3.1. Taxonomic Distribution
A total of 23 toothbrush microbiomes were analysed using NGS, revealing 1,581,052 sequences assigned to 2,341 OTUs (operational taxonomic units).
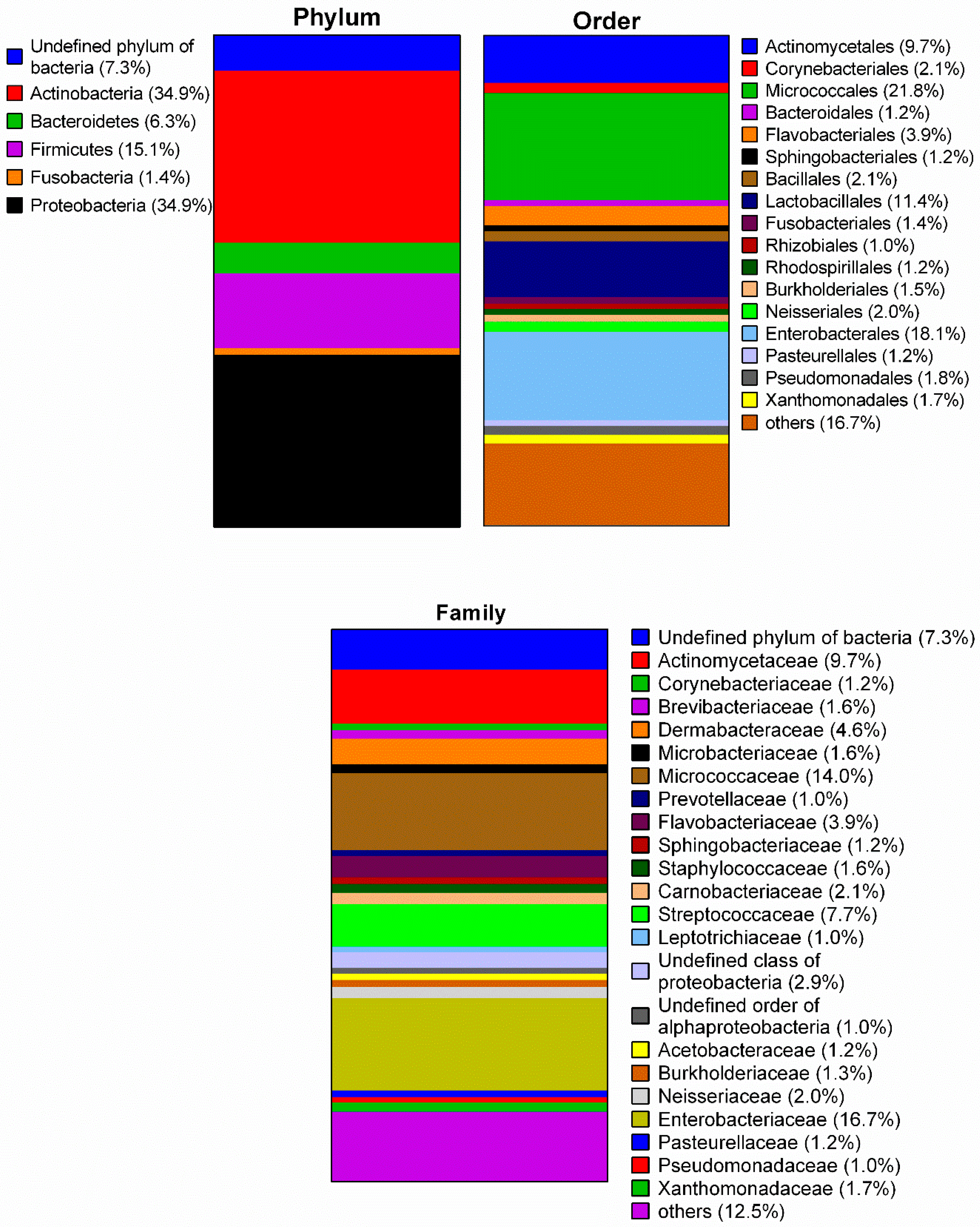
Figure 1 indicates the average microbial composition of the toothbrush samples at phylum-, order- and family-level. The analysis revealed nine phyla, 22 classes, 43 orders, 74 families, and 130 genera. The majority of identified bacteria belonged to the phyla
Actinobacteria (34.9%) and
Proteobacteria (34.9%) while the phyla
Deinococcus-Thermus,
Streptophyta, and
Cyanobacteria were poorly represented (<1.0%). Thus, the classes
Actinobacteria and
Gammaproteobacteria dominated with 34.6% and 23.1%, respectively (see
Table S1). The order
Micrococcales occurred most (21.8%) followed by
Enterobacterales (18.1%),
Lactobacillales (11.4%), and
Actinomycetales (9.7%).
Micrococcaceae (14.0%) were the most abundant family among
Actinobacteria,
Streptococcaceae (7.7%) among
Bacilli, and
Enterobacteriaceae (16.7%) among
Gammaproteobacteria.
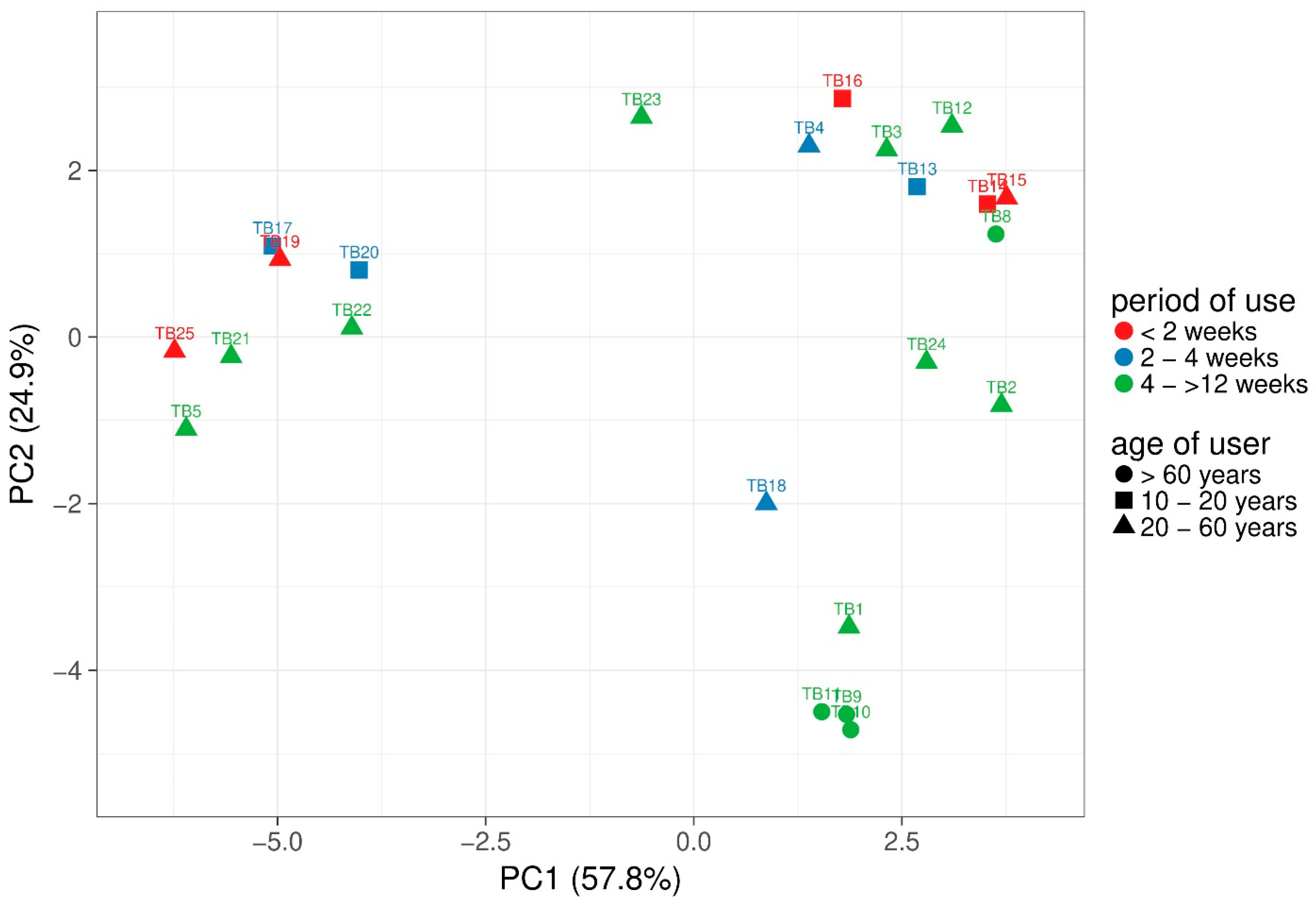
Alpha-diversity was calculated based on observed OTUs. Between 83 and 256 different species were observed per sample and Shannon index of the samples ranged from 3.45 to 7.06. However, non-parametric Kruskal-Wallis test revealed no significant differences of alpha diversity based on user age or period of use. To compare the different samples, principal component analysis (PCA) with weighted UniFrac distance analysis of the microbiomes was performed using ClustVis (
Figure 2) [
31]. Samples are coloured based on period of use and the different age is presented as shapes. The majority of the samples with short distances revealed strong variations of age and period of use. However, TB17 and TB19 clustered closely together and revealed a rather short period of use with two to four weeks and shorter than two weeks, respectively. Most of the samples TB3, TB4, TB8, TB12, TB13, TB14, TB15, and TB16 were used for a short period (<2 to 4 weeks) and although TB15, TB14, and TB8 were clustered closely together, only TB15 and TB14 were used for the same period and the age differed between all three samples. In contrast, TB24 and TB2 as well as TB9, TB10, and TB11 revealed the same period of use and age group.
Considering the order-level, Micrococcales occurred in all samples (TB17, TB21 and TB22 < 1.0%) and dominated on four toothbrushes (55–90%) while Enterobacterales were detected on 10 toothbrushes varying between 0.7 and 81%. Rothia and Kocuria were the most common genera of the Micrococcaceae, mainly represented by the species R. dentocariosa (15 samples) whereas Kocuria could not be identified to the species level in most samples. Although the Enterobacterales were dominantly Enterobacteriaceae, most could not be identified on species level but inter alia Klebsiella and Citrobacter occurred as genera. Besides, the orders Actinomycetales (0.3–42.0%) and Lactobacillales (0.1–37.1%) were detected in 22 and 23 samples, respectively. The genus Actinomyces (9.0%) was detected in all samples except TB10 with the dominating species Actinomyces oral taxon 448 (13 samples), A. massiliensis (13 samples), and A. oris (12 samples). For the Lactobacillales, the genus Streptococcus (7.7%) occurred in all analysed samples and amongst 44 different Streptococcus species in the samples, S. sanguinis (18 samples), S. mitis (15 samples), S. cristatus (12 samples), and S. oralis (11 samples) occurred most often. Furthermore, Haemophilus parainfluenzae and the Streptococcus like bacterium Granulicatella adiacens were identified in 17, Gemella haemolysins in 14, Lautropia mirabilis in 13, and Fusobacterium nucleatum as well as Kingella oralis in 12 toothbrush samples.
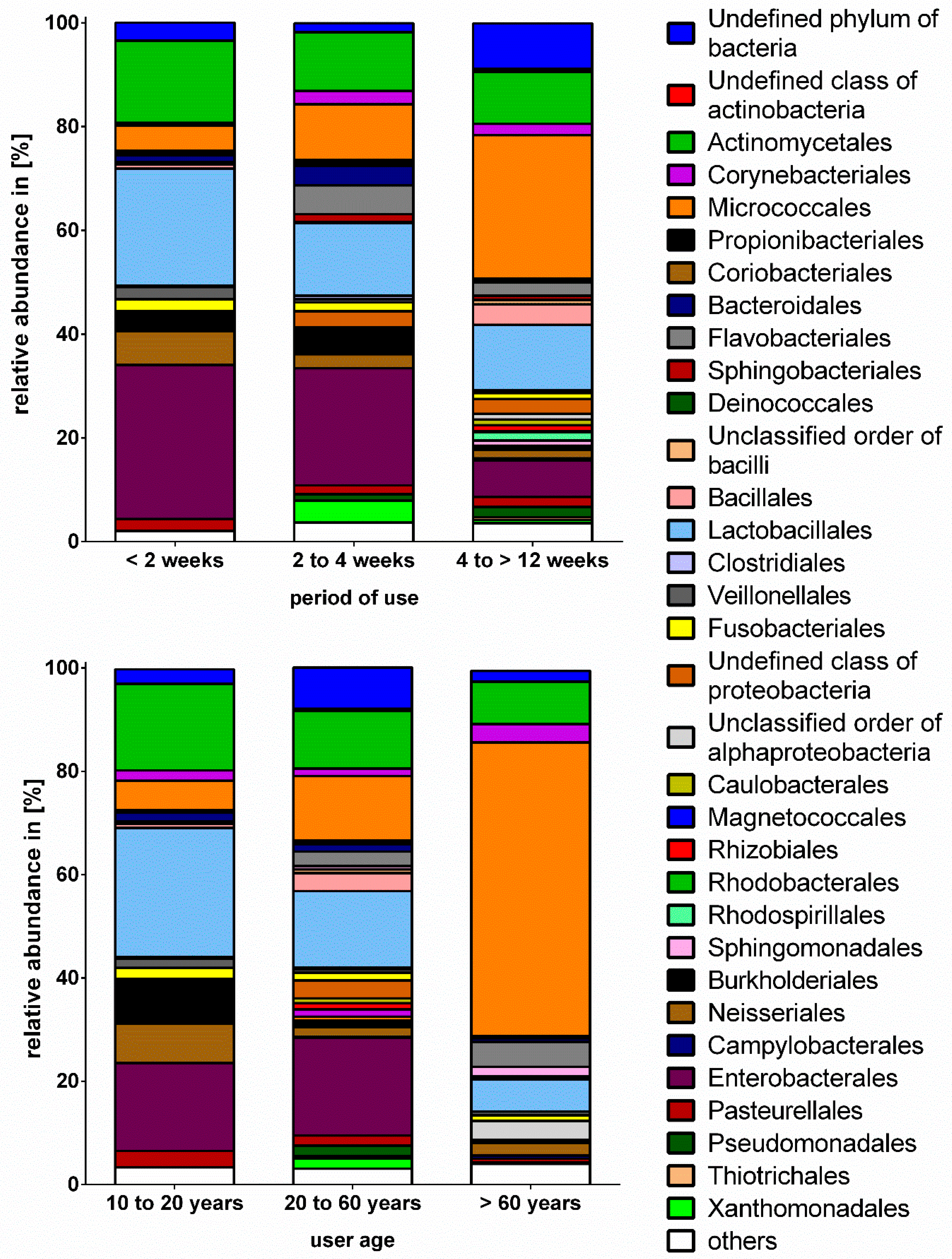
Due to the low number of toothbrushes used for more than 12 weeks (
n = 2), samples are presented combined as the group four to >12 weeks. The comparison of the taxonomic composition on order level revealed significant differences between samples grouped by period of use (
Figure 3). Although beta-diversity did not differ significantly between samples grouped based on period of use, non-parametric Mann-Whitney test (
p ≤ 0.05) revealed significant differences based on order level between the usage of less than two weeks and four to >12 weeks. The percentage of
Micrococcales was significantly higher in the group four to >12 weeks compared to >2 weeks, while the percentage of
Enterobacterales was significantly lower (
Table 1). Moreover, the amount of
Lactobacillales,
Actinomycetales,
Enterobacterales, and
Neisserales slightly decreased from shortest to longest period of use. Interestingly, the
Pseudomonadales and
Sphingomonadales were not detected in toothbrush samples used for less than two weeks whereas toothbrushes used for a period between four and >12 weeks revealed the highest, but still very low percentages of these bacterial orders. When comparing the microbial composition based on user age, the group of >60 years differed significantly from group 20 to 60 years and revealed a significantly higher percentage of
Micrococcales while no
Enterobacterales were detected. The
Lactobacillales dominated in the group of the youngest participants and the
Enterobacterales were slightly lower compared to the group 20 to 60 years. The prevalence of
Micrococcales seemed to increase with increasing age and
Pseudomonadales only occurred in the groups 20 to 60 and >60 years. However,
Lactobacillales and
Actinomycetales decreased from the group 10 to 20 years to the group of >60 years (
Table 3).
3.2. Microbial Contamination of Toothbrushes
A total number of 25 toothbrushes with varying period of use and user age (
Table 4) was analysed to determine the microbial contamination using culture-based approaches. The means of total viable counts (TVC) under aerobic and anaerobic conditions as well as the amount of
Streptococcus spp., gram-negatives and fungi are shown in
Table 5. High bacterial counts (1.42 × 10
6 cfu·mL
−1 to 1.19 × 10
7 cfu·mL
−1) were found on all tested media.
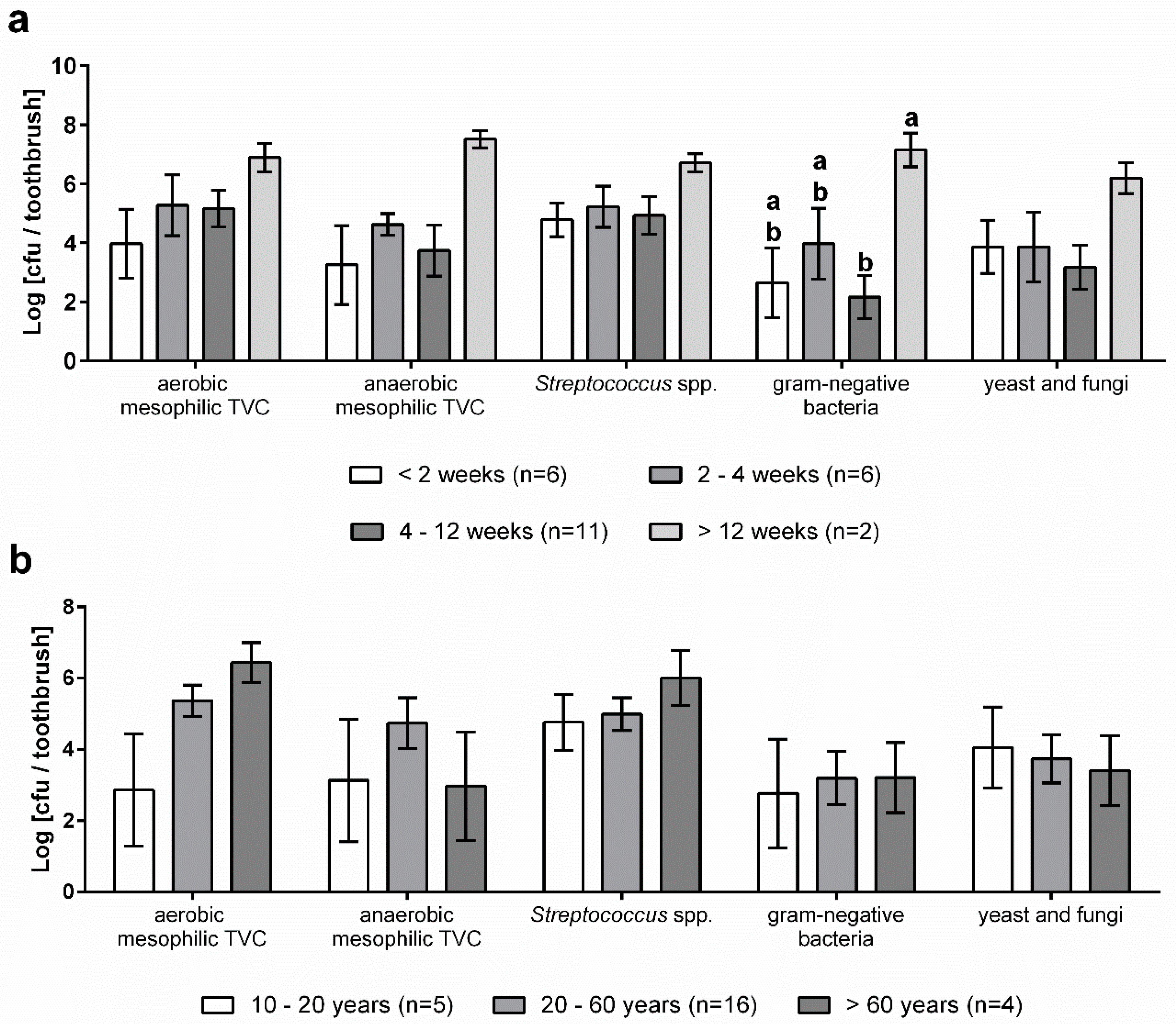
Figure 4 shows the microbiological contamination of toothbrushes in relation to the age of users and the period of use. Although the aerobic mesophilic TVC of toothbrushes of older users was much higher compared to younger users, the means did not differ significantly (
p = 0.9). In contrast, the other media tested revealed only minor differences between the age groups (
Figure 4b). The anaerobic mesophilic TVC was highest in samples of the age group between 20 and 60 years and the microbial count of
Streptococcus spp. was higher in samples belonging to the group of >60 years.
In addition, the microbial counts on toothbrushes were evaluated grouped by the period of use (
Figure 4a). The highest bacterial loads were determined for a period of use of more than 12 weeks on all media tested (3.25 × 10
5 cfu·toothbrush
−1 to 7.50 × 10
6 cfu·toothbrush
−1) and the count of gram-negative bacteria was significantly higher compared to the other periods. However, no trends for the other use periods were identified.
3.3. Occurrence of Antibiotic Resistance Genes
Besides NGS, qPCR for the screening of beta-lactamase (
bla), mobile colistin resistance (
mcr), and class 1 integron integrase (
intI1) genes was performed. As a result of our investigation, in 20 of the analysed samples,
bla genes were detected; while no
mcr genes occurred and all samples, except TB6 and TB14, revealed the presence of class 1 integrons. Of the 13
bla types chosen for screening, only
blaACT/MIR,
blaCMY-2,
blaGES,
blaKPC,
blaOXA-48,
blaOXA-23 and
blaOXA-58 occurred in the toothbrush samples (
Table 6).
BlaOXA-58 was most frequently identified, followed by
blaOXA-23 and
blaGES.
The absolute abundance of both total ARGs and
intI1 varied strongly across samples, thus no significant differences were detected (
Figure 5). However, in all samples of the group, 20 to 60 years ARGs were detected and
intI1 revealed the highest abundance as well. Despite a shorter period of use, toothbrushes used between two and four weeks revealed the highest values of both ARGs and
intI1.
3.4. In-Vitro Study of Different Types of Toothbrush Bristles
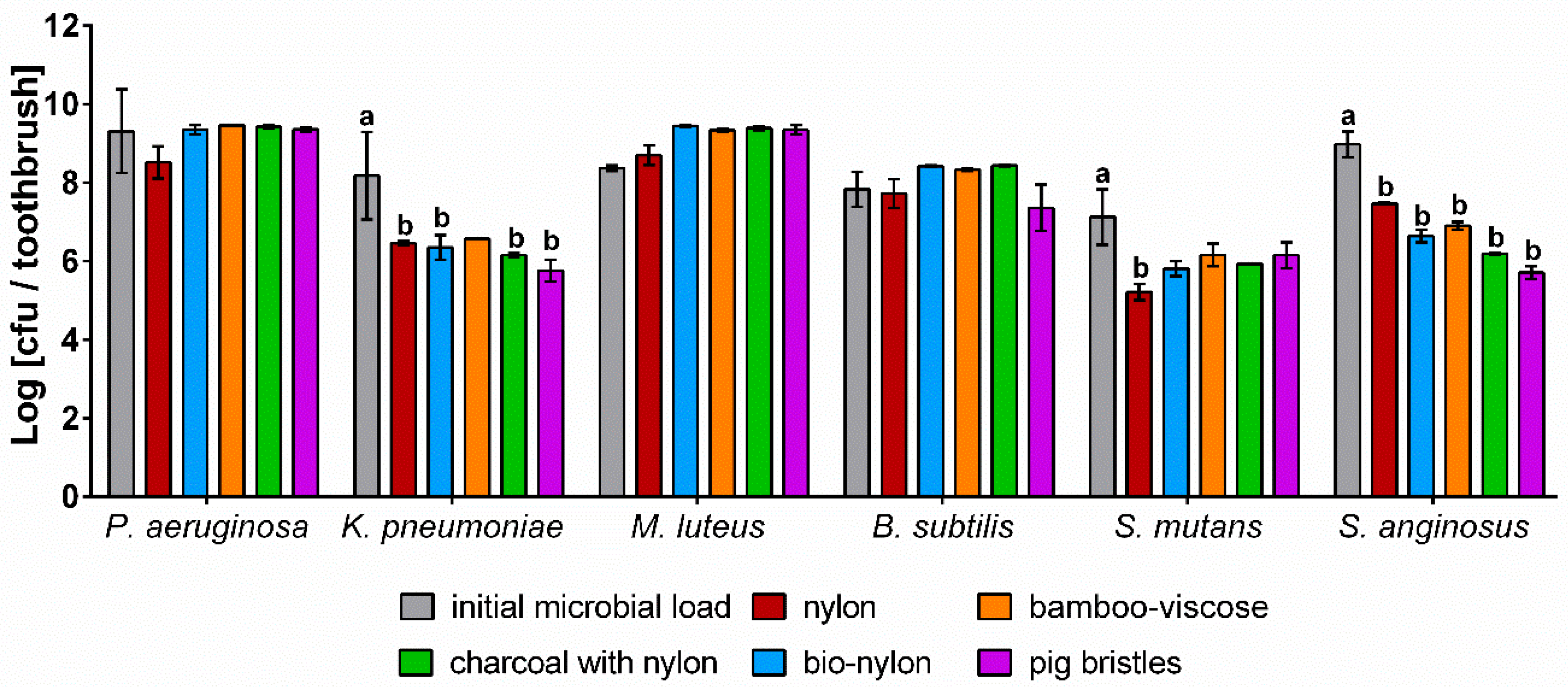
To examine the survival and retention of bacteria on toothbrushes and the effect of different bristle materials on microbial growth and survival, toothbrushes were artificially contaminated twice a day with six different microorganisms (
Figure 6).
All test strains were detected on the toothbrushes after a period of one week with bacterial loads close to the initial count of the bacterial suspensions. None of the bristle types tested revealed a particular antimicrobial effect, although charcoal bristles and bamboo bristles are supposed to have antimicrobial properties. However, no positive influence on bacterial growth was observed as well. While the lowest bacterial counts were determined for either nylon or pig bristles, the other bristle materials showed nearly no differences. Although the bristle type only had a minor effect, the test strains differed in growth. In case of P. aeruginosa, M. luteus, and B. subtilis, the TVC on the tested bristle types slightly increased or revealed the same amount compared to the microbial load of the bacterial suspension. In contrast, lower TVCs of K. pneumoniae, S. mutans, and S. anginosus remained on all bristle types, even revealing significant differences compared to the bacterial suspension. Similar to the NGS results, the in-vitro tests showed an increase of Micrococcales on the toothbrushes as well, while Streptococcus spp. and Enterobacteriaceae revealed lower bacterial loads.









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}