Mitral Valve Repair of Atrial Functional Mitral Regurgitation in Heart Failure with Preserved Ejection Fraction

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
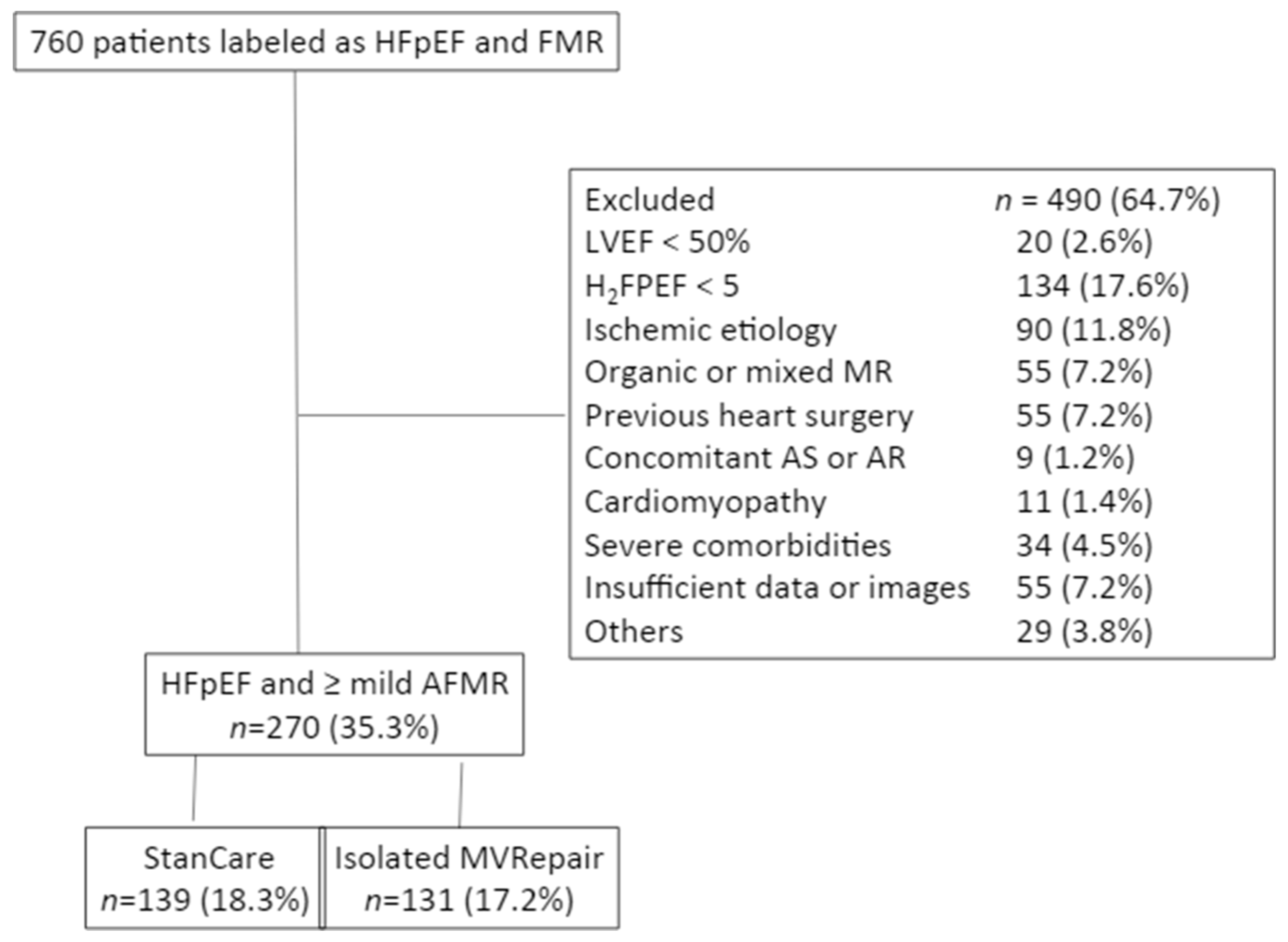
2.2. Study Population
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Periprocedural and 30-Day Outcome in the MVRepair Group
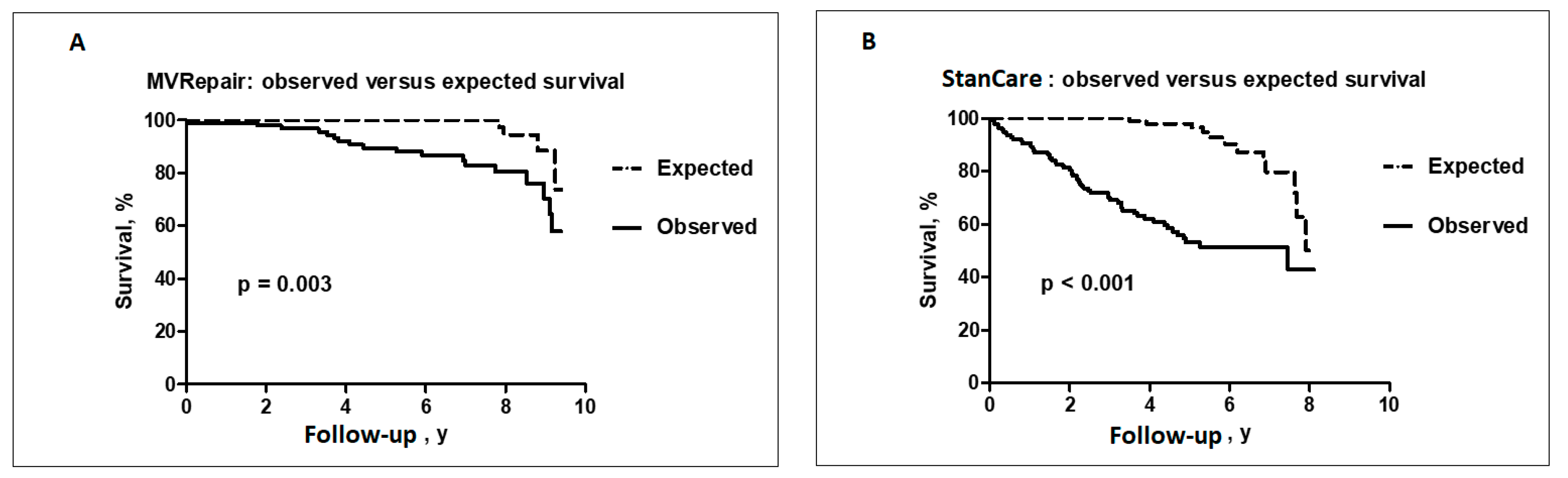
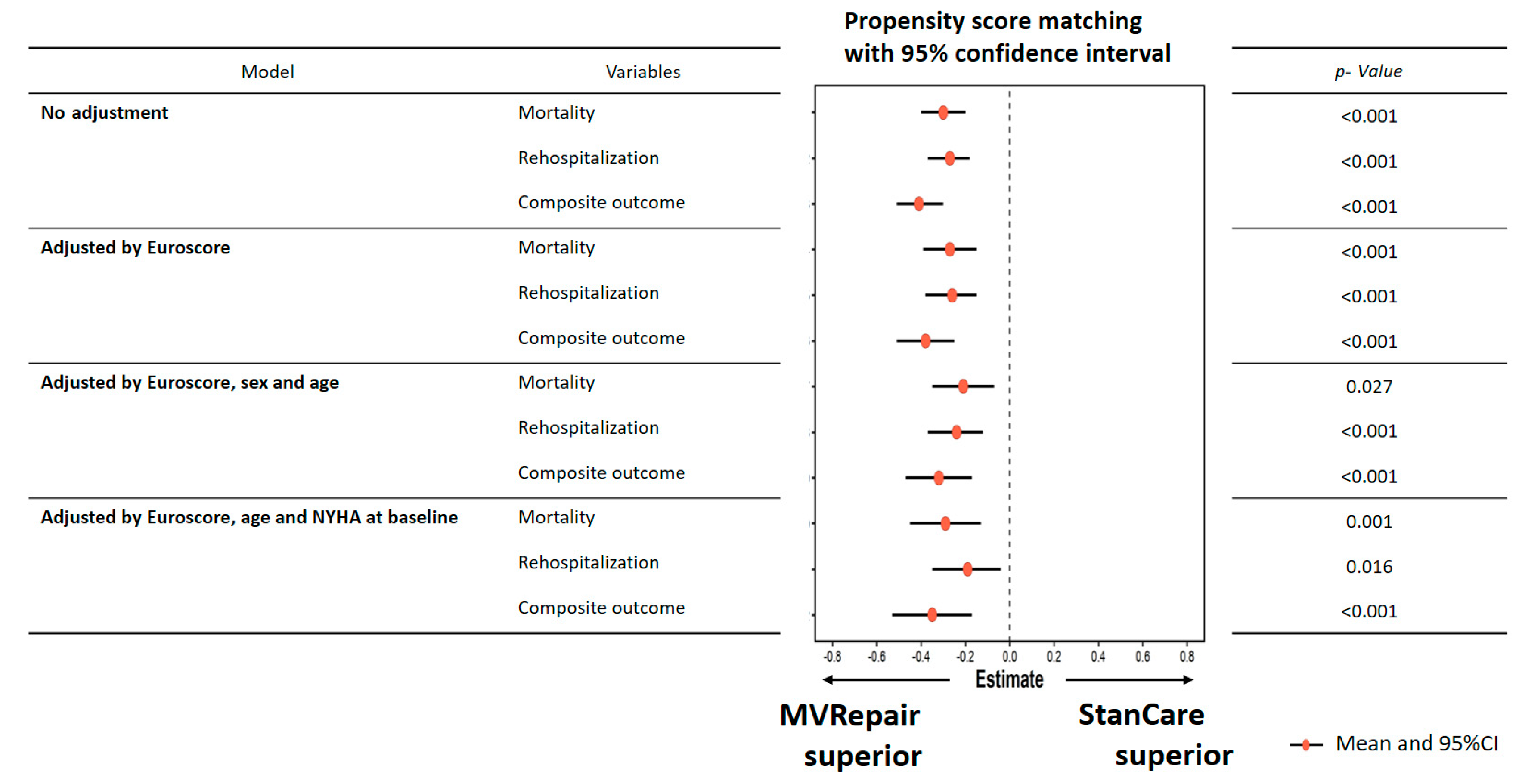
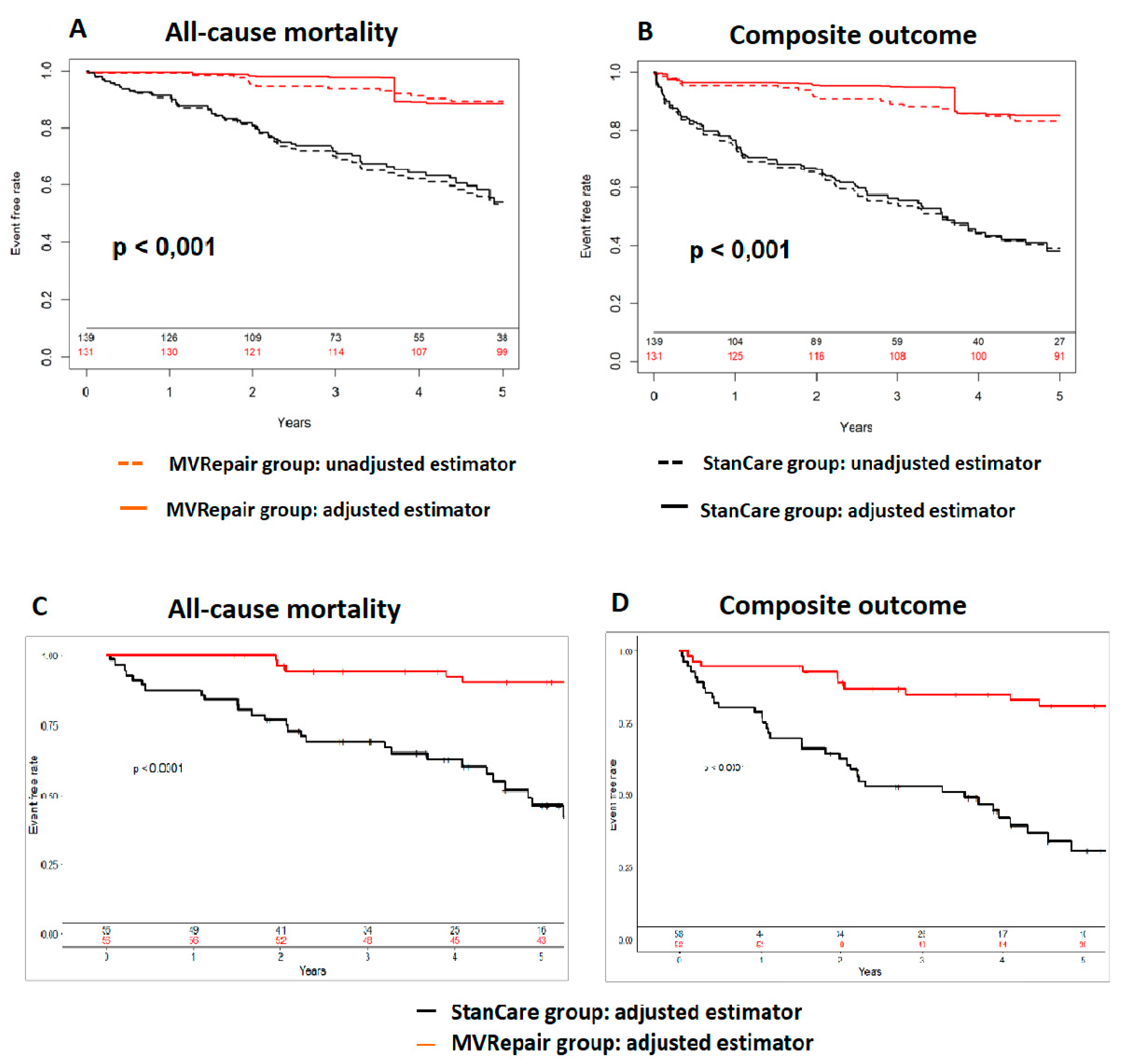
3.3. Long-Term Outcome
3.4. Predictors of Outcome
4. Discussion
4.1. Prevalence and Outcome of AFMR
4.2. Management of AFMR
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| AF | atrial fibrillation |
| AFMR | atrial functional mitral regurgitation |
| BMI | body mass index |
| COPD | chronic obstructive pulmonary disease |
| HFpEF | heart failure with preserved ejection fraction |
| LA | left atrium |
| LAD | left atrial diameter |
| LV | left ventricular |
| LVEDd | left ventricular end-diastolic diameter |
| LVEF | left ventricular ejection fraction |
| MR | mitral regurgitation |
| MV | mitral valve |
| MVRepair | mitral valve repair |
| NYHA | New York Heart Association |
| StanCare | standard of care |
| PAP | pulmonary artery pressure |
| TR | tricuspid regurgitation |
References
- Agrawal, A.; Naranjo, M.; Kanjanahattakij, N.; Rangaswami, J.; Gupta, S. Cardiorenal syndrome in heart failure with preserved ejection fraction—An under-recognized clinical entity. Heart Fail. Rev. 2019, 24, 421–437. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, H. The 2017 ESC/EACTS guidelines on the management of valvular heart disease. Wiener Klinische Wochenschrift 2018, 130, 168–171. [Google Scholar] [CrossRef] [PubMed]
- Casselman, F.P.; Van Slycke, S.; Wellens, F.; De Geest, R.; Degrieck, I.; Van Praet, F.; Vermeulen, Y.; Vanermen, H. Mitral Valve Surgery Can Now Routinely Be Performed Endoscopically. Circulation 2003, 108, 48–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chugh, S.S.; Havmoeller, R.; Narayanan, K.; Singh, D.; Rienstra, M.; Benjamin, E.J.; Gillum, R.F.; Kim, Y.-H.; McAnulty, J.H.; Zheng, Z.-J.; et al. Worldwide Epidemiology of Atrial Fibrillation: A Global Burden of Disease 2010 Study. Circulation 2014, 129, 837–847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deferm, S.; Bertrand, P.B.; Verbrugge, F.H.; Verhaert, D.; Rega, F.; Thomas, J.D.; Vandervoort, P.M. Atrial Functional Mitral Regurgitation: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2019, 73, 2465–2476. [Google Scholar] [CrossRef]
- Dunlay, S.M.; Roger, V.L.; Redfield, M.M. Epidemiology of heart failure with preserved ejection fraction. Nat. Rev. Cardiol. 2017, 14, 591–602. [Google Scholar] [CrossRef]
- Dziadzko, V.; Dziadzko, M.; Medina-Inojosa, J.R.; Benfari, G.; Michelena, H.I.; Crestanello, J.A.; Maalouf, J.; Thapa, P.; Enriquez-Sarano, M. Causes and mechanisms of isolated mitral regurgitation in the community: Clinical context and outcome. Eur. Heart J. 2019, 40, 2194–2202. [Google Scholar] [CrossRef]
- Grayburn, P.A.; Sanino, A.; Packer, M. Proportionate and Disproportionate Functional Mitral Regurgitation: A New Conceptual Framework That Reconciles the Results of the MITRA-FR and COAPT Trials. JACC Cardiovasc. Imaging 2019, 12, 353–362. [Google Scholar] [CrossRef]
- Ito, K.; Abe, Y.; Takahashi, Y.; Shimada, Y.; Fukumoto, H.; Matsumura, Y.; Naruko, T.; Shibata, T.; Yoshiyama, M.; Yoshikawa, J. Mechanism of atrial functional mitral regurgitation in patients with atrial fibrillation: A study using three-dimensional transesophageal echocardiography. J. Cardiol. 2017, 70, 584–590. [Google Scholar] [CrossRef] [Green Version]
- Kagiyama, N.; Hayashida, A.; Toki, M.; Fukuda, S.; Ohara, M.; Hirohata, A.; Yamamoto, K.; Isobe, M.; Yoshida, K. Insufficient Leaflet Remodeling in Patients with Atrial Fibrillation: Association With the Severity of Mitral Regurgitation. Circ. Cardiovasc. Imaging 2017, 10, e005451. [Google Scholar] [CrossRef] [Green Version]
- Kagiyama, N.; Mondillo, S.; Yoshida, K.; Mandoli, G.E.; Cameli, M. Subtypes of Atrial Functional Mitral Regurgitation: Imaging Insights into Their Mechanisms and Therapeutic Implications. JACC Cardiovasc. Imaging 2019, 13, 820–835. [Google Scholar] [CrossRef] [PubMed]
- Kajimoto, K.; Minami, Y.; Otsubo, S.; Sato, N.; Investigators of the Acute Decompensated Heart Failure Syndromes (ATTEND) registry. Ischemic or Nonischemic Functional Mitral Regurgitation and Outcomes in Patients with Acute Decompensated Heart Failure with Preserved or Reduced Ejection Fraction. Am. J. Cardiol. 2017, 120, 809–816. [Google Scholar] [CrossRef] [PubMed]
- Kajimoto, K.; Sato, N.; Takano, T.; Investigators of the Acute Decompensated Heart Failure Syndromes (ATTEND) registry. Functional mitral regurgitation at discharge and outcomes in patients hospitalized for acute decompensated heart failure with a preserved or reduced ejection fraction. Eur. J. Heart Fail. 2016, 18, 1051–1059. [Google Scholar] [CrossRef] [Green Version]
- Kihara, T.; Gillinov, A.M.; Tasaki, K.; Fukuda, S.; Song, J.-M.; Shiota, M.; Shiota, T. Mitral Regurgitation Associated with Mitral Annular Dilation in Patients with Lone Atrial Fibrillation: An Echocardiographic Study. Echocardiography 2009, 26, 885–889. [Google Scholar] [CrossRef]
- Kim, D.-H.; Heo, R.; Handschumacher, M.D.; Lee, S.; Choi, Y.-S.; Kim, K.-R.; Shin, Y.; Park, H.-K.; Bischoff, J.; Aikawa, E.; et al. Mitral Valve Adaptation to Isolated Annular Dilation: Insights into the Mechanism of Atrial Functional Mitral Regurgitation. JACC Cardiovasc. Imaging 2019, 12, 665–677. [Google Scholar] [CrossRef] [PubMed]
- Nishino, S.; Watanabe, N.; Ashikaga, K.; Morihisa, K.; Kuriyama, N.; Asada, Y.; Shibata, Y. Reverse Remodeling of the Mitral Valve Complex After Radiofrequency Catheter Ablation for Atrial Fibrillation: A Serial 3-Dimensional Echocardiographic Study. Circ. Cardiovasc. Imaging 2019, 12, e009317. [Google Scholar] [CrossRef]
- Penicka, M.; Kotrc, M.; Ondrus, T.; Mo, Y.; Casselman, F.P.; Vanderheyden, M.; Van Camp, G.; Van Praet, F.; Bartunek, J. Minimally invasive mitral valve annuloplasty confers a long-term survival benefit compared with state-of-the-art treatment in heart failure with functional mitral regurgitation. Int. J. Cardiol. 2017, 244, 235–241. [Google Scholar] [CrossRef]
- Reddy, Y.N.V.; Carter, R.E.; Obokata, M.; Redfield, M.M.; Borlaug, B.A. A Simple, Evidence-Based Approach to Help Guide Diagnosis of Heart Failure with Preserved Ejection Fraction. Circulation 2018, 138, 861–870. [Google Scholar] [CrossRef]
- Ring, L.; Dutka, D.P.; Wells, F.C.; Fynn, S.P.; Shapiro, L.M.; Rana, B.S. Mechanisms of atrial mitral regurgitation: Insights using 3D transoesophageal echo. Eur. Heart J. Cardiovasc. Imaging 2013, 15, 500–508. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, Y.; Abe, Y.; Sasaki, Y.; Bito, Y.; Morisaki, A.; Nishimura, S.; Shibata, T. Mitral valve repair for atrial functional mitral regurgitation in patients with chronic atrial fibrillation. Interact. Cardiovasc. Thorac. Surg. 2015, 21, 163–168. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, Y.; Abe, Y.; Takashi, M.; Fujii, H.; Morisaki, A.; Nishimura, S.; Sakon, Y.; Ito, K.; Shintani, A.; Shibata, T. Mid-term results of valve repairs for atrial functional mitral and tricuspid regurgitations. Gen. Thorac. Cardiovasc. Surg. 2019, 68, 467–476. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | MVRepair n = 131 | StanCare n = 139 | p |
|---|---|---|---|
| Age, y | 71.99 (7.26) | 77.71 (8.92) | <0.001 |
| Gender, n (%) | 28 (21.4) | 39 (28.1) | 0.259 |
| Hypertension, n (%) | 75 (60.5) | 90 (64.7) | 0.558 |
| Diabetes mellitus, n (%) | 1 (0.8) | 13 (9.5) | 0.003 |
| COPD, n (%) | 13 (10.0) | 22 (15.8) | 0.216 |
| MDRD < 50 mL /min/1.73 m2, n (%) | 29 (22) | 46 (33) | 0.057 |
| Stroke, n (%) | 3 (2.3) | 16 (11.5) | 0.007 |
| EuroSCORE II, % | 2 (1) | 3 (2) | <0.001 |
| History of AF, n (%) | 122 (93.1) | 133 (95.7) | 0.516 |
| NYHA, n (%) I, II III, IV | 38 (29.0) 93 (71.0) | 0 139 (100) | Not applicable |
| Body mass index, kg/m2 | 27.44 (4.30) | 29.00 (7.48) | 0.040 |
| H2FPEF | 6.34 (1.14) | 6.79 (1.27) | 0.003 |
| LVEDd, mm | 49.80 (6.44) | 48.48 (5.95) | 0.093 |
| LVEF, % | 59.05 (5.55) | 55.94 (4.13) | <0.001 |
| LA diameter, mm | 47.16 (7.10) | 44.10 (5.96) | <0.001 |
| AFMR ≤2/4 3/4, 4/4 | 39 (30%) 92 (70%) | 133 (96%) 6 (4%) | <0.001 |
| Tricuspid regurgitation | 2.14 (1.03) | 1.68 (0.94) | <0.001 |
| Systolic PAP, mmHg | 42.04 (10.52) | 44.22 (13.62) | 0.150 |
| Multivariable Analysis | ||
|---|---|---|
| HR (95% CI) | p-Value | |
| All-cause mortality | ||
| Age | 1.05 (1.01–1.10) | 0.031 |
| Body mass index | 0.93 (0.87–0.99) | 0.023 |
| MV repair | 0.16 (0.07–0.34) | <0.001 |
| HFpEF readmissions | ||
| Diabetes mellitus | 5.14 (1.16–22.73) | 0.031 |
| TR grade | 2.14 (1.00–4.58) | 0.050 |
| MV repair | 0.21 (0.09–0.51) | <0.001 |
| Mortality and HFpEF readmissions | ||
| Age | 1.03 (1.00–1.07) | 0.050 |
| MV repair | 0.22 (0.13–0.41) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balogh, Z.; Mizukami, T.; Bartunek, J.; Collet, C.; Beles, M.; Albano, M.; Katbeh, A.; Casselman, F.; Vanderheyden, M.; Van Camp, G.; et al. Mitral Valve Repair of Atrial Functional Mitral Regurgitation in Heart Failure with Preserved Ejection Fraction. J. Clin. Med. 2020, 9, 3432. https://doi.org/10.3390/jcm9113432
Balogh Z, Mizukami T, Bartunek J, Collet C, Beles M, Albano M, Katbeh A, Casselman F, Vanderheyden M, Van Camp G, et al. Mitral Valve Repair of Atrial Functional Mitral Regurgitation in Heart Failure with Preserved Ejection Fraction. Journal of Clinical Medicine. 2020; 9(11):3432. https://doi.org/10.3390/jcm9113432
Chicago/Turabian StyleBalogh, Zsuzsanna, Takuya Mizukami, Jozef Bartunek, Carlos Collet, Monika Beles, Marzia Albano, Asim Katbeh, Filip Casselman, Marc Vanderheyden, Guy Van Camp, and et al. 2020. "Mitral Valve Repair of Atrial Functional Mitral Regurgitation in Heart Failure with Preserved Ejection Fraction" Journal of Clinical Medicine 9, no. 11: 3432. https://doi.org/10.3390/jcm9113432