Serum Iron Levels and Copper-to-Zinc Ratio in Sickle Cell Disease

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Site
2.2. Study Design, Subject Recruitment, and Data Collection
2.3. Laboratory Analysis
2.4. Data Analysis
2.5. Ethics Statement
3. Results
3.1. Demographic Characteristics of the Study Participants
3.2. Serum Levels of Iron, Copper and Zinc in the Study Participants
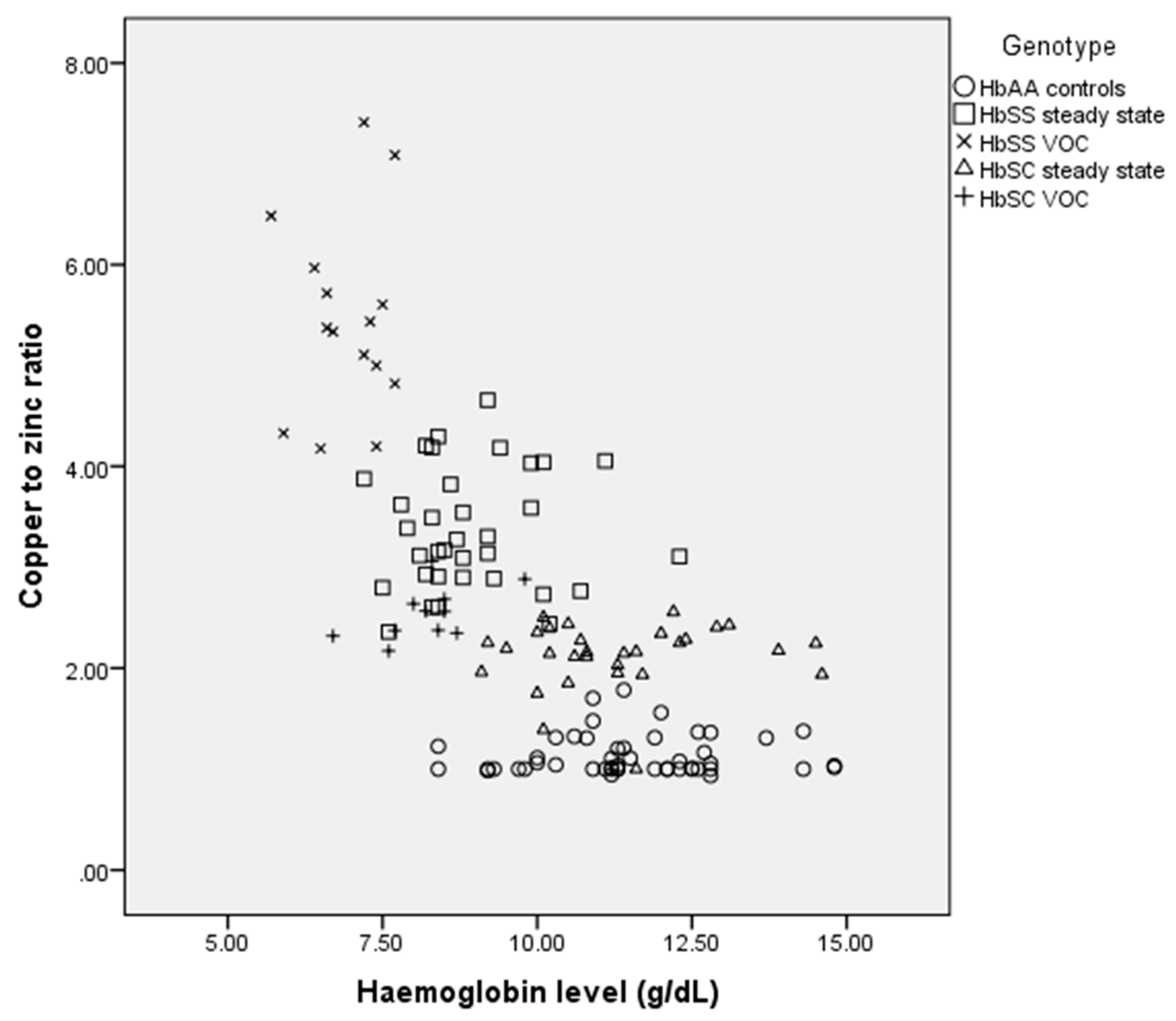
3.3. Correlation between Copper-to-Zinc Ratio and Haemoglobin Among the Study Participants
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Serjeant, G.R. Sickle-cell disease. Lancet 1997, 350, 725–730. [Google Scholar] [CrossRef]
- Amer, J.; Ghoti, H.; Rachmilewitz, E.; Koren, A.; Levin, A.; Fibach, E. Red blood cells, platelets and polymorphonuclear neutrophils of patients with sickle cell disease exhibit oxidative stress that can be ameliorated by antioxidants. Br. J. Haematol. 2006, 1321, 108–111. [Google Scholar] [CrossRef] [PubMed]
- Madigan, C.; Malik, P. Pathophysiology and therapy for haemoglobinopathies. Part I: Sickle cell disease. Expert Rev. Mol. Med. 2006, 8, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Ohene-Frempong, K.; Oduro, J.; Tetteh, H.; Nkrumah, F. Screening newborns for sickle cell disease in Ghana. Paediatrics 2008, 121, S120–S121. [Google Scholar] [CrossRef]
- Al-saqladi, A.W.M.; Cipolotti, R.; Fijnvandraat, K.; Brabin, B.J. Growth and nutritional status of children with homozygous sickle cell disease. Ann. Trop. Paediatr. 2008, 28, 165–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nur, E.; Biemond, B.J.; Otten, H.; Brandjes, D.P.; John-John, B.; Schnog, J.B. Oxidative stress in sickle cell disease; pathophysiology and potential implications for disease management. Am. J. Hematol. 2011, 86, 484–489. [Google Scholar] [CrossRef]
- Voskou, S.; Aslan, M.; Fanis, P.; Phylactides, M.; Kleanthous, M. Oxidative stress in the beta thalassemia and sickle cell disease. Redox Biol. 2015, 6, 226–239. [Google Scholar] [CrossRef]
- Vichinsky, E. Emerging “A” therapies in Hemoglobinopathies: Agonists, antogonists, antioxidants, and arginine. Hematology Am Soc Hematol Educ Program. 2012, 2012, 271–275. [Google Scholar] [PubMed]
- Prasad, A.S.; Schoomaker, E.B.; Ortega, J.; Brewer, G.J.; Oberleas, D.; Oelshlegel, F.J., Jr. Zinc deficiency in sickle cell disease. Clin. Chem. 1975, 21, 582–587. [Google Scholar]
- Prasad, A.S. Zinc deficiency in patients with sickle cell disease. Am. J. Clin. Nutr. 2002, 75, 181–182. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.C.; Chow, C. Interaction of antioxidants and their implication in generic anemia. Proc. Soc. Biol. Med. 1999, 222, 274–282. [Google Scholar] [CrossRef]
- Guo, C.H.; Chen, P.C.; Yeh, M.S.; Hsiung, D.Y.; Wang, C.L. Cu/Zn ratios are associated with nutritional status, oxidative stress, inflammation, and immune abnormalities in patients on peritoneal dialysis. Clin. Biochem. 2011, 44, 275–280. [Google Scholar] [CrossRef]
- Osredkar, J.; Sustar, N. Copper and Zinc, Biological role and significance of copper/zinc imbalance. J. Clin. Toxicol. 2011, 3, 0495. [Google Scholar] [CrossRef]
- Canellas, C.G.; Carvalho, S.M.; Anjos, M.J.; Lopes, R.T. Determination of Cu/Zn and Fe in human serum of patients with sickle cell anemia using radiation synchrotron. Appl. Radiat. Isot. 2012, 70, 1277–1280. [Google Scholar] [CrossRef] [PubMed]
- Meret, S.; Henkin, R.I. Simultaneous direct estimation by atomic absorption spectrophotometry of copper and zinc in serum, urine, and cerebrospinal fluid. Clin. Chem. 1971, 17, 369–373. [Google Scholar] [PubMed]
- Al-Naama, L.; Hassan, M.; Mehdi, J. Association of erythrocytes anti-oxidant enzymes and their cofactors with markers of oxidative stress in patients with sickle cell anemia. Qatar Med. J. 2015, 14. [Google Scholar] [CrossRef]
- Dos Santos, T.; de Sousa, G.; Barbosa, M.; Goncalves, R. The role of iron overload on oxidative stress in sickle cell anemia. Biomark. Med. 2012, 6, 813–819. [Google Scholar] [CrossRef]
- Chirico, E.N.; Pialoux, V. Role of oxidative stress in the pathogenesis of sickle cell disease. IUBMB Life 2012, 64, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Gaetke, L.M.; Chow, C.K. Copper toxicity, oxidative stress, and antioxidant nutrients. Toxicology 2003, 189, 147–163. [Google Scholar] [CrossRef]
- Mahdi, J.K. Plasma zinc level in patients with sickle cell anemia. Tech. Res. J. 2001, 78, 7–13. [Google Scholar]
- Akenami, F.O.; Aken’Ova, Y.A.; Osifo, B.O. Serum zinc, copper and magnesium in sickle cell disease at Ibadan, South western Nigeria. Afr. J. Med. Sci. 1999, 28, 137–139. [Google Scholar]
- Prasad, A.S. Discovery of human zinc deficiency: Its impact on human health and disease. Adv. Nutr. 2013, 4, 176–190. [Google Scholar] [CrossRef] [PubMed]
- Prasad, S.A.; Beck, F.W.J.; Kaplan, J.; Chandrasekar, P.H.; Ortega, J.; Fitzgerald, J.T.; Swerdlow, P. Effect of zinc supplementation on incidence of infections and hospital admissions in sickle cell disease (SCD). Am. J. Hematol. 1999, 61, 194–202. [Google Scholar] [CrossRef]
- Cousins, R.; Cousins, R.J. Zinc. In Present Knowledge in Nutrition, 7th ed.; Ziegler, E.E., Filer, L.J., Jr., Eds.; International Life Sciences Institute Press: Washington, DC, USA, 1996. [Google Scholar]
- Bao, B.; Prasad, A.S.; Beck, F.W.J.; Snell, D.; Suneja, A.; Sarkar, F.H.; Doshi, N.; Fitzgerald, J.T.; Swerdlow, P. Zinc supplementation decreases oxidative stress, incidence of infection and generation of inflammatory cytokines in sickle cell disease patients. Transl. Res. 2008, 152, 67–80. [Google Scholar] [CrossRef] [PubMed]
- Leone, N.; Courbon, D.; Ducimetiere, P.; Zureik, M. Zinc, copper, and magnesium and risks for all-cause, cancer, and cardiovascular mortality. Epidemiology 2006, 17, 308–314. [Google Scholar] [CrossRef] [PubMed]
- Malavolta, M.; Giacconi, R.; Piacenza, F.; Santarelli, L.; Cipriano, C.; Costarelli, L.; Tesei, S.; Pierpaoli, S.; Basso, A.; Galeazzi, R.; et al. Plasma copper/zinc ratio: An inflammatory/nutritional biomarker as predictor of all-cause mortality in elderly population. Biogerontology 2010, 11, 309–319. [Google Scholar] [CrossRef]
- Reunanen, A.; Knekt, P.; Marniemi, J.; Maki, J.; Maatela, J.; Aromaa, A. Serum calcium, magnesium, copperand zinc and risk of cardiovascular death. Eur. J. Clin. Nutr. 1996, 50, 431–437. [Google Scholar]
- Mezzetti, A.; Pierdomenico, S.D.; Costantini, F.; Romano, F.; De, C.D.; Cuccurullo, F.; Imbastaro, T.; Riario-Sforza, G.; di Giacomo, F.; Zuliani, G.; et al. Copper/zinc ratio and systemic oxidant load: Effect of aging and aging-related degenerative diseases. Free Radic. Biol. Med. 1998, 25, 676–681. [Google Scholar] [CrossRef]


{kind=link}
| Parameter | Genotype | ||||
|---|---|---|---|---|---|
| HbAA (n = 50) | HbSC Steady State (n = 30) | HbSS Steady State (n = 34) | HbSC VOC (n = 11) | HbSS VOC (n = 15) | |
| Mean Age | 32.8 ± 10.4 years | 38.2 ± 15.1 years | 25.0 ± 9.0 years | 23.3 ± 9.5 years | 21.3 ± 4.6 years |
| Gender | |||||
| Male n (%) | 20 (40.0) | 13 (43.3) | 20 (58.8) | 5 (45.5) | 5 (33.3) |
| Female n (%) | 30 (60.0) | 17 (56.7) | 14 (41.2) | 6 (54.5) | 10 (66.7) |
| Parameter | Genotype | |||||
|---|---|---|---|---|---|---|
| HbAA (n = 50) | HbSC Steady State (n = 30) | HbSS Steady State (n = 34) | HbSC VOC (n = 11) | HbSS VOC (n = 15) | p-Value | |
| Iron (µg/dL) | 106.0 ± 12.7 | 123.8 ± 6.1 | 164.3 ± 7.2 | 139.3 ± 6.9 | 175.9 ± 5.3 | <0.001 |
| Copper (µg/dL) | 114.0 ± 16.3 | 179 ± 23.9 | 220.9 ± 27.8 | 194.6 ± 12.6 | 277.9 ± 41.7 | <0.001 |
| Zinc (µg/dL) | 101.4 ± 9.4 | 85.0 ± 6.9 | 66.5 ± 5.8 | 76.9 ± 5.2 | 51.3 ± 6.0 | <0.001 |
| Copper/Zinc ratio | 1.1 ± 0.2 | 2.1 ± 0.3 | 3.4 ± 0.6 | 2.5 ± 0.3 | 5.5 ± 1.0 | <0.001 |
| Haemoglobin (g/dL) | 11.5 ± 1.5 | 11.3 ± 1.5 | 8.9 ± 1.1 | 8.2 ± 0.8 | 6.9 ± 0.6 | <0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Antwi-Boasiako, C.; Dankwah, G.B.; Aryee, R.; Hayfron-Benjamin, C.; Doku, A.; N’guessan, B.B.; Asiedu-Gyekye, I.J.; Campbell, A.D. Serum Iron Levels and Copper-to-Zinc Ratio in Sickle Cell Disease. Medicina 2019, 55, 180. https://doi.org/10.3390/medicina55050180
Antwi-Boasiako C, Dankwah GB, Aryee R, Hayfron-Benjamin C, Doku A, N’guessan BB, Asiedu-Gyekye IJ, Campbell AD. Serum Iron Levels and Copper-to-Zinc Ratio in Sickle Cell Disease. Medicina. 2019; 55(5):180. https://doi.org/10.3390/medicina55050180
Chicago/Turabian StyleAntwi-Boasiako, Charles, Gifty B. Dankwah, Robert Aryee, Charles Hayfron-Benjamin, Alfred Doku, Benoit Banga N’guessan, Isaac Julius Asiedu-Gyekye, and Andrew D. Campbell. 2019. "Serum Iron Levels and Copper-to-Zinc Ratio in Sickle Cell Disease" Medicina 55, no. 5: 180. https://doi.org/10.3390/medicina55050180