Dietary Fiber Intake (Supplemental or Dietary Pattern Rich in Fiber) and Diabetic Kidney Disease: A Systematic Review of Clinical Trials

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Searches
2.2. Study Selection
2.3. Data Extraction and Quality Assessment
3. Results
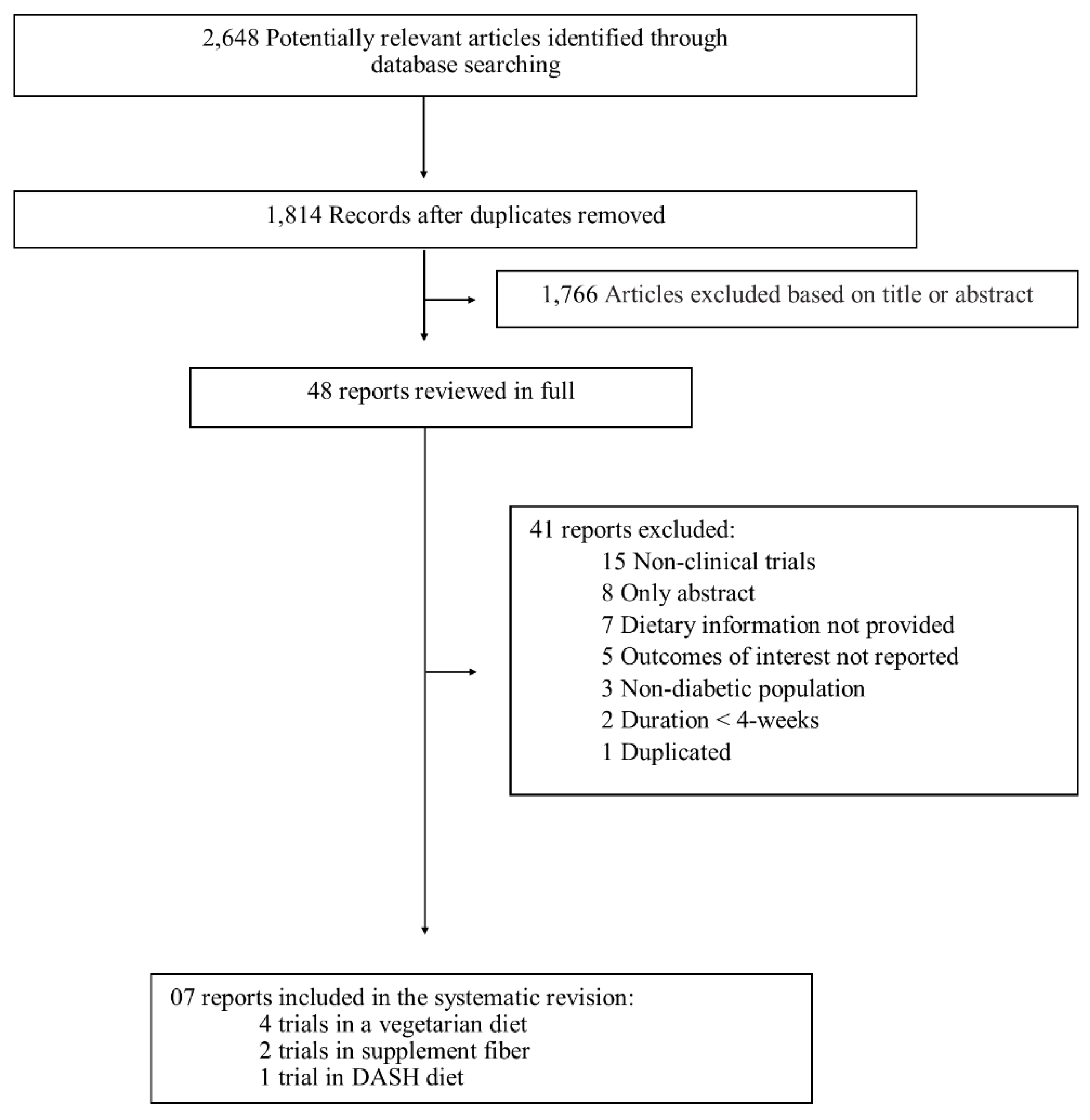
3.1. Literature Search
3.2. Study Characteristics
3.3. Vegetarian diet
3.3.1. Type 1 DM
3.3.2. Type 2 DM
3.4. Fiber Supplement
3.5. DASH Diet
3.6. Methodological Quality Assessment of Studies
4. Discussion
Author Contributions
Acknowledgments
Conflicts of Interest
Appendix A. MEDLINE Search Strategy for the Systematic Review
Appendix B. Excluded Studies of the Systematic Review (n = 41)
| Author | Year | Periodic | Reasons to exclusion |
| Paisey | 1984 | Diabetes Care | Non-clinical trials |
| Parillo | 1984 | Minerva Endocrinologica | Duration <4-weeks |
| Barsotti | 1987 | Infusionstherapie und Klinische Ernährung | Only abstract |
| Parillo | 1988 | American Journal of Clinical Nutrition | Duration <4-weeks |
| Barsotti | 1988 | Contributions of Nephrology | Only abstract |
| Naumova | 1990 | Vŭtreshni Bolesti | Only abstract |
| Barsotti | 1991 | American Journal of Nephrology | Non-diabetic population |
| Metcalf | 1993 | Clinical Chemistry | Outcomes of interest not reported |
| Hadfield | 1993 | Practical Diabetes | Non-clinical trials |
| Oldrizzi | 1994 | Journal of the American Society of Neprhology | Dietary information not provided |
| Citro | 1998 | Minerva Endocrinologica | Outcomes of interest not reported |
| GSEDNu | 2006 | Journal of Diabetes and Complications | Non-clinical trials |
| Brunori | 2007 | American Journal of Kidney Diseases | Non-diabetic population |
| Cámara | 2008 | Revista Espanhola de Salud Publica | Outcomes of interest not reported |
| Glover | 2009 | Food Hydrocolloids | Outcomes of interest not reported |
| Teixeira | 2010 | Diabetes | Outcomes of interest not reported |
| Gong | 2011 | Diabetologia | Dietary information not provided |
| Lin | 2011 | American Journal of Kidney Diseases | Dietary information not provided |
| Sun | 2011 | Journal of Chinese Clinical Medicine | Only abstract |
| Reddy | 2012 | Kidney Research Clinical Practice | Non-clinical trials |
| Dunkler | 2013 | JAMA Internal Medicine | Non-clinical trials |
| Chang | 2013 | American Journal of Kidney Diseases | Non-clinical trials |
| Tirosh | 2013 | Diabetes Care | Only abstract |
| Dans | 2013 | Phillipine Journal of Internal med | Only abstract |
| Khatri | 2014 | Clinical Journal of the American Society of Nephrology | Non-clinical trials |
| Hsu | 2014 | Clinical Nutrition | Non-clinical trials |
| Xu | 2014 | Clinical Journal of the American Society of Nephrology | Non-clinical trials |
| Díaz-López | 2015 | Diabetes Care | Dietary information not provided |
| Villarini | 2015 | Annali di Igiene | Non-diabetic population |
| Lee | 2015 | Nephrology Dialysis Transplantation | Non-clinical trials |
| Nazha | 2015 | Nephrology Dialysis Transplantation | Only abstract |
| Rebholz | 2016 | American Journal of Kidney Diseases | Duplicated |
| Dunkler | 2016 | American Journal of Kidney Diseases | Non-clinical trials |
| Piccoli | 2016 | BMC Nephrology | Dietary information not provided |
| Ashgari | 2016 | Hypertension Research | Non-clinical trials |
| Hirahatake | 2016 | Circulation | Dietary information not provided |
| Rebhold | 2016 | American Journal of Nephrology | Non-clinical trials |
| Mejia | 2016 | The FASEB Journal | Only abstract |
| Ashgari | 2017 | Nephrology, Dialysis, Transplantation | Non-clinical trials |
| Horikawa | 2017 | Nutrients | Non-clinical trials |
| Duncan | 2017 | Diabetology and Metabolic Syndrome | Dietary information not provided |
References
- International Diabetes Federation. IDF Diabetes Atlas, 8th ed.; International Diabetes Federation: Brussels, Belgium, 2017. [Google Scholar]
- Slabaugh, S.L.; Curtis, B.H.; Clore, G.; Fu, H.; Schuster, D.P. Factors associated with increased healthcare costs in Medicare Advantage patients with type 2 diabetes enrolled in a large representative health insurance plan in the US. J. Med. Econ. 2015, 18, 106–112. [Google Scholar] [CrossRef] [PubMed]
- Lupsa, B.C.; Inzucchi, S.E. Diabetes medications and cardiovascular disease: At long last progress. Curr. Opin. Endocrinol. Diabetes Obes. 2018, 25, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Sarnak, M.J.; Levey, A.S.; Schoolwerth, A.C.; Coresh, J.; Culleton, B.; Hamm, L.L.; McCullough, P.A.; Kasiske, B.L.; Kelepouris, E.; Klag, M.J.; et al. Kidney disease as a risk factor for development of cardiovascular disease: A statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Circulation 2003, 108, 2154–2169. [Google Scholar] [CrossRef] [PubMed]
- Lima, E.G.; Hueb, W.; Gersh, B.J.; Rezende, P.C.; Garzillo, C.L.; Favarato, D.; Hueb, A.C.; Rahmi Garcia, R.M.; Franchini Ramires, J.A.; Filho, R.K. Impact of Chronic Kidney Disease on Long-Term Outcomes in Type 2 Diabetic Patients With Coronary Artery Disease on Surgical, Angioplasty, or Medical Treatment. Ann. Thorac. Surg. 2016, 101, 1735–1744. [Google Scholar] [CrossRef] [PubMed]
- Ko, G.J.; Kalantar-Zadeh, K.; Goldstein-Fuchs, J.; Rhee, C.M. Dietary Approaches in the Management of Diabetic Patients with Kidney Disease. Nutrients 2017, 9, 824. [Google Scholar] [CrossRef] [PubMed]
- Silva, F.M.; Kramer, C.K.; de Almeida, J.C.; Steemburgo, T.; Gross, J.L.; Azevedo, M.J. Fiber intake and glycemic control in patients with type 2 diabetes mellitus: A systematic review with meta-analysis of randomized controlled trials. Nutr. Rev. 2013, 71, 790–801. [Google Scholar] [CrossRef] [PubMed]
- McRae, M.P. Dietary Fiber Is Beneficial for the Prevention of Cardiovascular Disease: An Umbrella Review of Meta-analyses. J. Chiropr. Med. 2017, 16, 289–299. [Google Scholar] [CrossRef]
- Evert, A.B.; Boucher, J.L.; Cypress, M.; Dunbar, S.A.; Franz, M.J.; Mayer-Davis, E.J.; Neumiller, J.J.; Nwankwo, R.; Verdi, C.L.; Urbanski, P.; et al. Nutrition therapy recommendations for the management of adults with diabetes. Diabetes Care 2014, 37 (Suppl. 1), S120–S143. [Google Scholar] [CrossRef]
- American Diabetes Association. 4. Lifestyle Management: Standards of Medical Care in Diabetes-2018. Diabetes Care 2018, 41 (Suppl. 1), S38–S50. [Google Scholar] [CrossRef]
- Eckel, R.H.; Jakicic, J.M.; Ard, J.D.; de Jesus, J.M.; Houston Miller, N.; Hubbard, V.S.; Lee, I.M.; Lichtenstein, A.H.; Loria, C.M.; Millen, B.E.; et al. 2013 AHA/ACC guideline on lifestyle management to reduce cardiovascular risk: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2014, 129 (Suppl. 2), S76–S99. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services and U.S. Department of Agriculture. 2015–2020 Dietary Guidelines for Americans, 8th ed.; U.S. Department of Health and Human Services and U.S. Department of Agriculture: Washington, DC, USA, 2015.
- Molitch, M.E.; Adler, A.I.; Flyvbjerg, A.; Nelson, R.G.; So, W.Y.; Wanner, C.; Kasiske, B.L.; Wheeler, D.C.; de Zeeuw, D.; Mogensen, C.E. Diabetic kidney disease: A clinical update from Kidney Disease: Improving Global Outcomes. Kidney Int. 2015, 87, 20–30. [Google Scholar] [CrossRef] [PubMed]
- Academy of Nutrition and Dietetics Evidence Analysis Library, 2015. Chronic Kidney Disease (CKD) Evidence-Based Nutrition Practice Guideline. 2010. USA. Available online: https://www.andeal.org/topic.cfm?cat=3927 (accessed on 1 February 2019).
- Higgins JPT GSe. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [Updated March 2011]; The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. 10. Microvascular Complications and Foot Care: Standards of Medical Care in Diabetes-2018. Diabetes Care 2018, 41 (Suppl. 1), S105–S118. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- De Mello, V.D.; Zelmanovitz, T.; Perassolo, M.S.; Azevedo, M.J.; Gross, J.L. Withdrawal of red meat from the usual diet reduces albuminuria and improves serum fatty acid profile in type 2 diabetes patients with macroalbuminuria. Am. J. Clin. Nutr. 2006, 83, 1032–1038. [Google Scholar] [CrossRef] [PubMed]
- Kontessis, P.A.; Bossinakou, I.; Sarika, L.; Iliopoulou, E.; Papantoniou, A.; Trevisan, R.; Roussi, D.; Stipsanelli, K.; Grigorakis, S.; Souvatzoglou, A. Renal, metabolic, and hormonal responses to proteins of different origin in normotensive, nonproteinuric type I diabetic patients. Diabetes Care 1995, 18, 1233. [Google Scholar] [CrossRef] [PubMed]
- Jibani, M.M.; Bloodworth, L.L.; Foden, E.; Griffiths, K.D.; Galpin, O.P. Predominantly vegetarian diet in patients with incipient and early clinical diabetic nephropathy: Effects on albumin excretion rate and nutritional status. Diabet. Med. 1991, 8, 949–953. [Google Scholar] [CrossRef]
- Dall’Alba, V.; Silva, F.M.; Antonio, J.P.; Steemburgo, T.; Royer, C.P.; Almeida, J.C.; Gross, J.L.; Azevedo, M.J. Improvement of the metabolic syndrome profile by soluble fibre—Guar gum—In patients with type 2 diabetes: A randomised clinical trial. Br. J. Nutr. 2013, 110, 1601–1610. [Google Scholar] [CrossRef]
- Paula, T.P.; Viana, L.V.; Neto, A.T.; Leitao, C.B.; Gross, J.L.; Azevedo, M.J. Effects of the DASH Diet and Walking on Blood Pressure in Patients With Type 2 Diabetes and Uncontrolled Hypertension: A Randomized Controlled Trial. J. Clin. Hypertens. (Greenwich) 2015, 17, 895–901. [Google Scholar] [CrossRef]
- Nicholson, A.S.; Sklar, M.; Barnard, N.D.; Gore, S.; Sullivan, R.; Browning, S. Toward improved management of NIDDM: A randomized, controlled, pilot intervention using a lowfat, vegetarian diet. Prev. Med. 1999, 29, 87–91. [Google Scholar] [CrossRef]
- Farhangi, M.A.; Javid, A.Z.; Dehghan, P. The effect of enriched chicory inulin on liver enzymes, calcium homeostasis and hematological parameters in patients with type 2 diabetes mellitus: A randomized placebo-controlled trial. Prim. Care Diabetes 2016, 10, 265–271. [Google Scholar] [CrossRef]
- Maezawa, Y.; Takemoto, M.; Yokote, K. Cell biology of diabetic nephropathy: Roles of endothelial cells, tubulointerstitial cells and podocytes. J. Diabetes Investig. 2015, 6, 3–15. [Google Scholar] [CrossRef] [PubMed]
- Fujii, H.; Iwase, M.; Ohkuma, T.; Ogata-Kaizu, S.; Ide, H.; Kikuchi, Y.; Idewaki, Y.; Joudai, T.; Hirakawa, Y.; Uchida, K.; et al. Impact of dietary fiber intake on glycemic control, cardiovascular risk factors and chronic kidney disease in Japanese patients with type 2 diabetes mellitus: The Fukuoka Diabetes Registry. Nutr. J. 2013, 12, 159. [Google Scholar] [CrossRef] [PubMed]
- Post, R.E.; Mainous, A.G., 3rd; King, D.E.; Simpson, K.N. Dietary fiber for the treatment of type 2 diabetes mellitus: A meta-analysis. J. Am. Board Fam. Med. 2012, 25, 16–23. [Google Scholar] [CrossRef] [PubMed]
- De Carvalho, C.M.; de Paula, T.P.; Viana, L.V.; Machado, V.M.; de Almeida, J.C.; Azevedo, M.J. Plasma glucose and insulin responses after consumption of breakfasts with different sources of soluble fiber in type 2 diabetes patients: A randomized crossover clinical trial. Am. J. Clin. Nutr. 2017, 106, 1238–1245. [Google Scholar] [CrossRef]
- Showail, A.A.; Ghoraba, M. The association between glycemic control and microalbuminuria in Type 2 diabetes. Saudi J. Kidney Dis. Transplant. 2016, 27, 473–479. [Google Scholar] [CrossRef]
- DCCT/EDIC Research Group. Effect of intensive diabetes treatment on albuminuria in type 1 diabetes: Long-term follow-up of the Diabetes Control and Complications Trial and Epidemiology of Diabetes Interventions and Complications study. Lancet Diabetes Endocrinol. 2014, 2, 793–800. [Google Scholar] [CrossRef]
- Chen, W.Z.; Hung, C.C.; Wen, Y.W.; Ning, H.C.; Gau, B.R.; Huang, Y.Y. Effect of glycemic control on microalbuminuria development among type 2 diabetes with high-normal albuminuria. Ren. Fail. 2014, 36, 171–175. [Google Scholar] [CrossRef]
- Metcalf, P.A.; Baker, J.R.; Scragg, R.K.; Dryson, E.; Scott, A.J.; Wild, C.J. Dietary nutrient intakes and slight albuminuria in people at least 40 years old. Clin. Chem. 1993, 39, 2191–2198. [Google Scholar]
- Kondo, K.; Morino, K.; Nishio, Y.; Ishikado, A.; Arima, H.; Nakao, K.; Nakagawa, F.; Nikami, F.; Sekine, O.; Nemoto, K.I.; et al. Fiber-rich diet with brown rice improves endothelial function in type 2 diabetes mellitus: A randomized controlled trial. PLoS ONE 2017, 12, e0179869. [Google Scholar] [CrossRef]
- Chiavaroli, L.; Mirrahimi, A.; Sievenpiper, J.L.; Jenkins, D.J.; Darling, P.B. Dietary fiber effects in chronic kidney disease: A systematic review and meta-analysis of controlled feeding trials. Eur. J. Clin. Nutr. 2015, 69, 761–768. [Google Scholar] [CrossRef] [PubMed]
- Salmean, Y.A.; Segal, M.S.; Langkamp-Henken, B.; Canales, M.T.; Zello, G.A.; Dahl, W.J. Foods with added fiber lower serum creatinine levels in patients with chronic kidney disease. J. Ren. Nutr. 2013, 23, e29–e32. [Google Scholar] [CrossRef] [PubMed]
- Mirmiran, P.; Yuzbashian, E.; Asghari, G.; Sarverzadeh, S.; Azizi, F. Dietary fibre intake in relation to the risk of incident chronic kidney disease. Br. J. Nutr. 2018, 119, 479–485. [Google Scholar] [CrossRef] [PubMed]
- Kelly, J.T.; Palmer, S.C.; Wai, S.N.; Ruospo, M.; Carrero, J.J.; Campbell, K.L.; Strippoli, G.F. Healthy Dietary Patterns and Risk of Mortality and ESRD in CKD: A Meta-Analysis of Cohort Studies. Clin. J. Am. Soc. Nephrol. 2017, 12, 272–279. [Google Scholar] [CrossRef] [PubMed]
- Gluba-Brzozka, A.; Franczyk, B.; Rysz, J. Vegetarian Diet in Chronic Kidney Disease-A Friend or Foe. Nutrients 2017, 9, 374. [Google Scholar] [CrossRef] [PubMed]
- Melina, V.; Craig, W.; Levin, S. Position of the Academy of Nutrition and Dietetics: Vegetarian Diets. J. Acad. Nutr. Diet. 2016, 116, 1970–1980. [Google Scholar] [CrossRef] [PubMed]
- Lohsiriwat, S. Protein Diet and Estimated Glomerular Filtration Rate. Open J. Nephrol. 2013, 3, 97–100. [Google Scholar] [CrossRef]
- Barai, S.; Gambhir, S.; Prasad, N.; Sharma, R.K.; Ora, M.; Kumar, A.; Gupta, A.; Parasar, D.S.; Suneetha, B. Levels of GFR and protein-induced hyperfiltration in kidney donors: A single-center experience in India. Am. J. Kidney Dis. 2008, 51, 407–414. [Google Scholar] [CrossRef]
- Moorthi, R.N.; Vorland, C.J.; Hill Gallant, K.M. Diet and Diabetic Kidney Disease: Plant Versus Animal Protein. Curr. Diabetes Rep. 2017, 17, 15. [Google Scholar] [CrossRef]
- Kaysen, G.A.; Odabaei, G. Dietary protein restriction and preservation of kidney function in chronic kidney disease. Blood Purif. 2013, 35, 22–25. [Google Scholar] [CrossRef]
- Jacobs, D.R., Jr.; Gross, M.D.; Steffen, L.; Steffes, M.W.; Yu, X.; Svetkey, L.P.; Appel, L.J.; Vollmer, W.M.; Bray, G.A.; Moore, T.; et al. The effects of dietary patterns on urinary albumin excretion: Results of the Dietary Approaches to Stop Hypertension (DASH) Trial. Am. J. Kidney Dis. 2009, 53, 638–646. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; Fung, T.T.; Hu, F.B.; Curhan, G.C. Association of dietary patterns with albuminuria and kidney function decline in older white women: A subgroup analysis from the Nurses’ Health Study. Am. J. Kidney Dis. 2011, 57, 245–254. [Google Scholar] [CrossRef] [PubMed]
- Rebholz, C.M.; Crews, D.C.; Grams, M.E.; Steffen, L.M.; Levey, A.S.; Miller, E.R., 3rd; Appel, L.J.; Coresh, J. DASH (Dietary Approaches to Stop Hypertension) Diet and Risk of Subsequent Kidney Disease. Am. J. Kidney Dis. 2016, 68, 853–861. [Google Scholar] [CrossRef] [PubMed]
- Asghari, G.; Farhadnejad, H.; Mirmiran, P.; Dizavi, A.; Yuzbashian, E.; Azizi, F. Adherence to the Mediterranean diet is associated with reduced risk of incident chronic kidney diseases among Tehranian adults. Hypertens. Res. 2017, 40, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Diaz-Lopez, A.; Babio, N.; Martinez-Gonzalez, M.A.; Corella, D.; Amor, A.J.; Fito, M.; Estruch, R.; Aros, F.; Gomez-Gracia, E.; Fiol, M.; et al. Mediterranean Diet, Retinopathy, Nephropathy, and Microvascular Diabetes Complications: A Post Hoc Analysis of a Randomized Trial. Diabetes Care 2015, 38, 2134–2141. [Google Scholar] [CrossRef] [PubMed]
- Diaz-Lopez, A.; Bullo, M.; Martinez-Gonzalez, M.A.; Guasch-Ferre, M.; Ros, E.; Basora, J.; Covas, M.I.; del Carmen Lopez-Sabater, M.; Salas-Salvado, J.; Investigators, P.R.S. Effects of Mediterranean diets on kidney function: A report from the PREDIMED trial. Am. J. Kidney Dis. 2012, 60, 380–389. [Google Scholar] [CrossRef] [PubMed]
- Dahl, W.J.; Stewart, M.L. Position of the Academy of Nutrition and Dietetics: Health Implications of Dietary Fiber. J. Acad. Nutr. Diet. 2015, 115, 1861–1870. [Google Scholar] [CrossRef]
- EFSA Panel on Dietetic Products, Nutrition, and Allergies (NDA). Scientific Opinion on Dietary Reference Values for carbohydrates and dietary fibre. EFSA J. 2010, 8, 1462. [Google Scholar]
- Medina-Remon, A.; Kirwan, R.; Lamuela-Raventos, R.M.; Estruch, R. Dietary patterns and the risk of obesity, type 2 diabetes mellitus, cardiovascular diseases, asthma, and neurodegenerative diseases. Crit. Rev. Food Sci. Nutr. 2018, 58, 262–296. [Google Scholar] [CrossRef]
- Krishnamurthy, V.M.; Wei, G.; Baird, B.C.; Murtaugh, M.; Chonchol, M.B.; Raphael, K.L.; Greene, T.; Beddhu, S. High dietary fiber intake is associated with decreased inflammation and all-cause mortality in patients with chronic kidney disease. Kidney Int. 2012, 81, 300–306. [Google Scholar] [CrossRef]


{kind=link}
| Dietary Patterns/ Guidelines Recommendations | Main Foods | Nutrients Characteristics |
|---|---|---|
| DASH diet 1,2,4 | Includes vegetables, fruits, whole grains, fat-free or low-fat dairy products, fish, poultry, beans, nuts, and vegetable oils; <25% dietary intake from fat; low in sweets, sugar-sweetened beverages, and tropical oils. | Low in saturated fats and cholesterol Rich in fiber Rich in protein |
| Vegetarian diet 2,3, 4 | Includes whole grains, vegetables, fruits, legumes, nuts, seeds, soy and, if desired, dairy products, and eggs. Does not include meat, fowl or seafood, or products containing those foods. | Rich in fiber Rich in n-6 fatty acids Rich in vegetable protein |
| Mediterranean diet 1,2,4 | Includes fruits, vegetables, whole grains, beans, nuts, seeds, seafood, olive oil; low to moderate amounts of poultry, and dairy products, with little red meat; low to moderate wine consumption (optional). | Rich in fiber Rich in monounsaturated and polyunsaturated fat |
| Guidelines recommendations | 1 AHA: Rich in fiber 2 American Guideline: 14 g/1000kcal 5 European Guideline: 25 g/day 4 ADA: 14g/1000 kcal or 25 g/day women, 38 g/day men 6 KDOQI/7KDIGO: no specific recommendation | |
| Author Year Country | Sample Characteristics | Study Design | Diet Characteristics | Renal Outcomes |
|---|---|---|---|---|
| Type 1 diabetes | ||||
| Vegetarian diet | ||||
| Jibani 1991 n = 8 United Kingdom | Females: 37.5% Hypertension: 25% Age: 46 (22–70) years HbA1c: NA BMI: NA Withdrawals: 20% Duration: 8-weeks | Crossover clinical trial Washout: 8-weeks | Intervention (n = 10): vegetarian diet * Energy: 32 (23–34) kcal/kg/day CHO: 3.4 (2.3–4.2) g/kg/day; Prot: 1.0 g/kg/day; Lip: 1.2 g/kg/day Total fiber: 0.4 g/kg/day Soluble fiber: NA Insoluble fiber: NA Control (n = 10): conventional diet * Energy: 29 (15–35) kcal/kg /day CHO: 3.7 (2.6–4.6) g/kg/day; Prot: 1.4 g/kg/day; Lip: 1.4 g/kg/day Total fiber: 0.3 g/kg/day Soluble fiber: NA Insoluble fiber: NA | Intervention eGFR (mL/min/1.73 m2) § Final: 109 (48–163) Fractional albumin clearance (x10−4) ** Final: 87 (23–829) Control eGFR (mL/min/1.73 m2) Final: 109 (45–134) Fractional albumin clearance (x10−4) Final: 188 (58–810) |
| Kontessis 1995 n = 9 Greece | Females: 77.8% Hypertension: 0% Age: 32 (20–48) years HbA1c: 6.7 (5.1–8.4)% BMI: 23.8 (20.6–27.8) kg/m2 Withdrawals: 0% Duration: 4-weeks | Randomized crossover clinical trial Washout: ≥1-week | Intervention (n = 9): vegetal protein diet * Energy: 22.8 ± 3.8 kcal/kg/day CHO: 2.8 ± 0.7 g/kg/day; Prot: 0.95 ± 0.3 g/kg/day; Lip: 0.9 ± 0.1 g/kg/day Total fiber: 0.2 ± 0.03 g/kg/day Soluble fiber: NA Insoluble fiber: NA Control (n = 9): animal protein diet * Energy: 23.3 ± 3.7 kcal/kg /day CHO: 2.4 ± 0.65 g/kg/day; Prot: 1.1 ± 0.3 g/kg/day; Lip: 0.95 ± 0.1 g/kg/day Total fiber: 0.1 ± 0.1 g/kg/day Soluble fiber: NA Insoluble fiber: NA | Intervention eGFR (mL/min/1.73 m2) ** Basal: 110 (88–129) Final: 89.9 ± 4.1 Albuminuria (mg/24 h) ** Final: 10.4 (1.3–22.5) Control eGFR (mL/min/1.73 m2) Basal: 110 (88–129) Final: 105.6 ± 5.1 Albuminuria (mg/24 h) Final: 17.1 (4.1–44.5) |
| Type 2 diabetes | ||||
| Vegetarian diet | ||||
| Nicholson 1999 n = 11 USA | Females: 45.5% Hypertension: 81.8% Age: 54.3 (34–74) years HbA1c: 8.2 ± 1.5% BMI: NA Withdrawals: 15.4% Duration: 12-weeks | Randomized clinical trial | Intervention (n = 7): low fat vegan diet * Energy: 1409 ± 549 kcal/day CHO: 75 ± 4.4%; Prot: 14 ± 1.6%; Lip: 11 ± 4.7% Total fiber: 26 ± 8.2 g/day Soluble fiber: NA Insoluble fiber: NA Control (n = 4): conventional diet * Energy: 1526 ± 314 kcal/day CHO: 51 ± 3.5%; Prot: 18 ± 1.4%; Lip: 31 ± 2.4% Total fiber: 20 ± 2.7 g/day Soluble fiber: NA Insoluble fiber: NA | Intervention Albuminuria (mg/24 h) § Basal: 434.8 ± 565.5 Final: 155.2 ± 182.6 Control Albuminuria (mg/24 h) Basal: 82.9 ± 114.6 Final: 169.2 ± 298 |
| Mello 2006 n = 17 Brazil | Females: 17.6% Hypertension: 47% Age: 59 ± 11 years HbA1c: 7.6 ± 2.6% BMI: 26.2 ± 2.6 kg/m2 Withdrawals: 57.5% Duration: 4-weeks | Randomized crossover clinical trial Washout: 4-weeks | Intervention (n = 17): lactovegetarian diet * Energy: 1634 ± 451 kcal/day CHO: 58.7 ± 6.8%; Prot: 11.6 ± 1.5%; Lip: 29.5 ± 6.8% Total fiber: 27 ± 8.1 g/day Soluble fiber: NA Insoluble fiber: NA Control (n = 17): usual diet * Energy: 1901 ± 480 kcal/day CHO: 46.9 ± 6.7%; Prot: 21.9 ± 3.4%; Lip: 30.8 ± 6.3% Total fiber: 20±7.5 g/day Soluble fiber: NA Insoluble fiber: NA | Intervention eGFR (mL/min/1.73 m2) § Final: 81.9 ± 25.3 Albuminuria (mg/24 h) ** Final: 332.5 (111.1–1449) Control eGFR (mL/min/1.73 m2) Final: 81.8 ± 22.2 Albuminuria (mg/24 h) Final: 453.6 (324.4–1774.4) |
| Fiber supplement | ||||
| Dall’Alba 2013 n = 44 Brazil | Females: 38.6% Hypertension: 93.2% Age: 62 ± 9.7 years HbA1c: 6.9 ± 0.8% BMI: 29.8 ± 3.7 kg/m2 Withdrawals: 4.3% Duration: 6-weeks | Randomized clinical trial | Intervention (n = 23): 10 g guar gum supplement * Energy: 1700 ± 439 kcal/day CHO: 184.2 ± 28.1 g/day; Prot: 81.5 ± 15.4 g/day; Lip: 61.5 ± 10.2 g/day Total fiber: 24.3 ± 5.4 g/day Soluble fiber: 14.8 ± 1.9 g/day Insoluble fiber: 9.5 ± 3.6 g/day Control (n = 21): control group * Energy: 1553 ± 371 kcal/day CHO: 191.9 ± 27.3 g/day; Prot: 86.3 ± 12 g/day; Lip: 58.3 ± 12.8 g/day Total fiber: 15.7 ± 6.3 g/day Soluble fiber: 5.2 ± 1.9 g/day Insoluble fiber: 10.5 ± 4.7 g/day | Intervention eGFR (mL/min/1.73 m2) § Basal: 84.8 ± 16.6 Final: 85 ± 16.2 Albuminuria (mg/24 h) ‡ Basal: 6.8 (3–17.5) Final: 6.2 (3–9.5) Control eGFR (mL/min/1.73 m2) § Basal: 89.2 ± 16.7 Final: 89 ± 17.4 Albuminuria (mg/24 h) § Basal: 6.7 (3–19.3) Final: 7.6 (3–15.8) |
| Farhangi 2016 n = 49 Iran | Females: 100% Hypertension: NA Age: 48.3 ± 8.8 years HbA1c: 8.3 ± 0.9% BMI: 30.8 ± 3.9 kg/m2 Withdrawals: 9.3% Duration: 2-months | Randomized clinical trial | Intervention (n = 27): 10g chicory inulin supplement Energy: NA CHO: NA; Prot: NA; Lip: NA Total fiber: NA Soluble fiber: 10 g/day Insoluble fiber: NA Control (n = 22): placebo Energy: NA CHO: NA; Prot: NA; Lip: NA Total fiber: NA Soluble fiber: NA Insoluble fiber: NA | Intervention eGFR (mL/min/1.73 m2) § Basal: 86.3 ± 14 Final: 84.3 ± 13.6 Control eGFR (mL/min/1.73 m2) Basal: 85.3 ± 13.5 Final: 82.1 ± 16.1 |
| DASH diet | ||||
| Paula 2015 n = 40 Brazil | Females: 55% Hypertension: 100% Age: 62.2 ± 8.4 years HbA1c: 8.7 ± 1.8% BMI: 29.4 ± 3.4 kg/m2 Withdrawals: 0% Duration: 4-weeks | Randomized clinical trial | Intervention (n = 20): DASH diet * Energy: 1585 ± 321 kcal/day CHO: 47.1 ± 7.3%; Prot: 23.5 ± 6.7%; Lip: 29.4 ± 5.8% Total fiber: 20.1 ± 4.3 g/day Soluble fiber: 6.1 ± 2.1 g/day Insoluble fiber: 12.9 ± 2.9 g/day Control (n = 20): ADA recommendations * Energy: 1752 ± 299 kcal/day CHO: 39.3 ± 9.9%; Prot: 23 ± 3.8%; Lip: 36.8 ± 8% Total fiber: 14.1 ± 4.8 g/day Soluble fiber: 4.7 ± 2.1 g/day Insoluble fiber: 11 ± 5.3 g/day | Intervention Albuminuria (mg/24 h) § Basal: 41.6 (22.1–185.8) Final: 31.8 (10.2–132.7) ‡ Control Albuminuria (mg/24 h) Basal: 43.5 (18.5–194.4) Final: 33.4 (11.2–119.6) |
| Selection Bias | Performance Bias | Detection Bias | Attrition Bias | Reporting Bias | Other Bias | ||
|---|---|---|---|---|---|---|---|
| Random sequence generation | Allocation Concealment | Blinding of participant and personnel | Blinding of outcome assessment | Incomplete outcome data | Selective reporting | Diet/supplement adherence | |
| Jibani, 1991 | NA * | NA * | NA * | Uncertain | Low | Uncertain | Low |
| Kontessis, 1995 | Uncertain | Uncertain | NA * | Uncertain | Uncertain | Uncertain | Low |
| Nicholson, 1999 | Uncertain | Uncertain | NA * | Uncertain | Low | Uncertain | Low |
| Mello, 2006 | Uncertain | Uncertain | NA * | Uncertain | High | Uncertain | Low |
| Dall’Alba, 2013 | Low | Uncertain | High | Uncertain | Low | Low | Low |
| Paula, 2015 | Low | Uncertain | NA * | Uncertain | Low | Low | Low |
| Farhangi, 2016 | Low | Low | Low | Low | Low | High | Low |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mesquita de Carvalho, C.; Azevedo Gross, L.; Jobim de Azevedo, M.; Verçoza Viana, L. Dietary Fiber Intake (Supplemental or Dietary Pattern Rich in Fiber) and Diabetic Kidney Disease: A Systematic Review of Clinical Trials. Nutrients 2019, 11, 347. https://doi.org/10.3390/nu11020347
Mesquita de Carvalho C, Azevedo Gross L, Jobim de Azevedo M, Verçoza Viana L. Dietary Fiber Intake (Supplemental or Dietary Pattern Rich in Fiber) and Diabetic Kidney Disease: A Systematic Review of Clinical Trials. Nutrients. 2019; 11(2):347. https://doi.org/10.3390/nu11020347
Chicago/Turabian StyleMesquita de Carvalho, Cláudia, Luiza Azevedo Gross, Mirela Jobim de Azevedo, and Luciana Verçoza Viana. 2019. "Dietary Fiber Intake (Supplemental or Dietary Pattern Rich in Fiber) and Diabetic Kidney Disease: A Systematic Review of Clinical Trials" Nutrients 11, no. 2: 347. https://doi.org/10.3390/nu11020347