Dietary Interventions for Gout and Effect on Cardiovascular Risk Factors: A Systematic Review

 ,
,
Abstract
:1. Introduction
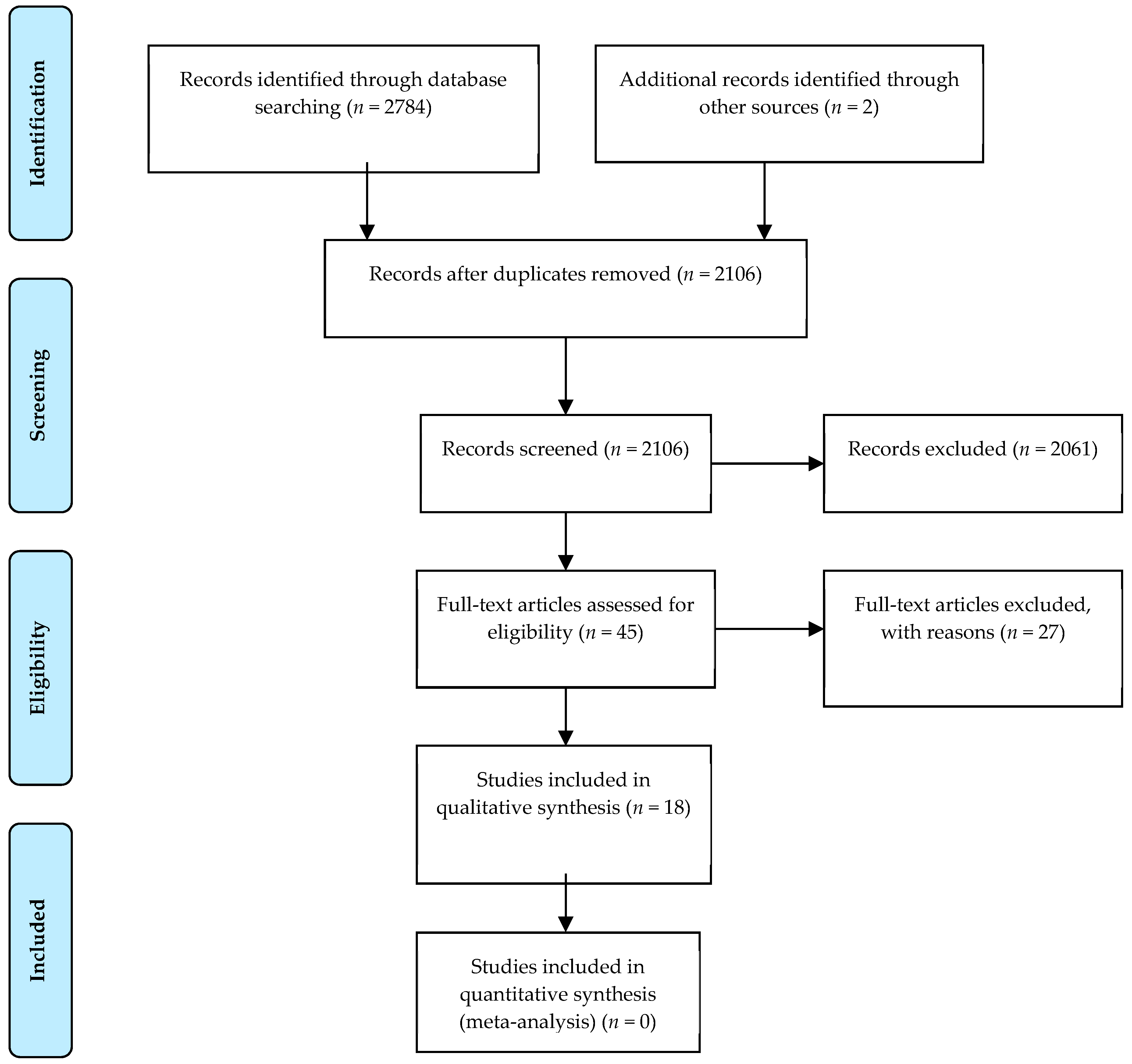
2. Materials and Methods
3. Results
3.1. Effect of Diet Interventions on Serum Uric Acid Level and Gout Flares
3.1.1. Calorie Restriction and Fasting
3.1.2. Purine-Low Diet
3.1.3. Mediterranean-Style Diets
3.1.4. Supplements
3.2. Diet Intervention and Changes in Cardiovascular Risk Factors
3.2.1. Calorie Restriction and Fasting
3.2.2. Purine-Low Diets
3.2.3. Mediterranean-Style Diets
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Kuo, C.F.; Grainge, M.J.; Zhang, W.; Doherty, M. Global epidemiology of gout: Prevalence, incidence and risk factors. Nat. Rev. Rheumatol. 2015, 11, 649–662. [Google Scholar] [CrossRef] [PubMed]
- Dalbeth, N.; Merriman, T.R.; Stamp, L.K. Gout. Lancet 2016, 388, 2039–2052. [Google Scholar] [CrossRef]
- Duskin-Bitan, H.; Cohen, E.; Goldberg, E.; Shochat, T.; Levi, A.; Garty, M.; Krause, I. The degree of asymptomatic hyperuricemia and the risk of gout. A retrospective analysis of a large cohort. Clin. Rheumatol. 2014, 33, 549–553. [Google Scholar] [CrossRef] [PubMed]
- MacFarlane, L.A.; Kim, S.C. Gout: A review of nonmodifiable and modifiable risk factors. Rheum. Dis. Clin. N. Am. 2014, 40, 581–604. [Google Scholar] [CrossRef] [PubMed]
- Rai, S.K.; Fung, T.T.; Lu, N.; Keller, S.F.; Curhan, G.C.; Choi, H.K. The Dietary Approaches to Stop Hypertension (DASH) diet, Western diet, and risk of gout in men: Prospective cohort study. BMJ 2017, 357. [Google Scholar] [CrossRef]
- Choi, H.K.; McCormick, N.; Lu, N.; Rai, S.K.; Yokose, C.; Zhang, Y. Population Impact Attributable to Modifiable Risk Factors for Hyperuricemia. Arthritis Rheumatol. 2019. [Google Scholar] [CrossRef]
- Andrés, M.; Bernal, J.A.; Sivera, F.; Quilis, N.; Carmona, L.; Vela, P.; Pascual, E. Cardiovascular risk of patients with gout seen at rheumatology clinics following a structured assessment. Ann. Rheum. Dis. 2017, 76, 1263–1268. [Google Scholar] [CrossRef]
- Janssens, H.J.; Arts, P.G.; Schalk, B.W.; Biermans, M.C. Gout and rheumatoid arthritis, both to keep in mind in cardiovascular risk management: A primary care retrospective cohort study. Jt. Bone Spine 2017, 84, 59–64. [Google Scholar] [CrossRef]
- Clarson, L.E.; Chandratre, P.; Hider, S.L.; Belcher, J.; Heneghan, C.; Roddy, E.; Mallen, C.D. Increased cardiovascular mortality associated with gout: A systematic review and meta-analysis. Eur. J. Prev. Cardiol. 2015, 22, 335–343. [Google Scholar] [CrossRef]
- Disveld, I.J.; Fransen, J.; Rongen, G.A.; Kienhorst, L.B.; Zoakman, S.; Janssens, H.J.; Janssen, M. Crystal-proven Gout and Characteristic Gout Severity Factors Are Associated with Cardiovascular Disease. J. Rheumatol. 2018, 45, 858–863. [Google Scholar] [CrossRef]
- Richette, P.; Doherty, M.; Pascual, E.; Barskova, V.; Becce, F.; Castaneda-Sanabria, J.; Coyfish, M.; Guillo, S.; Jansen, T.L.; Janssens, H.; et al. 2016 updated EULAR evidence-based recommendations for the management of gout. Ann. Rheum. Dis. 2017, 76, 29–42. [Google Scholar] [CrossRef] [PubMed]
- Torralba, K.D.; De Jesus, E.; Rachabattula, S. The interplay between diet, urate transporters and the risk for gout and hyperuricemia: Current and future directions. Int. J. Rheum. Dis. 2012, 15, 499–506. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed]
- Maclachlan, M.J.; Rodnan, G.P. Effect of food, fast and alcohol on serum uric acid and acute attacks of gout. Am. J. Med. 1967, 42, 38–57. [Google Scholar] [CrossRef]
- Scott, J.T.; Sturge, R.A. The effect of weight loss on plasma and urinary uric acid and lipid levels. Adv. Exp. Med. Biol. 1977, 76B, 274–277. [Google Scholar]
- Yamashita, S.; Matsuzawa, Y.; Tokunaga, K. Studies on the impaired metabolism of uric acid in obese subjects: Marked reduction of renal urate excretion and its improvement by a low-calorie diet. Int. J. Obes. 1986, 10, 255–264. [Google Scholar]
- Tinahones, F.J.; Soriguer, F.J.; Collantes, E.; Perez-Lindon, G.; Guijo, P.S.; Lillo, J.A. Decreased triglyceride levels with low calorie diet and increased renal excretion of uric acid in hyperuricaemic-hyperlipidaemic patients. Ann. Rheum. Dis. 1995, 54, 609–610. [Google Scholar] [CrossRef]
- Tinahones, J.F.; Perez-Lindon, G.; C-Soriguer, F.J.; Pareja, A.; Sanchez-Guijo, P.; Collantes, E. Dietary alterations in plasma very low density lipoprotein levels modify renal excretion of urates in hyperuricemic-hypertriglyceridemic patients. J. Clin. Endocrinol. Metab. 1997, 82, 1188–1191. [Google Scholar] [CrossRef]
- Dessein, P.H.; Shipton, E.A.; Stanwix, A.E.; Joffe, B.I.; Ramokgadi, J. Beneficial effects of weight loss associated with moderate calorie/carbohydrate restriction, and increased proportional intake of protein and unsaturated fat on serum urate and lipoprotein levels in gout: A pilot study. Ann. Rheum. Dis. 2000, 59, 539–543. [Google Scholar] [CrossRef]
- Habib, G.; Badarny, S.; Khreish, M.; Khazin, F.; Shehadeh, V.; Hakim, G.; Artul, S. The impact of ramadan fast on patients with gout. J. Clin. Rheumatol. 2014, 20, 353–356. [Google Scholar] [CrossRef]
- Peixoto, M.D.R.G.; Monego, E.T.; Jardim, P.C.B.V.; Carvalho, M.M.; Sousa, A.L.L.; Oliveira, J.S.D.; Balestra Neto, O. Diet and medication in the treatment of hyperuricemia in hypertensive patients. Arq. Bras. Cardiol. 2001, 76, 463–472. [Google Scholar] [CrossRef] [PubMed]
- Cardona, F.; Tinahones, F.J.; Collantes, E.; Garcia-Fuentes, E.; Escudero, A.; Soriguer, F. Response to a urate-lowering diet according to polymorphisms in the apolipoprotein AI-CIII-AIV cluster. J. Rheumatol. 2005, 32, 903–905. [Google Scholar] [PubMed]
- Holland, R.; McGill, N. Comprehensive dietary education in treated gout patients does not further improve serum urate. Intern. Med. J. 2015, 45, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Chatzipavlou, M.; Magiorkinis, G.; Koutsogeorgopoulou, L.; Kassimos, D. Mediterranean diet intervention for patients with hyperuricemia: A pilot study. Rheumatol. Int. 2014, 34, 759–762. [Google Scholar] [CrossRef]
- Zhang, M.; Gao, Y.; Wang, X.; Liu, W.; Zhang, Y.; Huang, G. Comparison of the effect of high fruit and soybean products diet and standard diet interventions on serum uric acid in asymptomatic hyperuricemia adults: An open randomized controlled trial. Int. J. Food Sci. Nutr. 2016, 67, 335–343. [Google Scholar] [CrossRef]
- Tang, O.; Miller, E.; Gelber, A.; Choi, H.; Appel, L.; Juraschek, S. DASH diet and change in serum uric acid over time. Clin. Rheumatol. 2017, 36, 1413–1417. [Google Scholar] [CrossRef]
- Juraschek, S.P.; White, K.; Tang, O.; Yeh, H.C.; Cooper, L.A.; Miller, E.R., III. Effects of a Dietary Approach to Stop Hypertension (DASH) Diet Intervention on Serum Uric Acid in African Americans with Hypertension. Arthritis Care Res. 2018, 70, 1509–1516. [Google Scholar] [CrossRef]
- Dalbeth, N.; Ames, R.; Gamble, G.D.; Horne, A.; Wong, S.; Kuhn-Sherlock, B.; MacGibbon, A.; McQueen, F.M.; Reid, I.R.; Palmano, K. Effects of skim milk powder enriched with glycomacropeptide and G600 milk fat extract on frequency of gout flares: A proof-of-concept randomised controlled trial. Ann. Rheum. Dis. 2012, 71, 929–934. [Google Scholar] [CrossRef]
- Stamp, L.K.; O’Donnell, J.L.; Frampton, C.; Drake, J.M.; Zhang, M.; Chapman, P.T. Clinically insignificant effect of supplemental vitamin C on serum urate in patients with gout: A pilot randomized controlled trial. Arthritis Rheum. 2013, 65, 1636–1642. [Google Scholar] [CrossRef]
- Kubomura, D.; Yamada, M.; Masui, A. Tuna extract reduces serum uric acid in gout-free subjects with insignificantly high serum uric acid: A randomized controlled trial. Biomed. Rep. 2016, 5, 254–258. [Google Scholar] [CrossRef]
- Azzeh, F.S.; Al-Hebshi, A.H.; Al-Essimii, H.D.; Alarjah, M.A. Vitamin C supplementation and serum uric acid: A reaction to hyperuricemia and gout disease. PharmaNutrition 2017, 5, 47–51. [Google Scholar] [CrossRef]
- Yamanaka, H. Essence of the revised guideline for the management of Hyperuricemia and gout. Jpn. Med. Assoc. J. 2012, 55, 324–329. [Google Scholar]
- Jordan, K.M.; Cameron, J.S.; Snaith, M.; Zhang, W.; Doherty, M.; Seckl, J.; Hingorani, A.; Jaques, R.; Nuki, G. British Society for Rheumatology and British Health Professionals in Rheumatology guideline for the management of gout. Rheumatology 2007, 46, 1372–1374. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.K. A prescription for lifestyle change in patients with hyperuricemia and gout. Curr. Opin. Rheumatol. 2010, 22, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Obarzanek, E.; Sacks, F.M.; Vollmer, W.M.; Bray, G.A.; Miller, E.R.; Lin, P.H.; Karanja, N.M.; Most-Windhauser, M.M.; Moore, T.J.; Swain, J.F.; et al. Effects on blood lipids of a blood pressure-lowering diet: The Dietary Approaches to Stop Hypertension (DASH) Trial. Am. J. Clin. Nutr. 2001, 74, 80–89. [Google Scholar] [PubMed]
- Choi, H.K.; Atkinson, K.; Karlson, E.W.; Willett, W.; Curhan, G. Purine-rich foods, dairy and protein intake, and the risk of gout in men. N. Engl. J. Med. 2004, 350, 1093–1103. [Google Scholar] [CrossRef]
- Teng, G.G.; Pan, A.; Yuan, J.M.; Koh, W.P. Food Sources of Protein and Risk of Incident Gout in the Singapore Chinese Health Study. Arthritis Rheumatol. 2015, 67, 1933–1942. [Google Scholar] [CrossRef]
- Vieira, A.T.; Galvão, I.; Macia, L.M.; Sernaglia, E.M.; Vinolo, M.A.R.; Garcia, C.C.; Tavares, L.P.; Amaral, F.A.; Sousa, L.P.; Martins, F.S.; et al. Dietary fiber and the short-chain fatty acid acetate promote resolution of neutrophilic inflammation in a model of gout in mice. J. Leukoc. Biol. 2017, 101, 275–284. [Google Scholar] [CrossRef]
- Appel, L.J.; Moore, T.J.; Obarzanek, E.; Vollmer, W.M.; Svetkey, L.P.; Sacks, F.M.; Bray, G.A.; Vogt, T.M.; Cutler, J.A.; Windhauser, M.M.; et al. A clinical trial of the effects of dietary patterns on blood pressure. DASH Collaborative Research Group. N. Engl. J. Med. 1997, 336, 1117–1124. [Google Scholar] [CrossRef]
- Fung, T.T.; Chiuve, S.E.; McCullough, M.L.; Rexrode, K.M.; Logroscino, G.; Hu, F.B. Adherence to a DASH-style diet and risk of coronary heart disease and stroke in women. Arch. Intern. Med. 2008, 168, 713–720. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| First Author Year Journal | Study-Design Population (n) Groups/Control | Intervention Duration | Serum Uric Acid (SUA) Baseline mg/dL | SUA End mg/dL | Change | Remarks | ||
|---|---|---|---|---|---|---|---|---|
| Intervention | Control | Intervention | Control | p-Value | ||||
| Machlachlan [14] 1967 American Journal of Medicine | Pilot study n = 9 (1♀) with gout Age ♀47/♂39–67 Control group: n = 2 normouricemic, non-gouty men |
| 7.2–13.9 | 4.1–5.0 | Not applicable (na) | na |
| No standard deviations (SDs) and p-values, patients were discussed individually. Results are average ranges. After fasting, SUA increased and returned to near baseline values within 24 h. |
| Scott [15] 1977 Advances in Experimental Medicine and Biology | Pilot study n = 35 (11♀) with obesity (defined as 10% above ideal weight) some with gout Control group: no | Low carbohydrate diet with 1 week low-purine (<200 mg) and alcohol-free diet before baseline measurements, Duration: until adequate weight loss | 6.96 | 6.27 | −0.69 p = 0.000025 | Association between reduction of total cholesterol (TC) and SUA (r = 0.62, p = 0.004). | ||
| Yamashita [16] 1986 International Journal of Obesity | Pilot study n = 27 (16♀) Japanese patients BMI >26 kg/m2 some with gout Mean age ♀37/♂32 Control group: subjects with healthy weight | 1500–800 kcal diet (stepwise reduction) Duration: 4–14 weeks | ♂ 9.2 ± 1.9 ♀ 6.8 ± 1.9 | ♂ 5.1 ± 0.8 ♀ 4.4 ± 1.0 | ♂ 7.4 ± 1.6 ♀ 5.5 ± 0.9 | na | p < 0.01 | Size of control group unknown. ‘Overweight’ defined as 130% of ‘ideal weight’ (recalculated≈ BMI = 26 kg/m2). p-value: when compared with baseline values (in-group). |
| Tinahones [17,18] 1995/1997 Annals of the Rheumatic Diseases/Journal of Clinical Endocrinology and Metabolism | Pilot study n = 36 (0♀) Age 36–52 Group 1: SUA >7.0 mg/dL Group 2: SUA >7.0 mg/dL and triglycerides >2.26 mmol/L | 1200 kcal diet 3 weeks | (1) 8.68 ± 1.7 (2) 8.78 ± 2.8 | na | (1) 8.05 ± 1.4 (2) 7.5 ± 1.9 | na | (1) −0.63 not significant (ns) (2) −1.28 ns | |
| Dessein [19] 2000 Annals of the Rheumatic Diseases | Pilot study n = 13 (0♀) Age 38–62 with ≥2 gout flares in the last 4 months, without tophi Control group: no | 1600 kcal diet (The Zone Diet), 40 en% carbohydrates, 30 en% protein, 30 en% fat, no purine restriction 16 weeks | 9.66 ± 1.7 | na | 7.97 ± 1.5 | na | −1.69 p = 0.001 | Number of self-reported monthly attacks was a primary outcome measure. Monthly attacks decreased from 2.1 ± 0.8 to 0.6 ± 0.7 (p = 0.002). |
| Habib [20] 2014 Journal of Clinical Rheumatology | Prospective cohort n = 43 (2♀) Age 32–82 diagnosed with gout Control group: No fasting | Ramadan: fasting including no drinking from sunrise to sunset 1 month | 7.92 ± 1.69 | 7.6 ± 1.6 | 8.11 ± 1.84 | 7.4 ± 1.8 | 0.19 p = 0.999 | Change and p-value: when compared with baseline values (in-group). |
| First Author Year Journal | Study-Design Population (n) Groups/Control | Intervention Duration | SUA Baseline mg/dL | SUA End mg/dL | Change | Remarks | ||
|---|---|---|---|---|---|---|---|---|
| Intervention | Control | Intervention | Control | p-Value | ||||
| Peixoto [21] 2001 Arquivos Brasileiros de Cardiologia | Randomized controlled trial (RCT) n = 60 (31♀), n = 55 completed the study Age 30–75 (mean: 54.4 ± 10.6) with SUA ♂ ≥8.5 mg/dL ♀ ≥7.5 mg/dL | 3 groups
| 1. 8.64 ± 1.09 | 2. 9.36 ± 0.89 3. 9.05 ± 1.23 | 1. 7.40 ± 1.27 | 2. 6.88 ± 1.72 3. 6.66 ± 1.73 | 1. −1.24, p < 0.001 2. −2.48, p < 0.001 3. −2.42, p < 0.001 | Delta’s and p-values: within group changes. Between 12 and 24 weeks SUA in group 1 further decreased to 6.55 ± 2.25 (p < 0.001) and increased in groups 2 and 3 (p-value when compared to baseline <0.05). |
| Cardona [22] 2005 The Journal of Rheumatology | Pilot study n = 64 (0♀) Mean age 50 with gout according to ACR criteria, no medication for gout, hyperlipidemia, hypertension, diabetes Control group: no | Purine-low diet: no meat, poultry, fish, seafood, alcohol, beans, peas, lentils, spinach, oatmeal, asparagus 2 weeks | 7.7 ± 1.7 | na | 7.13 | na | –0.57 ± 1.7 p = 0.01 | SD end measurement not available. |
| Holland [23] 2015 Internal Medicine Journal | RCT n = 29 (2♀, 28 completed the study) Australian patients with gout according to ACR criteria, stable on urate lowering therapy with SUA <6.05 mg/dL Age intervention group (n = 14, 2♀) 64 (44–80) Age control group (n = 16, 0♀) 61 (38–77) | Control group: general advice, compliance medication, weight loss, exercise, alcohol, target SUA Intervention group (in addition to intervention control group): additional dietary education 1 consult + follow up after 6 months | 4.88 ± 1.3 | 4.88 ± 1.0 | 5.04 ± 1.2 | 4.54 ± 1.2 | 0.16 in group 0.50 between group (p > 0.05) | |
| First Author Year Journal | Study-Design Population (n) Groups/Control | Intervention Duration | SUA Baseline mg/dL | SUA End mg/dL | Change | Remarks | ||
|---|---|---|---|---|---|---|---|---|
| Intervention | Control | Intervention | Control | p-Value | ||||
| Chatzipavlou [24] 2013 Rheumatology International | Pilot study n = 12, (6 completed the study, 1♀) Greek patients with asymptomatic hyperuricemia (SUA ♀ >5.7 mg/dL ♂ >7.0 mg/dL) Mean age 53 Control group: no | Cretan Mediterranean diet, high in MUFAs, legumes, cereals/bread, fruit, and vegetables; moderate in alcohol and dairy and low in meat. 8 weeks with additional measurements at 12 and 24 weeks | 9.12 (8.2–13.8) | na | 8 week: 6.2 (5.5–7.8) 24 week: 6.13 (na) | na | −2.92 p = na | SUA: averages for 6 patients with (ranges). |
| Zhang [25] 2016 International Journal of Food Sciences and Nutrition | RCT n = 187 (94♀) Chinese patients with asymptomatic hyperuricemia (SUA ♀ >6.0 mg/dL ♂ >7.0 mg/dL) Age 20–59 Control group: standard diet for hyperuricemia | Diet high in fruits and soybean products. 12 weeks | 7.71 ± 1.0 | 7.62 ± 1.0 | 6.61 ± 13.3 | 6.62 ± 1.2 | no difference between groups intervention group: −1.0, p < 0.001 control group: −1.0, p < 0.001 | Standard diet for hyperuricemia: restricted energy, fat, and animal protein intake (especially red meat and seafood), less salt restriction, increased intake of soybean products, fruits and vegetables, limiting alcohol or strong tea intake, increase water intake, and moderate intake of sweet fruits and seafood. |
| Tang [26] 2017 Clinical Rheumatology | RCT (crossover trial) n = 24 (subgroup of total 103 patients with (pre) ]hypertension, 34%♀) patients SUA ≥6.0 mg/dL Age 41–61 Control group: typical American diet | DASH with 3 sodium levels 90 days | 6.6 (6.3, 6.9) | 6.7 (6.3, 7.1) | 5.6 (4.9, 6.3) | 6.6 (5.9, 7.3) | −1.02 (−2.0, −0.1) p = 0.03 | SUA: mean with (95% CI) |
| Juraschek [27] 2018 Arthritis Care Res (Hoboken) | RCT (ancillary study) n = 117 (55% with SUA >6 mg/dL, 70%♀) African Americans with controlled hypertension Age 59 ± 9.5 Control group: DASH brochure and $30/week to purchase foods | DASH-plus: coach-directed dietary advice, assistance with purchasing DASH-related foods ($30/week), and home food delivery via a community supermarket 8 weeks | 6.51 ± 1.45 | 6.18± 1.89 | 6.58 ± 1.35 | 6.25 ± 1.86 | Change between groups −0.01 (95% CI −0.39, 0.38) p = 0.98 | Significant trend toward greater reduction in SUA among those with a higher SUA levels at baseline (p = 0.008 for trend) |
| First Author Year Journal | Study-Design Population (n) Groups/Control | Intervention Duration | SUA Baseline mg/dL | SUA End mg/dL | Change mg/dL | Remarks | ||
|---|---|---|---|---|---|---|---|---|
| Intervention | Control | Intervention | Control | p-Value | ||||
| Dalbeth [28] 2012 Annuals of Rheumatic Disease | Randomized double-blind controlled trial, n = 120 (16♀), New Zealand, patients with gout, >2 flares in last 4 months. |
| 1. 6.9 ± 1.5 2. 7.1 ± 1.8 | 3. 7.4 ± 1.8 | na | na | p(group) = 0.15 p(time) = 0.27 p(interaction) = 0.89 | Frequency of gout flares decreased significantly in all 3 groups. |
| Stamp [29] 2013 Arthritis & Rheumatism | Open label, parallel group, randomized controlled trial n = 40, (4♀) New Zealand, patients with gout, SUA >6 mg/dL, n = 20 without ULT (group 1 and 2) and n = 20 already on ULT (group 3 and 4) |
| 1 + 4: 8.4 ± 1.8 | 2 + 3: 8.4 ± 1.5 | na | na | 1: −0.07 ± 0.4 2: −2.5 ± 0.4 p < 0.001 3: −1.5 ±0.4 4: −0.5 ± 0.4 p < 0.029 | |
| Kubomura [30] 2016 Biomedical Reports | Double blind placebo controlled RCT n = 48, (0♀) Japanese patients with asymptomatic hyperuricemia (SUA 6.5–8.0 mg/dL) not on urate lowering therapy Age 20–64Control group: placebo | Tuna extract supplement
| 1. 7.2 ± 0.1 2. 7.2 ± 0.1 | 7.1 ± 0.1 | 1. 6.97 2. 6.86 | 7.03 | In group change 1. −0.23 2. −0.34 p-value not given | In group change 0–6 weeks in high dose group −0.49 mg/dL and +0.14 mg/dL in placebo group (p < 0.05). |
| Azzeh [31] 2017 Pharma- Nutrition | Pilot study n = 25 (14♀) Saudi patients not on urate lowering therapy of whom 15 (6♀) with gout (group 1, age 53, BMI 31 kg/m2) and 15 (8♀) with hyperuricemia (group 2, age 54, BMI 33 kg/m2) Control group: no | 500 mg vitamin C chewable tablet daily 8 weeks | 1. 8.09 ± 1.09 2. 7.94 ± 0.93 | 1. 8.4 ± 1.15 2. 7.16 ± 1.04 | 1. 0.31 ± 0.14 (ns) 2. −0.78 ± 0.3 (p < 0.05) | |||
| Yamanaka [32] 2018 Modern Rheumatology | Double blind placebo controlled RCT n = 25, (0♀) Japanese patients with asymptomatic hyperuricemia (SUA ≥7 mg/dL) not on urate lowering therapy Age 59–70 Control group: placebo (same yoghurt 2 × 100 g/day without PA-3) | PA-3Y (PA-3-containing yoghurt) 2 × 100 g/day fermentation with strains of Lactobacillus delbrueckii ssp. and Streptococcus thermophilus (n = 13) 8 weeks | 8.7 ± 1.0 | 8.5 ± 0.9 | 8.7 ± 1.2 | 8.7 ± 1.1 | No change (no difference between groups) | In group change intervention group: +0.1 ± 0.8mg/dL, in group change control group: +0.1 ± 0.7mg/dL |
| First Author Year | Blood Pressure in mm/Hg | Total Cholesterol in mmol/L | Triglycerides in mmol/L | High Density Lipoprotein (HDL) in mmol/L | Low Density Lipoprotein (LDL) in mmol/L | Glucose in mmol/L | Weight in Kg or Body Mass Index (BMI) in kg/m2 |
|---|---|---|---|---|---|---|---|
| Scott [15] 1977 | - | baseline: 6.3 end: 6.0 p = 0.03 | baseline: 2.1 end: 1.5 (p = 0.03) | - | - | - | mean weight loss 7 kg (range weight loss 1.6–12.3 kg) |
| Yamashita [16] 1986 | - | - | - | - | - | - | weight loss (% of baseline weight) ♂ 7.8 ± 2.4% ♀6.9 ± 2.1% |
| Tinahones [17,18] 1995/1997 | - | 1. baseline 5.2 ± 1.2; end 4.5 ± 0.9 (p < 0.05) 2. baseline 6.2 ± 1.1; end 5.3 ± 1.4 | 1. baseline 1.4 ± 0.5; end 1.1 ± 0.4 2. baseline 4.2 ± 3.8; end 1.7 ± 1.5 (p < 0.001) | 1. baseline 1.1 ± 0.3; end 1.0 ± 0.2 2. baseline 0.9 ± 0.2; end 1.0 ± 0.3 (p < 0.05) | - | - | 1. baseline 83.8 ± 9; end 79.8 ± 8 kg 2. baseline 85.5 ± 13; end 80.6 ± 13 kg |
| Dessein [19] 2000 | - | Baseline 6.0 ± 1.7; end 4.7 ± 0.9 (p = 0.002) | Baseline 4.7 ± 4.2; end 1.9 ± 1.0 (p = 0.001) | Baseline 0.87 ± 0.21; end 0.91 ± 0.16 (p = 0.5) | Baseline 3.5 ± 1.2; end 2.7 ± 0.8 (p = 0.004) | - | Baseline BMI 30.5 ± 8.1; end 27.8 ± 7.9 kg/m2 (p = 0.002) |
| Habib [20] 2014 | - | - | - | - | - | - | Ramadan group: baseline BMI 30.5 ± 5.8, end 31.0 ± 5.6 kg/m2; No Ramadan group: baseline BMI 29.8 ± 4.8, end 30.2 ± 5.2 kg/m2 |
| Peixoto [21] 2001 | 1. baseline 150 ± 22.6/102 ± 17.3; end 133 ± 21.7/92 ± 12 (p < 0.05) 2. baseline 140 ± 21.3/95 ± 11.1; end 140 ± 20.0/95 ± 13.1 3. baseline 141 ± 23.6/92 ± 14.8; end 140 ± 19.1/93 ± 10.6 | 1. baseline 5.8 ± 1.3; end 6.1 ± 1.1 2. baseline 5.9 ± 1.5; end 6.4 ± 0.9 3. baseline 6.0 ± 1.5; end 6.1 ± 1.4 | 1. baseline 2.5 ± 0.9; end 2.6 ± 0.8 2. baseline 3.2 ± 1.3; end 3.7 ± 1.5 3. baseline 2.6 ± 1.9; end 2.4 ± 1.1 | - | - | 1. baseline 5.8 ± 1.0; end 5.9 ± 0.7 2. baseline 5.5 ± 1.0; end 5.5 ± 0.8. 3. baseline 5.8 ± 1.1; end 5.4 ± 0.8. | 1. baseline 28.7 ± 4.2; end 28.7 ± 3.9. 2. baseline 28.4 ± 3.1; end 28.0 ± 3.0. 3. baseline 28.5 ± 4.7; end 28.2 ± 4.7 |
| Cardona [22] 2005 | - | Baseline 5.5 ± 1.0; change (2 weeks) −0.3 ± 0.8 p < 0.001 | Baseline 2.8 ± 2.5; change (2 weeks) −0.8 ± 1.8 p < 0.001 | - | - | Baseline 6.0 ± 1.1; change (2 weeks) -0.3 ± 0.7 p < 0.001 | Baseline 30.2 ± 3.8, no significant change |
| Chatzipavlou [24] 2013 | - | Average TC at baseline and 24 weeks (n = 6): 5.7 and 5.4 | Average triglycerides at baseline and 24 weeks (n = 6): 1.8 and 1.3 | Average HDL at baseline and 24 weeks (n = 6): 1.3 and 1.4 | Average LDL at baseline and 24 weeks (n = 6): 3.5 and 3.2 | - | BMI baseline 31.46 (range 28.2–37.3), at 8 weeks 29.4 (range 26–34.2) kg/m2, change −2.1 kg/m2 (n = 6) |
| Zhang [25] 2016 | 1. baseline 120.53 ± 11.58/78.29 ± 9.18; end 120.35 ± 13.05/77.18 ± 9.17 2. baseline 121.19 ± 14.07/77.87 ± 8.92; end 121.75 ± 15.33/77.26 ± 8.86 | 1. baseline 5.26 ± 1.05; end 5.08 ± 0.87 (p < 0.05) 2. baseline 5.20 ± 0.88; end 5.23 ± 0.88 | 1. baseline 1.75 ± 1.12; end 1.58 ± 0.89 (p < 0.05) 2. baseline 1.91 ± 1.26; end 1.85 ± 1.33 | 1. baseline 1.39 ± 0.36; end 1.41 ± 0.33 2. baseline 1.33 ± 0.35; end 1.41 ± 0.30 (p < 0.05) | 1. baseline 3.05 ± 0.81; end 2.98 ± 0.73 2. baseline 3.03 ± 0.75; end 3.06 ± 0.71 | 1. baseline 5.45 ± 0.87; end 5.45 ± 0.55 2. baseline 5.33 ± 0.56; end 5.48 ± 0.48 | 1. baseline: 25.5 ± 3.4; end 25.0 ± 3.2 kg/m2 (p < 0.05) 2. baseline 25.2 ± 2.8; end 25.1 ± 2.8 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vedder, D.; Walrabenstein, W.; Heslinga, M.; de Vries, R.; Nurmohamed, M.; van Schaardenburg, D.; Gerritsen, M. Dietary Interventions for Gout and Effect on Cardiovascular Risk Factors: A Systematic Review. Nutrients 2019, 11, 2955. https://doi.org/10.3390/nu11122955
Vedder D, Walrabenstein W, Heslinga M, de Vries R, Nurmohamed M, van Schaardenburg D, Gerritsen M. Dietary Interventions for Gout and Effect on Cardiovascular Risk Factors: A Systematic Review. Nutrients. 2019; 11(12):2955. https://doi.org/10.3390/nu11122955
Chicago/Turabian StyleVedder, Daisy, Wendy Walrabenstein, Maaike Heslinga, Ralph de Vries, Michael Nurmohamed, Dirkjan van Schaardenburg, and Martijn Gerritsen. 2019. "Dietary Interventions for Gout and Effect on Cardiovascular Risk Factors: A Systematic Review" Nutrients 11, no. 12: 2955. https://doi.org/10.3390/nu11122955