
Effects of Composite Attachments on Orthodontic Clear Aligners Therapy: A Systematic Review

 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol
2.2. Research Strategy and Information Sources
2.3. Selection of Studies
- Studies involving the presence of composite attachments in orthodontic therapy with clear aligners;
- Clinical studies on humans with a control group without attachments and/or a comparison between different configurations of composite attachments.
- Studies that do not relate to the topic or are related but have a different purpose;
- Clinical studies on humans without a control group and without a comparison between different configurations of attachments;
- Case reports, experimental studies that do not include humans, posters, books.
2.4. Data Extraction Process
2.5. Assessment of Risk of Bias
2.6. Data Analysis
3. Results
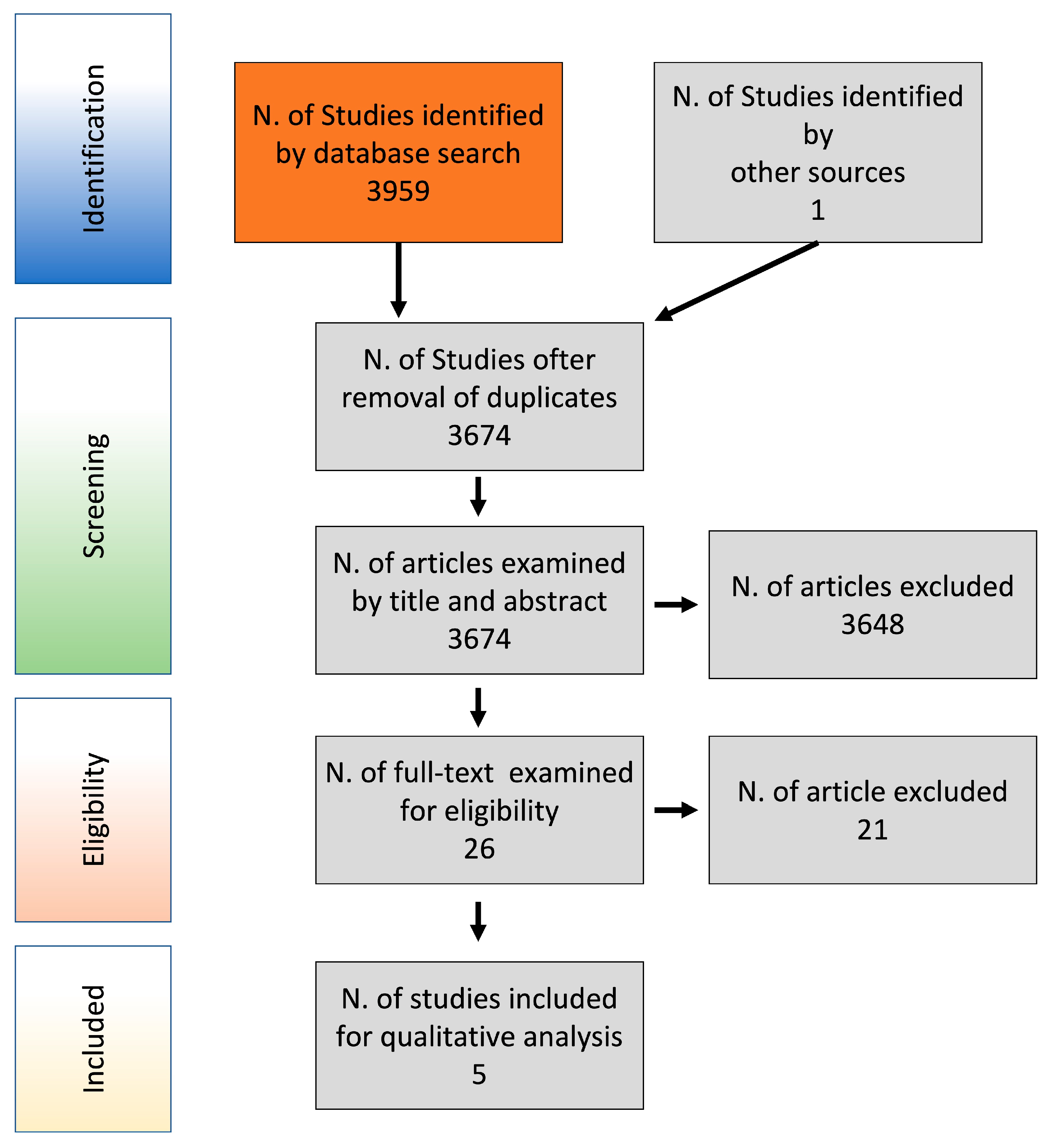
3.1. Search Results and Articles Selection
3.2. Study Characteristics
3.3. Risk of Bias Assessment
3.4. Analysis of the Results
4. Discussion
5. Conclusions
- The anterior root torque can be improved by the use of auxiliary elements, such as power ridges and attachments. However, they may be insufficient to ensure a right root control. Posterior anchorage seems important to ensure a greater control during anterior teeth retraction. It can be improved by adding attachments on a greater number of teeth [from canine to second molar].
- The evidence of the influence of attachments on intrusion and extrusion is lacking, although attachments seem to improve intrusion. No clinical studies evaluated posterior bucco-lingual tipping/expansion.
- Conflicting results were found about the ability of attachments to improve tooth rotation control. The majority of the studies showed a positive influence of attachments on derotation movement, although not statistically significant. The use of two attachments on the buccal and palatal side or the addition of attachments on adjacent teeth do not seem to improve rotation. Larger attachments with sharper edges showed better outcomes. However, several factors seemed to influence derotation effectiveness.
- The results have shown that the use of attachments could increase the molar mesio-distal movement efficacy. However, this improvement may not be clinically significant. Posterior anchorage can be improved by increasing the number of attachments bonded on the posterior teeth and optimized and rectangular horizontal attachments have shown the best results.
- Further clinical studies will be necessary to confirm all the above reported findings and to increase knowledge about the influence of attachments on different types of movement.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McCance, A.; Giovannoni, R.; Maspero, C.; Periti, G.; Toma, L.; Farronato, G. Un approccio estetico alla gestione del paziente ortodontico: Il sistema Clearstep. Mondo Ortod. 2010, 35, 77–86. [Google Scholar] [CrossRef]
- Savignano, R.; Barone, S.; Paoli, A.; Razionale, A. FEM analysis of bone-ligaments-tooth models for biomechanical simulation of individual orthodontic devices. In Proceedings of the ASME 2014 International Design Engineering Technical Conferences & Computers and Information in Engineering Conference, Buffalo, NY, USA, 17–20 August 2014. [Google Scholar]
- Comba, B.; Parrini, S.; Rossini, G.; Castroflorio, T.; Deregibus, A. A three-dimensional finite element analysis of upper-canine distalization with clear aligners, composite attachments, and class II elastics. J. Clin. Orthod. 2017, 51, 24–28. [Google Scholar] [PubMed]
- Momtaz, P. The Effect of Attachment Placement and Location on Rotational Control of Conical Teeth Using Clear Aligner Therapy. Master’s Thesis, University of Nevada, Las Vegas, NV, USA, 2016. [Google Scholar]
- Boyd, R. Three-dimensional diagnosis and orthodontic treatment of complex malocclusions with the invisalign appliance. In Seminars in Orthodontics; W.B. Saunders: Philadelphia, PA, USA, 2001. [Google Scholar]
- Boyd, R.; Miller, R.; Vlaskalic, V. The invisalign system in adult orthodontics: Mild crowding and space closure cases. J. Clin. Orthod. 2000, 34, 203–212. [Google Scholar]
- Womack, W.; Ahn, J.; Ammari, Z.; Castillo, A. A new approach to correction of crowding. Am. J. Orthod. Dentofac. Orthop. 2002, 122, 310–316. [Google Scholar] [CrossRef]
- Joffe, L. Current products and practice. Invisalign: Early experiences. J. Orthod. 2003, 30, 348–352. [Google Scholar] [CrossRef] [PubMed]
- Kravitz, N.; Kusnoto, B.; BeGole, E.; Obrez, A.; Agran, B. How well does Invisalign work? A prospective clinical study evaluating the efficacy of teeth movement with Invisalign. Am. J. Orthod. Dentofac. Orthop. 2009, 135, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Drake, C.; McGorray, S.; Dolce, C.; Nair, M.; Wheeler, T. Orthodontic tooth movement with clear aligners. ISRN Dent. 2012, 2012, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tuncay, O. The invisalign system. In Orthodontic Review, 2nd ed.; Mosby: St. Louis, MO, USA, 2014. [Google Scholar]
- Castroflorio, T.; Debernardi, C. Upper-incisor root control with invisalign appliances. J. Clin. Orthod. 2013, 47, 346–351. [Google Scholar]
- Rossini, G.; Parrini, S.; Deregibus, A.; Castroflorio, T. Controlling orthodontic tooth movement with clear aligners—An updated systematic review regarding efficacy and efficiency. J. Aligner Orthod. 2017, 1, 7–20. [Google Scholar]
- Rossini, G.; Parrini, S.; Castroflorio, T.; Deregibus, A.; Debernardi, C. Efficacy of Clear Aligners in controlling orthodontic tooth movement—A systematic review. Angle Orthod. 2015, 85, 881–889. [Google Scholar] [CrossRef] [Green Version]
- Papadimitriou, A.; Mousoulea, S.; Gkantidis, N.; Kloukos, D. Clinical effectiveness of Invisalign orthodontic treatment—A systematic review. Prog. Orthod. 2018, 19, 1–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garino, F.; Castroflorio, T.; Daher, S.; Ravera, S.; Rossini, G.; Cugliari, G.; Deregibus, A. Effectiveness of composite attachments in controlling upper-molar movement with aligners. J. Clin. Orthod. 2016, 50, 341–347. [Google Scholar] [PubMed]
- Higgins, J.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions—Version 5.1.0. 2011. Available online: https://handbook-5-1.cochrane.org/ (accessed on 20 December 2019).
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P). Syst. Rev. 2015, 4, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Downs, S.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durrett, S. Efficacy of Composite Tooth Attachments in Conjunction with the Invisalign Tm System Using Three-Dimensional Digital Technology. Master’s. Thesis, University of Florida, Gainesville, FL, USA, 2004. [Google Scholar]
- Simon, M.; Keilig, L.; Schwarze, J.; Jung, B.; Bourauel, C. Treatment outcome and efficacy of an aligner technique—Regarding incisor torque, premolar derotation and molar distalization. BMC Oral Health 2014, 14, 68. [Google Scholar] [CrossRef] [Green Version]
- Kravitz, N.; Kusnoto, B.; Agran, B.; Viana, G. Influence of attachments and interproximal reduction on the accuracy of canine rotation with Invisalign. Angle Orthod. 2008, 78, 682–687. [Google Scholar] [CrossRef] [Green Version]
- Dai, F.; Xu, T.; Shu, G. Comparison of achieved and predicted tooth movement of maxillary first molars and central incisors: First premolar extraction treatment with Invisalign. Angle Orthod. 2019, 89, 679–687. [Google Scholar] [CrossRef]
- Pavoni, C.; Lione, R.; Laganà, G.; Cozza, P. Self-ligating versus invisalign Analysis of dentoalveolar effects. Ann. Stomatol. 2011, 2, 23–27. [Google Scholar]
- Lombardo, L.; Arreghini, A.; Ramina, F.; Ghislanzoni, L.H.; Siciliani, G. Predictability of orthodontic movement with orthodontic aligners: A retrospective study. Prog. Orthod. 2017, 18, 35–46. [Google Scholar] [CrossRef] [Green Version]
- Hahn, W.; Zapf, A.; Dathe, H.; Fialka-Fricke, J.; Friche-Zech, S.; Gruber, R.; Kubein-Meesenburg, D.; Sadat-Khonsari, R. Torquing an upper central incisor with aligners—Acting forces and biomechanical principles. Eur. J. Orthod. 2010, 32, 607–613. [Google Scholar] [CrossRef] [Green Version]
- Brezniak, N. The clear plastic appliance—A biomechanical point of view. Angle Orthod. 2008, 78, 381–382. [Google Scholar] [CrossRef] [Green Version]
- Elkholy, F.; Panchaphongsaphak, T.; Kilic, F.; Schmidt, F.; Lapatki, B. Forces and moments delivered by PET-G aligners to an upper central incisor for labial and palatal translation. J. Orofac. Orthop. 2015, 76, 460–475. [Google Scholar] [CrossRef] [PubMed]
- Houle, J.; Piedade, L.; Todescan, R., Jr.; Pinheiro, F. The predictability of transverse changes with Invisalign. Angle Orthod. 2017, 87, 19–24. [Google Scholar] [CrossRef] [Green Version]
- Khosravi, R.; Cohanim, B.; Hujoel, P.; Daher, S.; Neal, M.; Liu, W.; Huang, G. Management of overbite with the Invisalign appliance. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 691–699.e2. [Google Scholar] [CrossRef] [PubMed]
- Vardimon, A.; Robbins, D.; Brosh, T. In-vivo von Mises strains during Invisalign treatment. Am. J. Orthod. Dentofac. Orthop. 2010, 138, 399–409. [Google Scholar] [CrossRef]
- Weir, T. Clear aligners in orthodontic treatment. Aust. Dent. J. 2017, 61, 58–62. [Google Scholar] [CrossRef] [Green Version]
- Boyd, R.L. Esthetic orthodontic treatment using the invisalign appliance for moderate to complex malocclusions. J. Dent. Educ. 2008, 72, 948–967. [Google Scholar] [CrossRef]
- Liu, Y.; Hu, W. Force changes associated with different intrusion strategies for deep-bite correction by clear aligners. Angle Orthod. 2018, 88, 771–778. [Google Scholar] [CrossRef] [Green Version]
- Savignano, R.; Valentino, R.; Razionale, A.; Michelotti, A.; Barone, S.; D’Antò, V. Biomechanical effects of different auxiliary-aligner designs for the extrusion of an upper central incisor: A finite element analysis. J. Healthc. Eng. 2019, 2019, 9687127. [Google Scholar] [CrossRef] [Green Version]
- Simon, M.; Keilig, L.; Schwarze, J.; Jung, B.; Bourauel, C. Forces and moments generated by removable thermoplastic aligners: Incisor torque, premolar derotation, and molar distalization. Am. J. Orthod. Dentofac. Orthop. 2014, 145, 728–735. [Google Scholar] [CrossRef]
- Cortona, A.; Rossini, G.; Parrini, S.; Deregibus, A.; Castroflorio, T. Clear aligner orthodontic therapy of rotated mandibular round-shaped teeth. A finite element study. Angle Orthod. 2020, 90, 247–254. [Google Scholar] [CrossRef] [Green Version]
- Elkholy, F.; Mikhaiel, B.; Repky, S.; Schmidt, F.; Lapatki, B. Effect of different attachment geometries on the mechanical load exerted by PET-G aligners during derotation of mandibular canines: An in vitro study. J. Orofac. Orthop. 2019, 80, 315–326. [Google Scholar] [CrossRef]
- Barone, S.; Paoli, A.; Razionale, A.; Savignano, R. Computer aided modelling to simulate the biomechanical behaviour of customised orthodontic removable appliances. Int. J. Interact. Des. Manuf. 2014, 10, 387–400. [Google Scholar] [CrossRef]
- Bollen, A.; Huang, G.; King, G.; Hujoel, P.; Ma, T. Activation time and material stiffness of sequential removable orthodontic appliances. Part 1: Ability to complete treatment. Am. J. Orthod. Dentofac. Orthop. 2003, 124, 496–501. [Google Scholar] [CrossRef]
- Baldwin, D.; King, G.; Ramsay, D.; Huang, G.; Bollen, A. Activation time and material stiffness of sequential removable orthodontic appliances. Part 3: Premolar extraction patients. Am. J. Orthod. Dentofac. Orthop. 2008, 133, 837–845. [Google Scholar] [CrossRef]
- Nucera, R.; Giudice, A.L.; Rustico, L.; Matarese, G.; Papadopoulos, M.; Cordassco, G. Effectiveness of orthodontic treatment with functional appliances on maxillary growth in the short term. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 600–611.e3. [Google Scholar]
- Cordasco, G.; Giudice, A.L.; Militi, A.; Nucera, R.; Triolo, G.; Matarese, G. In vitro evaluation of resistance to sliding in self-ligating and conventional bracket systems during dental alignment. Korean J. Orthod. 2012, 42, 218–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ravera, S.; Castroflorio, T.; Garino, F.; Daher, S.; Cugliari, G.; Deregibus, A. Maxillary molar distalization with aligners in adult patients—A multicenter retrospective study. Prog. Orthod. 2016, 17, 12–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, N.; Lei, X.; Yang, X.; Li, X.; Ge, Z. Three-dimensional Finite Element Analysis on Canine Teeth Distalization by Different Accessories of Bracket-free Invisible Orthodontics Technology. In AIP Conference Proceedings; AIP Publishing LLC: Melville, NY, USA, 2018. [Google Scholar]
- Gomez, J.; Pena, F.; Martinez, V.; Giraldo, D.; Cardona, C. Initial force systems during bodily tooth movement with plastic aligners and composite attachments—A three-dimensional finite element analysis. Angle Orthod. 2015, 85, 454–460. [Google Scholar] [PubMed]
- Yokoi, Y.; Arai, A.; Kawamura, J.; Uozumi, T.; Usui, Y.; Okafuji, N. Effects of Attachment of Plastic Aligner in Closing of Diastema of Maxillary Dentition by Finite Element Method. J. Healthc. Eng. 2019, 2019, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Ackley, B.J.; Swan, B.A.; Ladwig, G.; Tucker, S. Evidence-Based Nursing Care Guidelines: Medical-Surgical Interventions; Mosby Elsevier: St. Louis, MO, USA, 2008; p. 7. [Google Scholar]
- Nucera, R.; Lo Giudice, A.; Matarese, G.; Artemisia, A.; Bramanti, E.; Crupi, P.; Cordasco, G. Analysis of the characteristics of slot design affecting resistance to sliding during active archwire configurations. Prog. Orthod. 2013, 14, 35. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Database of Published Trials | Search Strategy Used | Hits |
|---|---|---|
| MEDLINE searched via Pubmed Searched on 22 March 2020 via https://www.ncbi.nlm.nih.gov/pubmed/ | (((((((((orthodontic*) OR treatment*) OR therapy) OR therapies) OR appliance*) OR device*)) AND (((((attachment*) OR accessory) OR accessories) OR auxiliary) OR auxiliaries)) AND ((((((((aligner*) OR Invisalign) OR thermoplastic) OR transparent) OR clear) OR invisible) OR thermoform*) OR removable)) | 1822 |
| COCHRANE Database of Systematic Reviews searched via The Cochrane Library Searched on 22 March 2020 via https://www.cochranelibrary.com/ | ((orthodontic*) OR (treatment*) OR (therapy) OR (therapies) OR (appliance*) OR (device*)) AND ((aligner*) OR (Invisalign) OR (thermoplastic) OR (thermoform*) OR (transparent) OR (invisible)) AND ((attachment*) OR (accessory) OR (accessories) OR (auxiliary) OR (auxiliaries)) | 666 |
| COCHRANE Central Register of Controlled Trials searched via The Cochrane Library Searched on 22 March 2020 via https://www.cochranelibrary.com/ | ((orthodontic*) OR (treatment*) OR (therapy) OR (therapies) OR (appliance*) OR (device*)) AND ((aligner*) OR (Invisalign) OR (thermoplastic) OR (thermoform*) OR (transparent) OR (invisible)) AND ((attachment*) OR (accessory) OR (accessories) OR (auxiliary) OR (auxiliaries)) | 34 |
| WEB OF SCIENCE Searched on 22 March 2020 via https://www.webofknowledge.com/ | (((((((((orthodontic*) OR treatment*) OR therapy) OR therapies) OR appliance*) OR device*)) AND ((((((aligner*) OR Invisalign) OR thermoplastic) OR thermoform*) OR transparent) OR invisible)) AND (((((attachment*) OR accessory) OR accessories) OR auxiliary) OR auxiliaries)) | 344 |
| LILACS Searched on 22 March 2020 via http://lilacs.bvsalud.org/ | (tw:(aligner OR Invisalign OR thermoplastic OR thermoformed OR transparent OR invisible)) AND (tw:(attachment OR accessory OR accessories OR auxiliary OR auxiliaries)) | 7 |
| EMBASE Searched on 10 January 2020 via https://www.embase.com/ | (orthodontic* OR treatment* OR ‘therapy’/exp OR therapy OR therapies OR appliance* OR device*) AND (aligner* OR Invisalign OR ‘thermoplastic’/exp OR thermoplastic OR thermoform* OR transparent OR invisible) AND (attachment* OR accessory OR accessories OR auxiliary OR auxiliaries) | 269 |
| CLINICALTRIALS.GOV Searched on 22 March 2020 via https://clinicaltrials.gov/ | (aligner OR Invisalign OR thermoplastic OR thermoformed OR transparent OR invisible) AND (attachment OR accessory OR accessories OR auxiliary OR auxiliaries) | 43 |
| PROQUEST Searched on 10 January 2020 via https://www.proquest.com/ | (aligner OR Invisalign OR thermoplastic OR thermoformed OR transparent OR invisible) AND (attachment OR accessory OR accessories OR auxiliary OR auxiliaries) AND Orthodontic* | 774 |
| TOTAL | 3959 | |
| Study | Type of Study | Setting | Analyzed Sample | Auxiliary Elements | Analysis Methods | Performed Movements | Duration of Treatment | Outcome |
|---|---|---|---|---|---|---|---|---|
| Dai et al. [23] | Case Series | The Second Dental Center, Peking University School and Hospital of Stomatology | 30 patients (4 M–26 F) Age: 19.4 ± 6.3 First premolar extraction cases treated with Invisalign. Three variables considered: -Age -Type of attachment -Initial crowding | On first molar: -Vertical attachment (3mm) -Horizontal attachment (3mm) -Horizontal attachment (5mm) -G6 optimized attachment | Superimposition of: -Real and virtual pre-treatment models -Real pre- and post-treatment models -Virtual pre- and post-treatment models -All four models | On first molar: -M-D TIPPING -M-D TRANSLATION -O-G TRANSLATION On central incisor: -TORQUE -V-L TRANSLATION -O-G TRANSLATION | 22.3 ± 4.6 months Aligner change every 1–2 weeks | - Difference between predicted and achieved tooth movement in maxillary first molar and central incisor -Influence of age, initial crowding and type of attachment |
| Durrett [20] | RCT | University of Florida Orthodontic Research clinic | 99 patients reduced to 86 Age: 18+ 6 configurations: -5 groups with different attachments -1 control group (without attachments) 2 groups: -Extraction and non-extraction cases | -No attachments (Group C) -Attachments with different shapes on the buccal surface (Groups A-B-D-F) -Attachments bonded to both buccal and lingual surfaces (Group E) | Superimposition of: initial models and final models or first reboot | -ROTATION of canine and premolar -INTRUSION and EXTRUSION of incisor, canine and premolar | Minimum 2 years Aligner change every 2 weeks | -ROTATION: Comparison between predicted and achieved tooth movement in reboot and non-reboot cases -INTRUSION and EXTRUSION: Comparison between predicted and achieved tooth movement in reboot cases |
| Garino et al. [16] | RCT | Orthodontic clinics in Turin and Vancouver Collections of the AAO Foundation Craniofacial Growth Legacy | 30 patients with class II malocclusion (12 M–18 F) Age: 30.5 3 configurations: -Group C1—5 attachments per quadrant -Group C2—3 attachments per quadrant -Group C—Control | Vertical rectangular attachments -Group C1—From maxillary canine to second molar -Group C2—From maxillary first premolar to first molar Class II elastics in the first phase Power ridge in the second phase | Superimposition of T0 and T1 cephalograms | -Maxillary molars DISTALIZATION -Incisors RETRACTION | Average time:24.3 months Aligner change every 2 weeks | Comparison of the position of upper molars and central incisors between T0 and T1 (angular, horizontal and vertical measurements expressed as angles and distances from y-axis, x-axis and occlusal plane). |
| Kravitz et al. [22] | Prospective CCT | Department of Orthodontics—University of Illinois-Chicago | 38 pazients reduced to 31 (13 M–18 F) Average age: 29.4 3 configurations: -Attachment only group (AO) -Interproximal-reduction only group (IO) -Group without attachments (N) | Attachemnt Only group: -Vertical or horizontal ellipsoid attachments -Horizontal rectangular attachments | Superimposition of the final stage of the pre-treatment model (ClinCheck) and the post-treatment model | Maxillary and mandibular canine ROTATION | Average time:7.2 months Aligner change every 2–3 weeks | Comparison between the amount of rotation predicted and the amount of rotation actually achieved |
| Simon et al. [21] | Retrospective CCT | Private practice-Cologne (Germany) |
30 patients (11 M–19 F) reduced to 26. Age: 32.9 3 configurations: -Incisors with attachments or power-ridges -Premolars with or without attachments -Molars with or without attachments | Incisor TORQUE: -Horizontal ellipsoid attachment or power ridge Premolar DEROTATION: -Optimized Attachment or no attachment Molar DISTALIZATION: -Horizontal Attachment Bevelled in gingival direction or no attachment | -Superimposition between the initial situation (T1) and the final stage of ClinCheck (Clin T2) -Superimposition between the initial situation (T1) and the actual post-treatment condition (T2) | -Incisor TORQUE > 10° -Premolar DEROTATION > 10° -Molar DISTALIZATION > 1.5 mm | Number of aligners: 18 aligners on average | -Comparison between (T2-T1) and (ClinT2-T1) to evaluate treatment efficacy with or without attachments and power ridges - Analysis of the accuracy of premolar derotation according to the staging (degree of derotation per aligner) and to the total amount of predicted movement |
| Study | Reporting | External Validity | Bias | Confounding | Power | Overall | Risk of Bias * |
|---|---|---|---|---|---|---|---|
| 0–11 | 0–3 | 0–7 | 0–6 | 0–1 | 0–28 | ||
| Dai et al. [23] | 10 of 11 | 1 of 3 | 3 of 7 | 3 of 6 | 0 of 1 | 17 of 28 | Medium |
| Durrett [20] | 6 of 11 | 1 of 3 | 2 of 7 | 3 of 6 | 0 of 1 | 12 of 28 | Medium |
| Garino et al. [16] | 9 of 11 | 1 of 3 | 4 of 7 | 2 of 6 | 1 of 1 | 17 of 28 | Medium |
| Kravitz et al. [22] | 10 of 11 | 1 of 3 | 4 of 7 | 3 of 6 | 0 of 1 | 18 of 28 | Medium |
| Simon et al. [21] | 9 of 11 | 1 of 3 | 3 of 7 | 3 of 6 | 0 of 1 | 16 of 28 | Medium |
| Study | Type of Study | Aim | Study Design | Results | |
|---|---|---|---|---|---|
| Anterior B-L tipping/Root torque | Simon et al. [21] | Retrospective CCT | Verification of the effectiveness of the Invisalign treatment by comparing clin-check with the obtained results. Analysis of the influence of attachments and power-ridges, patient compliance and staging (amount of movement per aligner) on treatment efficacy. | 30 patients (11 M–19 F) reduced to 26. Age: 32.9 3 configurations: -Incisors with attachments or power-ridges -Premolars with or without attachments -Molars with or without attachments | Incisor torque showed positive results, both with an horizontal ellipsoid attachment on upper central incisors and with power ridges. A torque loss (up to 50%) is a common finding during incisors retraction. |
| Garino et al. [16] | RCT | Verification of the influence of the number of attachments on the amount of upper molar distalization | 30 patients with class II malocclusion (12 M–18 F) Age: 30.5 3 configurations: -Group C1—5 attachments per quadrant -Group C2—3 attachments per quadrant -Group C—Control | The greatest distalization of central incisors was obtained in C1 group. | |
| Dai et al. [23] | Case Series | Comparison between predicted and achieved tooth movements of maxillary first molars and central incisors in extraction cases treated with Invisalign. | 30 patients (4 M–26 F) Age: 19.4 ± 6.3 First premolar extraction cases treated with Invisalign. Three variables considered: - Age -Type of attachment -Initial crowding | In case of anchorage loss of posterior teeth, the amount of incisors bodily movement in lingual direction was lower than expected, while inclination increased in the same direction. In particular, 3 mm vertical rectangular attachment, located on the maxillary first molar, showed the least efficacy in anchorage control, compared to horizontal attachments (3 or 5 mm) and optimized G6 attachments. | |
| Intrusion | Durrett [20] | RCT | Analysis of the influence of attachments during: -canine and premolar rotation; -incisors, canines and premolars intrusion and extrusion. Comparison between different attachment configurations. | 99 patients reduced to 86 Age: 18+ 6 configurations: -5 groups with different attachments -1 control group (without attachments) 2 groups: -Extraction and non-extraction cases | All the attachment groups showed a greater efficiency compared to the control group. The greatest efficiency and degree of correlation was shown by group F, characterized by a vestibular attachment with a poliedric shape. |
| Dai et al. [23] | Case Series | Comparison between predicted and achieved tooth movement of maxillary first molars and central incisors in extraction cases treated with Invisalign. | 30 patients (4 M–26 F)Age: 19.4 ± 6.3First premolar extraction cases treated with Invisalign. Three variables considered:- Age- Type of attachment- Initial crowding | First molars achieved greater intrusion than predicted. The group with the optimized G6 attachments showed a greater difference between predicted and achieved tooth movement compared to the other groups. | |
| Extrusion | Durrett [20] | RCT | Analysis of the influence of attachments during: -canine and premolar rotation; -incisors, canines and premolars intrusion and extrusion. Comparison between different attachment configurations. | 99 patients reduced to 86 Age: 18+ 6 configurations: -5 groups with different attachments -1 control group (without attachments) 2 groups: -Extraction and non-extraction cases | No statistically significant differences were found among the analyzed groups The group with an ovoid attachment on the buccal face, showed the greatest efficiency. However, the small number of the sample didn’t allow to draw clear conclusions. |
| Rotation | Simon et al. [21] | Retrospective CCT | Verification of the effectiveness of the Invisalign treatment by comparing clin-check with the obtained results. Analysis of the influence of attachments and power-ridges, patient compliance and staging (amount of movement per aligner) on treatment efficacy. | 30 patients (11 M–19 F) reduced to 26. Age: 32.9 3 configurations: -Incisors with attachments or power-ridges -Premolars with or without attachments -Molars with or without attachments | No significant differences were found among the analyzed groups. The effectiveness was reduced for predicted rotations greater than 15° and for movements greater than 1.5° per aligner. |
| Kravitz et al. [22] | Prospective CCT | Evaluation of the influence of attachments or IPR on canine rotation (comparison between predicted and achieved results) | 38 pazients reduced to 31 (13 M–18 F) Age: 29.4 3 configurations: -Attachment only group (AO) -Interproximal-reduction only group (IO) -Group without attachments (N) | No significant differences were found between groups with and without attachments. The IO group performed better than the other ones, because it allowed the creation of space for movement. | |
| Durrett [20] | RCT | Analysis of the influence of attachments during: -canine and premolar rotation; -incisors, canines and premolars intrusion and extrusion. Comparison between different attachment configurations. | 99 patients reduced to 86 Age: 18+ 6 configurations: -5 groups with different attachments -1 control group (without attachments) 2 groups: -Extraction and non-extraction cases | Conflicting results were found between groups that required or not required a “reboot”. In the non-rebooted patients, group C (without attachments) achieved a greater degree of rotation than group F (with a vestibular attachment). In the rebooted patients, on the other hand, the attachment groups were more effective than the control one, except for the group with a vestibular and a lingual attachment. Larger attachments with sharper edges seem to be more effective. | |
| M-D Movement | Simon et al. [21] | Retrospective CCT | Verification of the effectiveness of the Invisalign treatment by comparing clin-check with the obtained results. Analysis of the influence of attachments and power-ridges, patient compliance and staging (amount of movement per aligner) on treatment efficacy. | 30 patients (11 M–19 F) reduced to 26. Age: 32.9 3 configurations: -Incisors with attachments or power-ridges -Premolars with or without attachments -Molars with or without attachments | Molar distalization was more effective than the other movements, regardless to the use of attachments (average accuracy of 88.4% for the attachment group and 86.9% for the group without attachments). |
| Dai et al. [23] | Case Series | Comparison between predicted and achieved tooth movements of maxillary first molars and central incisors in extraction cases treated with Invisalign. | 30 patients (4 M–26 F)Age: 19.4 ± 6.3 First premolar extraction cases treated with Invisalign. Three variables considered:- Age- Type of attachment- Initial crowding | The study highlighted a loss of posterior anchorage: the 3-mm vertical rectangular attachment showed the worst clinical outcome. On the other hand, the G6-optimized attachments and the horizontal rectangular ones seem to be more effective in counteracting mesial tipping. | |
| Garino et al. [16] | RCT | Verification of the influence of the number of attachments on the amount of upper molar distalization | 30 patients with class II malocclusion (12 M–18 F) Age: 30.5 3 configurations: -Group C1—5 attachments per quadrant -Group C2—3 attachments per quadrant -Group C—Control | The number of attachments seems to play play an important role: group C1 (with attachments bonded on the surface of five teeth) showed greater first molar distalization and central-incisor retraction, compared to the other groups. No significant differences were found regarding the efficacy of second molar distalization among the attachment groups. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nucera, R.; Dolci, C.; Bellocchio, A.M.; Costa, S.; Barbera, S.; Rustico, L.; Farronato, M.; Militi, A.; Portelli, M. Effects of Composite Attachments on Orthodontic Clear Aligners Therapy: A Systematic Review. Materials 2022, 15, 533. https://doi.org/10.3390/ma15020533
Nucera R, Dolci C, Bellocchio AM, Costa S, Barbera S, Rustico L, Farronato M, Militi A, Portelli M. Effects of Composite Attachments on Orthodontic Clear Aligners Therapy: A Systematic Review. Materials. 2022; 15(2):533. https://doi.org/10.3390/ma15020533
Chicago/Turabian StyleNucera, Riccardo, Carolina Dolci, Angela Mirea Bellocchio, Stefania Costa, Serena Barbera, Lorenzo Rustico, Marco Farronato, Angela Militi, and Marco Portelli. 2022. "Effects of Composite Attachments on Orthodontic Clear Aligners Therapy: A Systematic Review" Materials 15, no. 2: 533. https://doi.org/10.3390/ma15020533