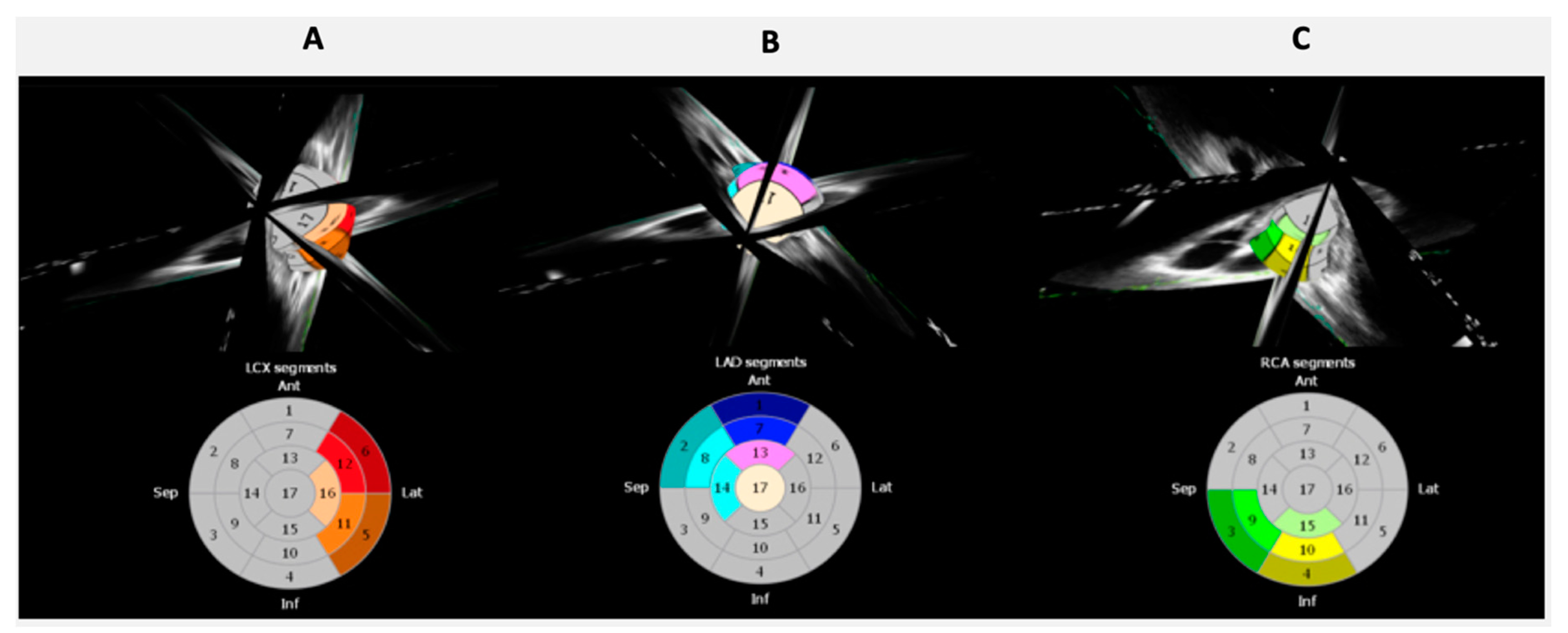
2. Left Ventricular Strain
Role of LV Strain in IHD
3. Left Atrial Strain
Role of LA Strain in IHD
4. Tissue Doppler Imaging (TDI)
Role of TDI in IHD
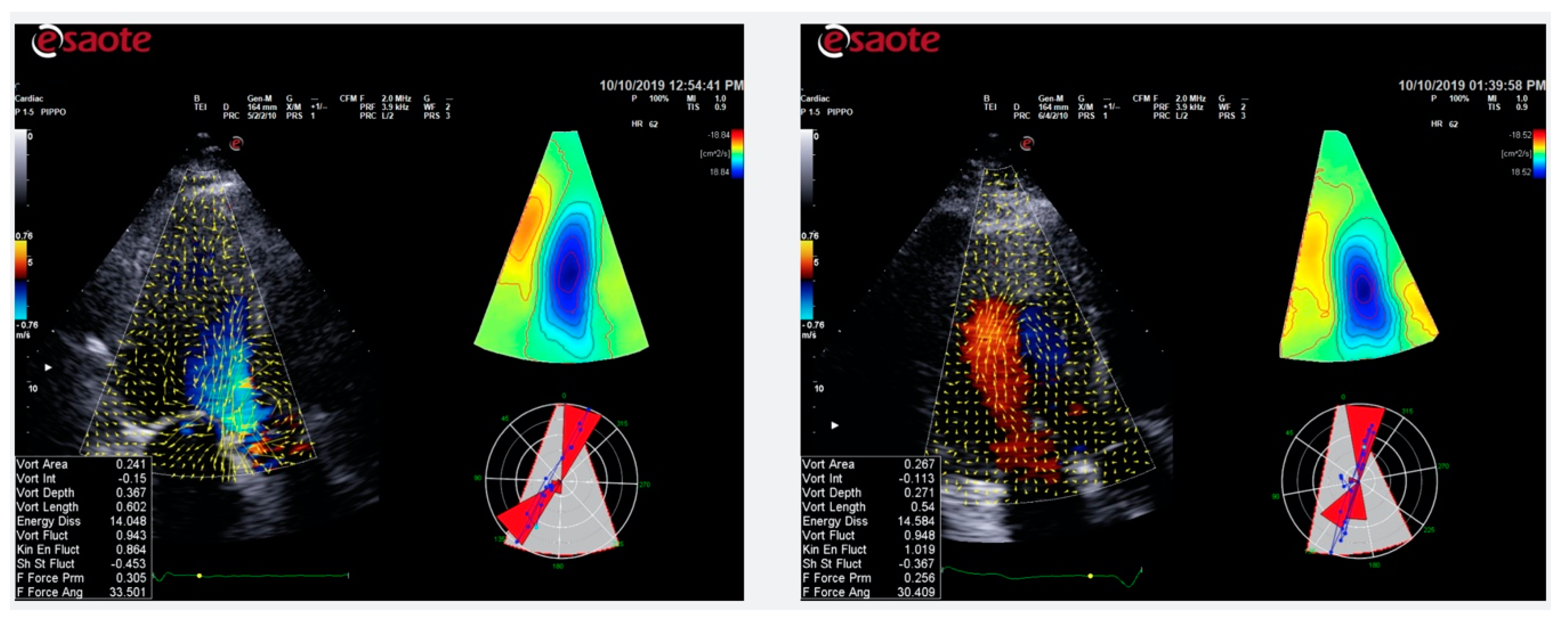
5. Color Doppler Flow Mapping
Role of CDFM in IHD
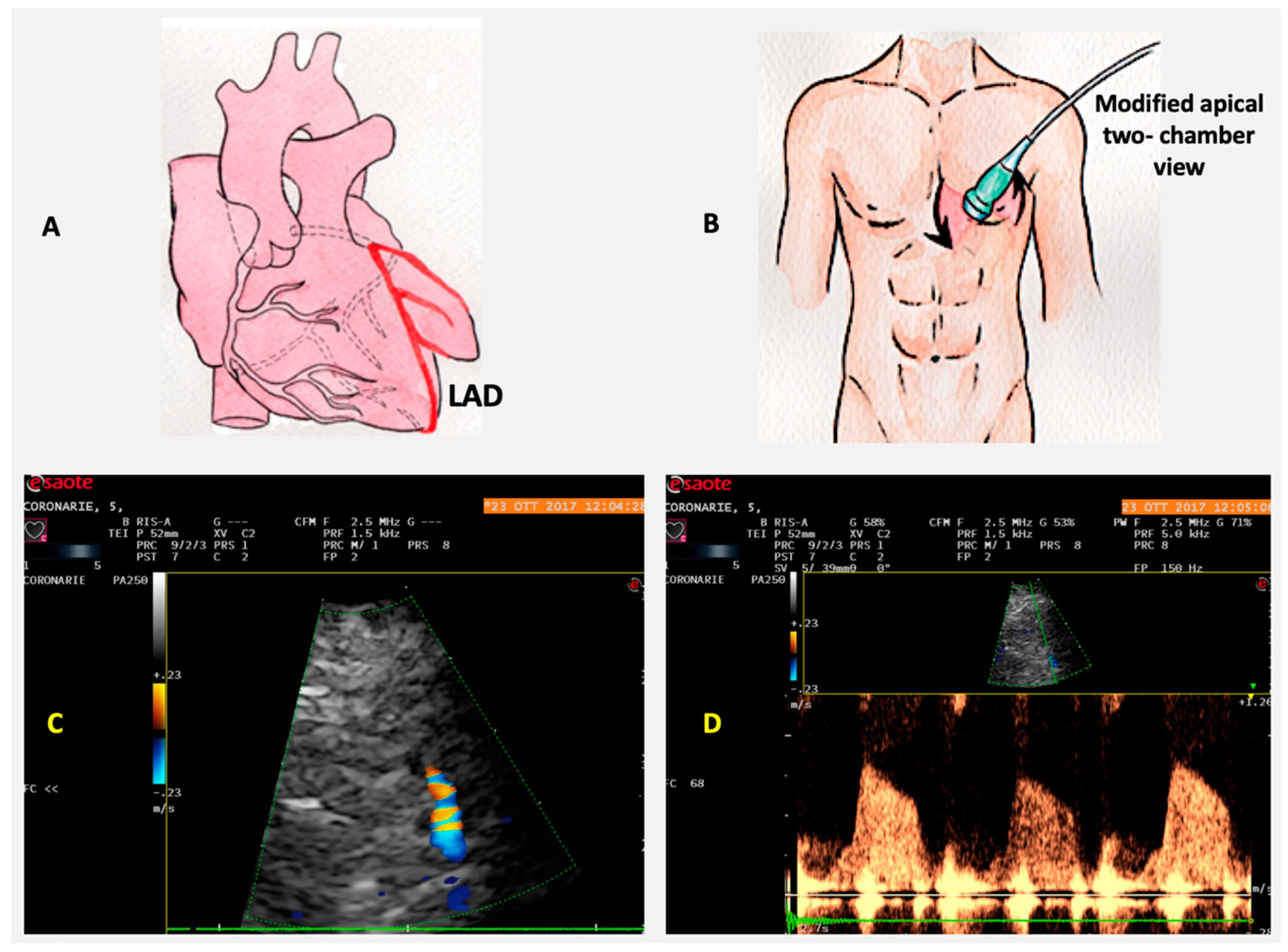
6. Coronary Flow Reserve
Role of CFR in IHD
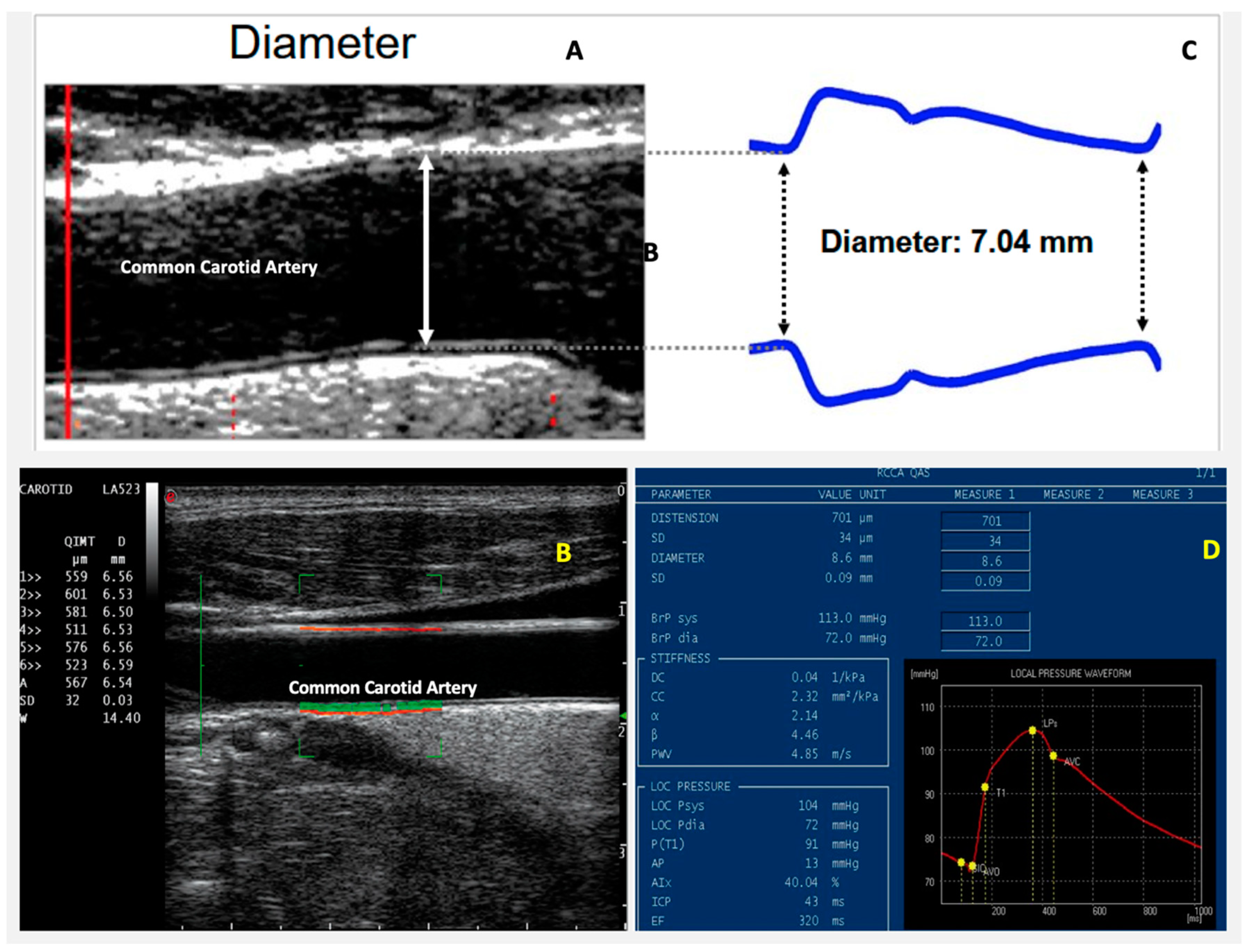
7. Arterial Stiffness
Role of Arterial Stiffness in IHD
8. Advantages and Limitations of the New Ultrasound Technologies
9. Cardiac Rehabilitation and New Echocardiographic Technologies
10. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Nowbar, A.N.; Gitto, M.; Howard, J.P.; Francis, D.P.; Al-Lamee, R. Mortality from ischemic heart disease. Circ. Cardiovasc. Qual. Outcomes 2019, 12, e005375. [Google Scholar] [CrossRef] [PubMed]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 2019, 41, 407–477. [Google Scholar] [CrossRef] [PubMed]
- Bansal, M.; Kasliwal, R.R. How do I do it? Speckle-tracking echocardiography. Indian Heart J. 2012, 65, 117–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muraru, D.; Niero, A.; Zanella, H.R.; Cherata, D.; Badano, L.P. Three-dimensional speckle-tracking echocardiography: Benefits and limitations of integrating myocardial mechanics with three-dimensional imaging. Cardiovasc. Diagn. Ther. 2018, 8, 101–117. [Google Scholar] [CrossRef] [Green Version]
- Omar, A.M.S.; Bansal, M.; Sengupta, P.P. Advances in echocardiographic imaging in heart failure with reduced and preserved ejection fraction. Circ. Res. 2016, 119, 357–374. [Google Scholar] [CrossRef]
- Weidemann, F.; Wacker, C.; Rauch, A.; Bauer, W.R.; Bijnens, B.; Sutherland, G.R.; Ertl, G.; Voelker, W.; Fidler, F.; Strotmann, J. Sequential changes of myocardial function during acute myocardial infarction, in the early and chronic phase after coronary intervention described by ultrasonic strain rate imaging. J. Am. Soc. Echocardiogr. 2006, 19, 839–847. [Google Scholar] [CrossRef]
- Cimino, S.; Canali, E.; Petronilli, V.; Cicogna, F.; De Luca, L.; Francone, M.; Sardella, G.; Iacoboni, C.; Agati, L. Global and regional longitudinal strain assessed by two-dimensional speckle tracking echocardiography identifies early myocardial dysfunction and transmural extent of myocardial scar in patients with acute ST elevation myocardial infarction and relatively preserved LV function. Eur. Heart J. Cardiovasc. Imaging 2012, 14, 805–811. [Google Scholar] [CrossRef]
- Liu, C.; Li, J.; Ren, M.; Wang, Z.-Z.; Li, Z.-Y.; Gao, F.; Tian, J.-W. Multilayer longitudinal strain at rest may help to predict significant stenosis of the left anterior descending coronary artery in patients with suspected non-ST-elevation acute coronary syndrome. Int. J. Cardiovasc. Imaging 2016, 32, 1675–1685. [Google Scholar] [CrossRef]
- Sarvari, S.I.; Haugaa, K.H.; Zahid, W.; Bendz, B.; Aakhus, S.; Aaberge, L.; Edvardsen, T. Layer-specific quantification of myocardial deformation by strain echocardiography may reveal significant CAD in patients with non–ST-segment elevation acute coronary syndrome. JACC Cardiovasc. Imaging 2013, 6, 535–544. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Wu, W.-C.; Ma, H.; Wang, H. Usefulness of layer-specific strain for identifying complex CAD and predicting the severity of coronary lesions in patients with non-ST-segment elevation acute coronary syndrome: Compared with Syntax score. Int. J. Cardiol. 2016, 223, 1045–1052. [Google Scholar] [CrossRef]
- Hutyra, M.; Skala, T.; Horak, D.; Kocher, M.; Tüdös, Z.; Zapletalová, J.; Přeček, J.; Louis, A.; Smékal, A.; Taborsky, M. Echocardiographic assessment of global longitudinal right ventricular function in patients with an acute inferior ST elevation myocardial infarction and proximal right coronary artery occlusion. Int. J. Cardiovasc. Imaging 2014, 31, 497–507. [Google Scholar] [CrossRef] [PubMed]
- D’Andrea, A.; Radmilovic, J.; Mele, D.; D’Ascenzi, F.; Agricola, E.; Carbone, A.; Iudice, F.L.; Novo, G.; Ancona, F.; Righini, F.M.; et al. Speckle tracking analysis in intensive care unit: A toy or a tool? Echocardiography 2018, 35, 506–519. [Google Scholar] [CrossRef] [PubMed]
- Woo, J.S.; Kim, W.-S.; Yu, T.-K.; Ha, S.J.; Kim, S.Y.; Bae, J.-H.; Kim, K.S. Prognostic value of serial global longitudinal strain measured by two-dimensional speckle tracking echocardiography in patients with ST-segment elevation myocardial infarction. Am. J. Cardiol. 2011, 108, 340–347. [Google Scholar] [CrossRef] [PubMed]
- Hung, C.-L.; Verma, A.; Uno, H.; Shin, S.-H.; Bourgoun, M.; Hassanein, A.; McMurray, J.J.; Velazquez, E.J.; Kober, L.; Pfeffer, M.A.; et al. Longitudinal and circumferential strain rate, left ventricular remodeling, and prognosis after myocardial infarction. J. Am. Coll. Cardiol. 2010, 56, 1812–1822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ersbøll, M.; Valeur, N.; Andersen, M.J.; Mogensen, U.M.; Vinther, M.; Svendsen, J.H.; Moller, J.E.; Kisslo, J.; Velazquez, E.J.; Hassager, C.; et al. Early echocardiographic deformation analysis for the prediction of sudden cardiac death and life-threatening arrhythmias after myocardial infarction. JACC Cardiovasc. Imaging 2013, 6, 851–860. [Google Scholar] [CrossRef] [Green Version]
- Antoni, M.L.; Mollema, S.A.; Atary, J.Z.; Borleffs, C.J.W.; Boersma, E.; Van De Veire, N.R.; Holman, E.R.; Van Der Wall, E.E.; Schalij, M.J.; Bax, J.J. Time course of global left ventricular strain after acute myocardial infarction. Eur. Heart J. 2010, 31, 2006–2013. [Google Scholar] [CrossRef] [Green Version]
- D’Andrea, A.; Mele, D.; Agricola, E.; Pezzullo, E.; Cameli, M.; Rossi, A.; Esposito, R.; Novo, G.; Mondillo, S.; Montisci, R.; et al. XStrain 4D analysis predicts left ventricular remodeling in patients with recent non-ST-segment elevation myocardial infarction. Int. J. Cardiol. 2016, 206, 107–109. [Google Scholar] [CrossRef]
- D’Andrea, A.; Cocchia, R.; Caso, P.; Riegler, L.; Scarafile, R.; Salerno, G.; Golia, E.; Di Salvo, G.; Calabrò, P.; Cappelli-Bigazzi, M.; et al. Global longitudinal speckle-tracking strain is predictive of left ventricular remodeling after coronary angioplasty in patients with recent non-st elevation myocardial infarction. Int. J. Cardiol. 2011, 153, 185–191. [Google Scholar] [CrossRef]
- D’Andrea, A.; Caso, P.; Scarafile, R.; Riegler, L.; Salerno, G.; Castaldo, F.; Gravino, R.; Cocchia, R.; Del Viscovo, L.; Limongelli, G.; et al. Effects of global longitudinal strain and total scar burden on response to cardiac resynchronization therapy in patients with ischaemic dilated cardiomyopathy. Eur. J. Heart Fail. 2009, 11, 58–67. [Google Scholar] [CrossRef]
- Ersboll, M.K.; Andersen, M.J.; Valeur, N.; Mogensen, U.M.; Waziri, H.; Moller, J.E.; Hassager, C.; Søgaard, P.; Kober, L. The prognostic value of left atrial peak reservoir strain in acute myocardial infarction is dependent on left ventricular longitudinal function and left atrial size. Circ. Cardiovasc. Imaging 2013, 6, 26–33. [Google Scholar] [CrossRef] [Green Version]
- Leung, M.; Abou, R.; Van Rosendael, P.J.; Van Der Bijl, P.; Van Wijngaarden, S.E.; Regeer, M.V.; Podlesnikar, T.; Marsan, N.A.; Leung, D.Y.; Delgado, V.; et al. Relation of echocardiographic markers of left atrial fibrosis to atrial fibrillation burden. Am. J. Cardiol. 2018, 122, 584–591. [Google Scholar] [CrossRef] [PubMed]
- Pathan, F.; D’Elia, N.; Nolan, M.; Marwick, T.H.; Negishi, K. Normal ranges of left atrial strain by speckle-tracking echocardiography: A systematic review and meta-analysis. J. Am. Soc. Echocardiogr. 2017, 30, 59–70.e8. [Google Scholar] [CrossRef] [PubMed]
- D’Andrea, A.; Caso, P.; Romano, S.; Scarafile, R.; Cuomo, S.; Salerno, G.; Riegler, L.; Limongelli, G.; Di Salvo, G.; Romanò, M.; et al. Association between left atrial myocardial function and exercise capacity in patients with either idiopathic or ischemic dilated cardiomyopathy: A two-dimensional speckle strain study. Int. J. Cardiol. 2009, 132, 354–363. [Google Scholar] [CrossRef] [PubMed]
- D’Andrea, A.; Caso, P.; Romano, S.; Scarafile, R.; Riegler, L.; Salerno, G.; Limongelli, G.; Di Salvo, G.; Calabrò, P.; Del Viscovo, L.; et al. Different effects of cardiac resynchronization therapy on left atrial function in patients with either idiopathic or ischaemic dilated cardiomyopathy: A two-dimensional speckle strain study. Eur. Heart J. 2007, 28, 2738–2748. [Google Scholar] [CrossRef] [PubMed]
- D’Andrea, A.; Scarafile, R.; Riegler, L.; Salerno, G.; Gravino, R.; Cocchia, R.; Castaldo, F.; Allocca, F.; Limongelli, G.; Di Salvo, G.; et al. Right atrial size and deformation in patients with dilated cardiomyopathy undergoing cardiac resynchronization therapy. Eur. J. Heart Fail. 2009, 11, 1169–1177. [Google Scholar] [CrossRef]
- Ancona, R.; Pinto, S.C.; Caso, P.; D’Andrea, A.; Di Salvo, G.; Arenga, F.; Coppola, M.G.; Sellitto, V.; Macrino, M.; Calabro, R. Left atrium by echocardiography in clinical practice: From conventional methods to new echocardiographic techniques. Sci. World J. 2014, 2014, 1–15. [Google Scholar] [CrossRef]
- Ancona, R.; Pinto, S.C.; Caso, P.; Di Salvo, G.; Severino, S.; D’Andrea, A.; Calabro, R. Two-dimensional atrial systolic strain imaging predicts atrial fibrillation at 4-year follow-up in asymptomatic rheumatic mitral stenosis. J. Am. Soc. Echocardiogr. 2013, 26, 270–277. [Google Scholar] [CrossRef]
- Carluccio, E.; Biagioli, P.; Mengoni, A.; Cerasa, M.F.; Lauciello, R.; Zuchi, C.; Bardelli, G.; Alunni, G.; Coiro, S.; Gronda, E.G.; et al. Left atrial reservoir function and outcome in heart failure with reduced ejection fraction. Circ. Cardiovasc. Imaging 2018, 11, 007696. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.-Y.; Xie, M.; Xu, J.-F.; Wang, X.-F.; Lv, Q.; Lu, X.-F.; Wang, J.; He, L.; Fang, L.-Y.; Zhang, J. Evaluation of Left Atrial Function in Patients with Coronary Artery Disease by Two-Dimensional Strain and Strain Rate Imaging. Echocardiography 2011, 28, 1095–1103. [Google Scholar] [CrossRef] [PubMed]
- Othman, K.M.S.; Nassar, A.I.; Fouad, A.; Ramzy, A.A.; Allah, M.F.F.A. Left atrial deformation analysis as a predictor of severity of coronary artery disease. Egypt. Heart J. 2018, 70, 353–359. [Google Scholar] [CrossRef]
- Stefanadis, C.; Dernellis, J.; Tsiamis, E.; Toutouzas, P. Effects of pacing-induced and balloon coronary occlusion ischemia on left atrial function in patients with coronary artery disease. J. Am. Coll. Cardiol. 1999, 33, 687–696. [Google Scholar] [CrossRef] [Green Version]
- Correale, M.; Totaro, A.; Ieva, R.; Ferraretti, A.; Musaico, F.; Di Biase, M. Tissue Doppler imaging in coronary artery diseases and heart failure. Curr. Cardiol. Rev. 2012, 8, 43–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agarwal, R.; Gosain, P.; Kirkpatrick, J.N.; Alyousef, T.; Doukky, R.; Singh, G.; Umscheid, C.A. Tissue Doppler imaging for diagnosis of coronary artery disease: A systematic review and meta-analysis. Cardiovasc. Ultrasound 2012, 10, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eek, C.; Grenne, B.; Brunvand, H.; Aakhus, S.; Endresen, K.; Smiseth, O.A.; Edvardsen, T.; Skulstad, H. Postsystolic shortening is a strong predictor of recovery of systolic function in patients with non-ST-elevation myocardial infarction. Eur. J. Echocardiogr. 2011, 12, 483–489. [Google Scholar] [CrossRef] [Green Version]
- Hosokawa, H.; Sheehan, F.H.; Suzuki, T. Measurement of postsystolic shortening to assess viability and predict recovery of left ventricular function after acute myocardial infarction. J. Am. Coll. Cardiol. 2000, 35, 1842–1849. [Google Scholar] [CrossRef] [Green Version]
- Song, J.-K.; Song, J.-M.; Kang, D.-H.; Haluska, B.; Marwick, T.H. Postsystolic thickening detected by doppler myocardial imaging: A marker of viability or ischemia in patients with myocardial infarction. Clin. Cardiol. 2006, 27, 29–32. [Google Scholar] [CrossRef]
- Terkelsen, C.J.; Poulsen, S.H.; Nørgaard, B.L.; Lassen, J.F.; Gerdes, J.C.; Sloth, E.; Nielsen, T.T.; Andersen, H.R.; Egeblad, H. Does Postsystolic motion or shortening predict recovery of myocardial function after primary Percutanous coronary intervention? J. Am. Soc. Echocardiogr. 2007, 20, 505–511. [Google Scholar] [CrossRef]
- Brainin, P.; Haahr-Pedersen, S.; Sengeløv, M.; Olsen, F.J.; Fritz-Hansen, T.; Jensen, J.S.; Biering-Sørensen, T. Presence of post-systolic shortening is an independent predictor of heart failure in patients following ST-segment elevation myocardial infarction. Int. J. Cardiovasc. Imaging 2017, 34, 751–760. [Google Scholar] [CrossRef]
- Mele, D.; Smarrazzo, V.; Pedrizzetti, G.; Capasso, F.; Pepe, M.; Severino, S.; Luisi, G.A.; Maglione, M.; Ferrari, R. Intracardiac flow analysis: Techniques and potential clinical applications. J. Am. Soc. Echocardiogr. 2019, 32, 319–332. [Google Scholar] [CrossRef]
- Agati, L.; Cimino, S.; Tonti, G.; Cicogna, F.; Petronilli, V.; De Luca, L.; Iacoboni, C.; Pedrizzetti, G. Quantitative analysis of intraventricular blood flow dynamics by echocardiographic particle image velocimetry in patients with acute myocardial infarction at different stages of left ventricular dysfunction. Eur. Heart J.-Cardiovasc. Imaging 2014, 15, 1203–1212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, B.T.; Yeoh, H.K.; Liew, Y.M.; Dokos, S.; Al Abed, A.; Chee, K.H.; Aziz, Y.F.A.; Sridhar, G.S.; Chinna, K.; Lim, E. Quantitative analysis of intraventricular flow-energetics and vortex in ischaemic hearts. Coron. Artery Dis. 2018, 29, 316–324. [Google Scholar] [CrossRef] [PubMed]
- Nucifora, G.; Delgado, V.; Bertini, M.; Marsan, N.A.; Van De Veire, N.R.; Ng, A.C.T.; Siebelink, H.-M.J.; Schalij, M.J.; Holman, E.R.; Sengupta, P.P.; et al. Left ventricular muscle and fluid mechanics in acute myocardial infarction. Am. J. Cardiol. 2010, 106, 1404–1409. [Google Scholar] [CrossRef] [PubMed]
- Son, J.-W.; Park, W.-J.; Choi, J.-H.; Houle, H.; Vannan, M.A.; Hong, G.-R.; Chung, N. Abnormal left ventricular vortex flow patterns in association with left ventricular apical thrombus formation in patients with anterior myocardial infarction. Circ. J. 2012, 76, 2640–2646. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trocino, G. Italian Society of Cardiovascular Echography (SIEC) Consensus Conference on the state of the art of contrast echocardiography. Ital. Heart. J. Off. J. Ital. Fed. Cardiol. 2004, 5, 309–334. [Google Scholar]
- Zagatina, A.; Zhuravskaya, N.; Shmatov, D.; Ciampi, Q.; Carpeggiani, C.; Picano, E. Exercise stress echocardiography with ABCDE protocol in unexplained dyspnoea. Int. J. Cardiovasc. Imaging 2020, 1–9. [Google Scholar] [CrossRef]
- Scali, M.C.; Zagatina, A.; Ciampi, Q.; Cortigiani, L.; D’Andrea, A.; Djordjevic-Dikic, A.; Merlo, P.M.; Lattanzi, F.; Simova, I.; Monte, I.P.; et al. The functional meaning of B-Profile during stress lung ultrasound. JACC Cardiovasc. Imaging 2019, 12, 928–930. [Google Scholar] [CrossRef]
- Gan, L.-M.; Svedlund, S.; Wittfeldt, A.; Eklund, C.; Gao, S.; Matejka, G.; Jeppsson, A.; Albertsson, P.; Omerovic, E.; Lerman, A. Incremental value of transthoracic doppler echocardiography-assessed coronary flow reserve in patients with suspected myocardial ischemia undergoing myocardial perfusion Scintigraphy. J. Am. Heart Assoc. 2017, 6, e004875. [Google Scholar] [CrossRef] [Green Version]
- Haraldsson, I.; Gan, L.-M.; Svedlund, S.; Wittfeldt, A.; Råmunddal, T.; Angerås, O.; Albertsson, P.; Matejka, G.; Omerovic, E. Non-invasive evaluation of coronary flow reserve with transthoracic Doppler echocardiography predicts the presence of significant stenosis in coronary arteries. Int. J. Cardiol. 2014, 176, 294–297. [Google Scholar] [CrossRef]
- Rahmani, M.; Cruz, R.P.; Granville, D.J.; McManus, B.M. Allograft Vasculopathy versus atherosclerosis. Circ. Res. 2006, 99, 801–815. [Google Scholar] [CrossRef]
- Sade, L.E.; Eroğlu, S.; Yuce, D.; Bircan, A.; Pirat, B.; Sezgin, A.; Aydınalp, A.; Muderrisoglu, H.; Bircan, A.; Aydinalp, A. Follow-up of heart transplant recipients with serial echocardiographic coronary flow reserve and Dobutamine stress echocardiography to detect cardiac allograft Vasculopathy. J. Am. Soc. Echocardiogr. 2014, 27, 531–539. [Google Scholar] [CrossRef]
- Feola, M.; Testa, M.; Ferreri, C.; Rosso, G.; Rossi, A.; Ruocco, G. The analysis of arterial stiffness in heart failure patients in comparison with healthy subjects and patients with cardiovascular risk factors. J. Clin. Med. 2019, 8, 1721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ikonomidis, I.; Makavos, G.; Lekakis, J.P. Arterial stiffness and coronary artery disease. Curr. Opin. Cardiol. 2015, 30. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, G.F.; Hwang, S.-J.; Vasan, R.S.; Larson, M.G.; Pencina, M.J.; Hamburg, N.M.; Vita, J.A.; Levy, D.; Benjamin, E.J. Arterial stiffness and cardiovascular events: The Framingham heart study. Circulation 2010, 121, 505–511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vlachopoulos, C.; Aznaouridis, K.; Stefanadis, C. Prediction of cardiovascular events and all-cause mortality with arterial stiffness: A systematic review and meta-analysis. J. Am. Coll. Cardiol. 2010, 55, 1318–1327. [Google Scholar] [CrossRef] [Green Version]
- Kaneko, H.; Yajima, J.; Oikawa, Y.; Matsuno, S.; Funada, R.; Tanaka, S.; Fukamachi, D.; Suzuki, S.; Aizawa, T.; Yamashita, T. Role of arterial stiffness and impaired renal function in the progression of new coronary lesions after percutaneous coronary intervention. Cardiovasc. Interv. Ther. 2012, 28, 56–62. [Google Scholar] [CrossRef]
- Nakamura, M.; Yamashita, T.; Yajima, J.; Oikawa, Y.; Sagara, K.; Koike, A.; Kirigaya, H.; Nagashima, K.; Sawada, H.; Aizawa, T.; et al. Brachial-ankle pulse wave velocity as a risk stratification index for the short-term prognosis of type 2 diabetic patients with coronary artery disease. Hypertens. Res. 2010, 33, 1018–1024. [Google Scholar] [CrossRef]
- Regnault, V.; Lagrange, J.; Pizard, A.; Safar, M.E.; Fay, R.; Pitt, B.; Challande, P.; Rossignol, P.; Zannad, F.; Lacolley, P. Opposite predictive value of pulse pressure and aortic pulse wave velocity on heart failure with reduced left ventricular ejection fraction: Insights from an Eplerenone Post-Acute Myocardial Infarction Heart Failure Efficacy and Survival Study (EPHESUS) substudy. Hypertension 2014, 63, 105–111. [Google Scholar] [CrossRef] [Green Version]
- Valkeinen, H.; Aaltonen, S.; Kujala, U.M. Effects of exercise training on oxygen uptake in coronary heart disease: A systematic review and meta-analysis. Scand. J. Med. Sci. Sports 2010, 20, 545–555. [Google Scholar] [CrossRef]
- Taylor, R.S.; Brown, A.; Ebrahim, S.; Jolliffe, J.; Noorani, H.; Rees, K.; Skidmore, B.; Stone, J.; Thompson, D.R.; Oldridge, N. Exercise-based rehabilitation for patients with coronary heart disease: Systematic review and meta-analysis of randomized controlled trials. Am. J. Med. 2004, 116, 682–692. [Google Scholar] [CrossRef]
- Giannuzzi, P.; Temporelli, P.; Corrà, U.; Tavazzi, T. Antiremodeling effect of long-term exercise training in patients with stable chronic heart failure results of the exercise in left ventricular dysfunction and chronic heart failure (ELVD-CHF) trial. ACC Curr. J. Rev. 2003, 12, 43. [Google Scholar] [CrossRef]
- Heran, B.S.; Chen, J.M.; Ebrahim, S.; Moxham, T.; Oldridge, N.; Rees, K.; Thompson, D.R.; Taylor, R. Exercise-based cardiac rehabilitation for coronary heart disease. Cochrane Database Syst. Rev. 2011, 001800. [Google Scholar] [CrossRef]
- Petrovic, M.T.; Djordjevic-Dikic, A.; Giga, V.; Boskovic, N.; Vukcevic, V.; Cvetic, V.; Mladenovic, A.; Radmili, O.; Markovic, Z.; Dobric, M.; et al. The coronary ARteriogenesis with combined Heparin and EXercise therapy in chronic refractory Angina (CARHEXA) trial: A double-blind, randomized, placebo-controlled stress echocardiographic study. Eur. J. Prev. Cardiol. 2020, 8. [Google Scholar] [CrossRef]
- Haykowsky, M.J.; Scott, J.; Esch, B.; Schopflocher, D.P.; Myers, J.; Paterson, I.; Warburton, D.E.; Jones, L.W.; Clark, A.M. A meta-analysis of the effects of exercise training on left ventricular remodeling following myocardial infarction: Start early and go longer for greatest exercise benefits on remodeling. Trials 2011, 12, 92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonzalez-Represas, A.; Mourot, L. Stroke volume and cardiac output measurement in cardiac patients during a rehabilitation program: Comparison between tonometry, impedancemetry and echocardiography. Int. J. Cardiovasc. Imaging 2019, 36, 447–455. [Google Scholar] [CrossRef]
- McGregor, G.; Stöhr, E.J.; Oxborough, D.; Kimani, P.K.; Shave, R. Effect of exercise training on left ventricular mechanics after acute myocardial infarction–an exploratory study. Ann. Phys. Rehabil. Med. 2018, 61, 119–124. [Google Scholar] [CrossRef]
- Trachsel, L.; David, L.; Gayda, M.; Henri, C.; Hayami, D.; Thorin-Trescases, N.; Thorin, É.; Blain, M.; Cossette, M.; Lalongé, J.; et al. The impact of high-intensity interval training on ventricular remodeling in patients with a recent acute myocardial infarction—A randomized training intervention pilot study. Clin. Cardiol. 2019, 42, 1222–1231. [Google Scholar] [CrossRef] [Green Version]
- Malfatto, G.; Revera, M.; Branzi, G.; Ciambellotti, F.; Giglio, A.; Blengino, S.; Oldani, M.; Facchini, C.; Parati, G.; Facchini, M. A brief period of intensive cardiac rehabilitation improves global longitudinal strain and diastolic function after a first uncomplicated myocardial infarction. Acta Cardiol. 2017, 72, 284–291. [Google Scholar] [CrossRef]
- Acar, R.D.; Bulut, M.; Ergun, S.; Yesin, M.; Alıcı, G.; Akcakoyun, M.; Alici, G. Effect of cardiac rehabilitation on left atrial functions in patients with acute myocardial infarction. Ann. Phys. Rehabil. Med. 2014, 57, 105–113. [Google Scholar] [CrossRef]
- Bokhari, S.; Schneider, R.H.; Salerno, J.W.; Rainforth, M.V.; Gaylord-King, C.; Nidich, S.I. Effects of cardiac rehabilitation with and without meditation on myocardial blood flow using quantitative positron emission tomography: A pilot study. J. Nucl. Cardiol. 2019, 1–12. [Google Scholar] [CrossRef]
- Laskey, W.K.; Siddiqi, S.; Wells, C.; Lueker, R. Improvement in arterial stiffness following cardiac rehabilitation. Int. J. Cardiol. 2013, 167, 2734–2738. [Google Scholar] [CrossRef]
- Oliveira, N.L.; Ribeiro, F.; Silva, G.; Alves, A.J.; Silva, N.; Guimarães, J.T.; Teixeira, M.; Oliveira, J. Effect of exercise-based cardiac rehabilitation on arterial stiffness and inflammatory and endothelial dysfunction biomarkers: A randomized controlled trial of myocardial infarction patients. Atherosclerosis 2015, 239, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Cieslik-Guerra, U.; Wierzbowska-Drabik, K.; Trzos, E.; Kaminski, M.; Kotas, R.; Rechcinski, T.; Kasprzak, J.; Napieralski, A.; Kurpesa, M. Cardiac rehabilitation reduces arterial stiffness independently of the coexistence of arterial hypertension (forever study). J. Hypertens. 2019, 37, e287. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Technology | Advantages | Limitations |
|---|---|---|
| Speckle tracking echocardiography |
|
|
| Tissue Doppler imaging |
|
|
| Color Doppler flow mapping |
|
|
| Coronary flow reserve |
|
|
| Carotid stiffness |
|
|
| Category | Traditional Indexes | New Technologies Indexes |
|---|---|---|
| LV dimension and systolic function |
|
|
| LV diastolic function |
|
|
| LA dimension and function |
|
|
| RV dimension and systolic function |
|
|
| Arterial stiffness | / |
|
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Andrea, A.; Sperlongano, S.; Pacileo, M.; Venturini, E.; Iannuzzo, G.; Gentile, M.; Sperlongano, R.; Vitale, G.; Maglione, M.; Cice, G.; et al. New Ultrasound Technologies for Ischemic Heart Disease Assessment and Monitoring in Cardiac Rehabilitation. J. Clin. Med. 2020, 9, 3131. https://doi.org/10.3390/jcm9103131
D’Andrea A, Sperlongano S, Pacileo M, Venturini E, Iannuzzo G, Gentile M, Sperlongano R, Vitale G, Maglione M, Cice G, et al. New Ultrasound Technologies for Ischemic Heart Disease Assessment and Monitoring in Cardiac Rehabilitation. Journal of Clinical Medicine. 2020; 9(10):3131. https://doi.org/10.3390/jcm9103131
Chicago/Turabian StyleD’Andrea, Antonello, Simona Sperlongano, Mario Pacileo, Elio Venturini, Gabriella Iannuzzo, Marco Gentile, Rossella Sperlongano, Giuseppe Vitale, Marco Maglione, Gennaro Cice, and et al. 2020. "New Ultrasound Technologies for Ischemic Heart Disease Assessment and Monitoring in Cardiac Rehabilitation" Journal of Clinical Medicine 9, no. 10: 3131. https://doi.org/10.3390/jcm9103131