Whole Grains, Refined Grains, and Cancer Risk: A Systematic Review of Meta-Analyses of Observational Studies


College of Health Solutions, Arizona State University, Phoenix, AZ 85004, USA
Nutrients 2020, 12(12), 3756; https://doi.org/10.3390/nu12123756
Submission received: 5 October 2020
/
Revised: 1 December 2020
/
Accepted: 2 December 2020
/
Published: 7 December 2020
(This article belongs to the Special Issue Grains and Human Health)
Abstract
:PubMed, Web of Science, and the Cochrane Database of Systematic Reviews were searched for meta-analyses that provided risk estimates (±95% confidence intervals) for associations between intakes of whole and refined grains and risk of total and site-specific cancer. The preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines were followed. Only meta-analyses that included whole grains and refined grains as separate food groups, and not as part of dietary patterns, were included. A total of 17 publications were identified that met inclusion criteria. Within these, results from a total of 54 distinct meta-analyses were reported for whole grains and 5 meta-analyses for refined grains. For total cancer mortality, 7 meta-analyses of cohort studies indicated that whole grain intake was associated with 6% to 12% lower risk in comparison of highest vs. lowest intake groups, and 3% to 20% lower risk for doses ranging from 15 to 90 g/day. For site-specific cancers, meta-analyses indicated that whole grain intake was consistently associated with lower risks of colorectal, colon, gastric, pancreatic, and esophageal cancers. Limited data were available for refined grains, with only 4 publications providing risk estimates, and only 1 of the meta-analyses included more than 3 studies. High intake of refined grains was associated with increased risk of colon and gastric cancer. By contrast, in the only dose-response meta-analysis, each 90 g/day consumption of refined grains was associated with a 6% lower risk of total cancer. In addition to the limited number of published meta-analyses on refined grains, results were also weakened due to the fact that refined grains were frequently defined to include both staple grain foods and indulgent grain foods, and the majority of studies included in the meta-analyses provided no specific definition of refined grains. Overall, meta-analyses of cohort and case-control studies consistently demonstrate that whole grain intake is associated with lower risk of total and site-specific cancer, and support current dietary recommendations to increase whole grain consumption. By contrast, the relationship between refined grain intake and cancer risk is inconclusive.
1. Introduction
Whole grains are associated with reduced risk of a number of chronic diseases, including cancer, and are recommended as an important part of a healthy diet [1,2,3]. By contrast, refined grains do not have similarly beneficial inverse associations between consumption and disease risk [4,5,6]. Consequently, dietary guidelines encourage increased consumption of whole grains and reduced consumption of refined grains [3]. The American Association of Cereal Chemists defined whole grains as consisting of the “intact, ground, cracked or flaked caryopsis, whose principal anatomical components—the starchy endosperm, germ and bran—are present in the same relative proportions as they exist in the intact caryopsis” [7]. This definition was adopted by regulatory and health promotion organizations to encourage greater consumption of whole grain foods [8]. Refined grains have some or all of the bran layers removed during processing, which reduces the content of fiber and micronutrients [8]. In research studies, whole grain and refined grain intake is assessed in terms of consumption of grain-based foods which may contain varying percentages of whole grains and refined grains, and definitions vary among studies [5,8]. In addition, grains may be consumed as a single food or as an ingredient in foods [9].
Much of the published research used to inform dietary guidelines comes from cohort studies that have examined the association between dietary patterns and risk of various chronic diseases [10]. A healthy dietary pattern typically includes whole grains, fruits, vegetables, fish, legumes, nuts, and low-fat dairy products. In contrast, an unhealthy dietary pattern, also widely referred to as a Western dietary pattern, is characterized by consumption of red and processed meat, sugar-sweetened foods and beverages, French fries, high-fat dairy products, and refined grains. With regard to cancer, the healthy dietary pattern is frequently associated with reduced risk and the Western dietary pattern is usually associated with increased risk [11,12,13,14,15]. However, dietary patterns do not allow for the contribution to cancer risk of specific food groups, such as whole and refined grain foods. Limitations of dietary pattern research, particularly with respect to interpretation of health outcomes associated with refined grain intake, has been reviewed recently [5]. For example, within the Western dietary pattern, consumption of red and processed meat is associated with increased risk of colorectal cancer and all-cause mortality, but consumption of refined grains is not [16,17].
Therefore, the objective of this review was to summarize the published research on the association between whole grain intake and cancer risk and between refined grain intake and cancer risk (including incidence and mortality). The review focuses exclusively on results from meta-analyses of observational cohort and case-control studies of adults in which whole grains and refined grains were evaluated as distinct food categories and not as part of dietary patterns.
2. Materials and Methods
The preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines were used for this review [18]. The Institute for Scientific Information’s Web of Science, PubMed, and the Cochrane Database of Systematic Reviews were used to identify relevant meta-analyses, and were searched from database inception until September 1, 2020. The search strategy included the following terms: “Whole grain” OR “wholegrain” OR “whole-grain” OR “whole grains” OR “wholegrains” OR “whole-grains” OR “refined grain” OR “refined grains” AND “cancer”. Search results were further filtered by “meta-analysis”, “systematic review”, or “review”. No restrictions were placed on date of publication. Only English language publications were considered. Reference lists and electronic citation records of all identified meta-analyses were also reviewed for additional meta-analyses not found in the initial searches. Meta-analyses of cohort and/or case-control studies were included in this review if they provided relative risks or odds ratios with 95% confidence intervals, for total or site-specific cancer risk associated with either whole grain or refined grain intake. Whole grain and refined grain intake had to be considered as separate food groups, and not as part of a dietary pattern. Meta-analyses that included whole grains or refined grains as part of dietary patterns were excluded.
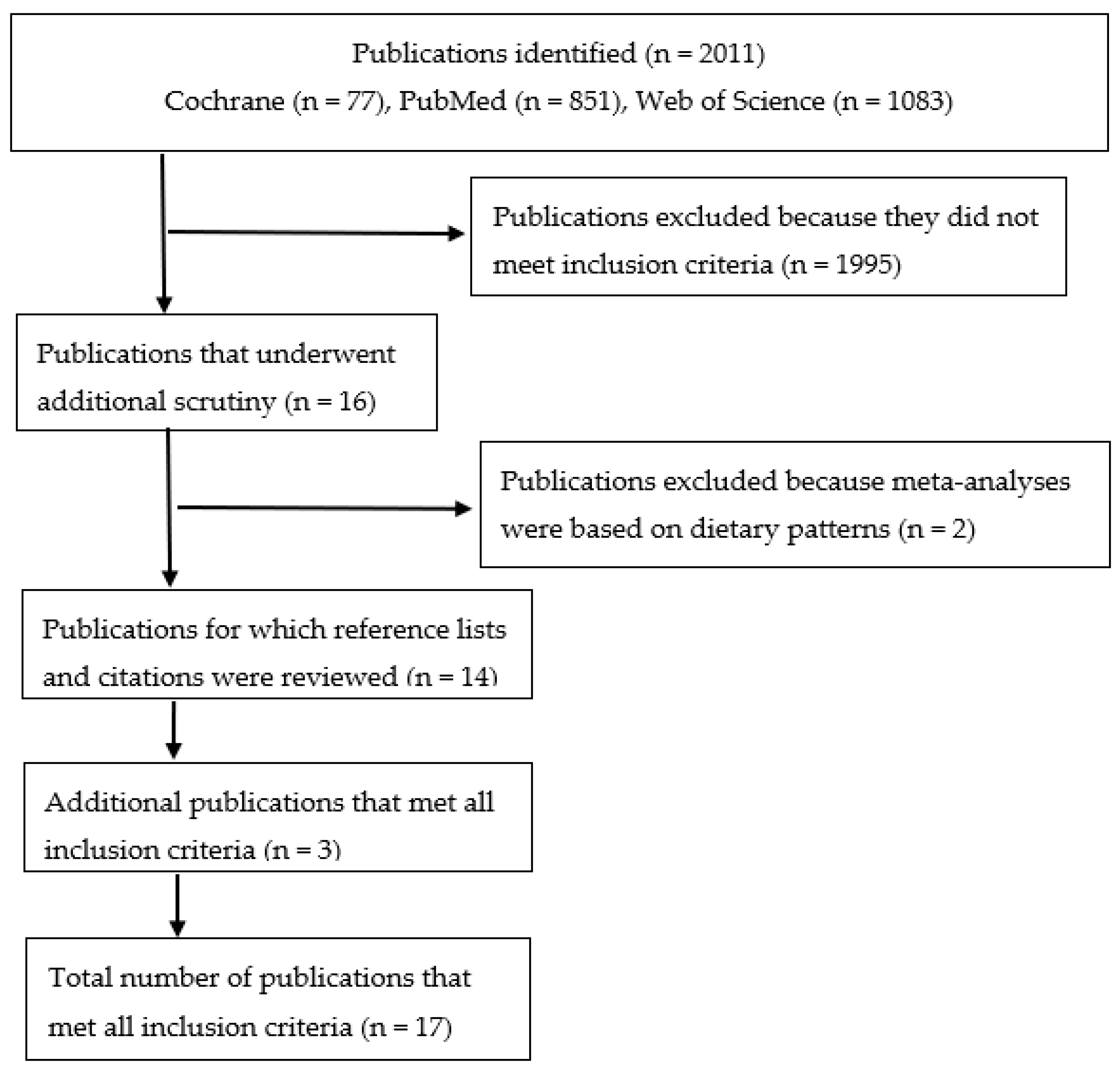
The flow chart for publication selection is presented in Figure 1. The initial searches identified 77 (Cochrane), 851 (PubMed), and 1083 (Web of Science) articles. After further restricting those searches using the filters described above, 16 publications were found that underwent additional scrutiny to ensure that they met the inclusion criteria [16,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33]. Two of the publications were excluded because some or all of the studies used in those meta-analyses included whole grains as part of a dietary pattern [23,27]. Review of reference lists and electronic citation records of each of the meta-analyses identified in the search revealed three additional publications that met inclusion criteria [34,35,36]. Thus, a total of 17 publications, each with 1 or more meta-analyses included in the publication, were used in the current review.
3. Results
Details of the meta-analyses, including information on the number of cohort and case-control studies included, total number of participants, and results of publication bias and heterogeneity assessments, are presented in Supplementary Table S1. Details on each of the studies used in the meta-analyses for whole grains and refined grains, including cohort and case-control populations, method of dietary assessment, and definition of whole grains and refined grains, are presented in Supplementary Tables S2 and S3, respectively.
All cohort studies were from the United States and Europe (United Kingdom, Norway, Sweden, Denmark, Finland, Spain) (Supplemental Tables S2 and S3). Cohorts included men and women aged 30–87 years at baseline, and ranged in size from 7216 to 489,611 participants. The case-control studies mainly included populations from the United States and Europe (Italy, Germany, Poland, Sweden, The Netherlands, Belgium, Switzerland, Greece, Spain), but also from Asia (China, Japan, South Korea, India), the Middle East (Jordan, Iran), South America (Brazil, Uruguay), Canada, and Australia (Supplemental Tables S2 and S3). Case-control studies included fewer participants, with most studies including fewer than 1000 cases and controls. Publication bias was assessed in all but two of the meta-analyses, mostly by using Egger’s [37] or Begg’s [38] tests, while one used the risk of bias in systematic reviews ROBIS assessment tool [39]. In all but one meta-analysis [32], no significant bias was detected (Supplementary Table S1). Heterogeneity was assessed with the I2 statistic [40]. Twenty-one of the meta-analyses reported statistically significant heterogeneity in their meta-analyses, with I2 between 53% and 91% (Supplementary Table S1).
3.1. Whole Grain Intake and Total Cancer Risk
Eight meta-analyses have been published on the relationship between whole grain intake and either cancer mortality [20,21,22,26,29,31,33] or total cancer risk [24] (Table 1). Seven of the meta-analyses used data entirely [20,21,22,26,29,33] or predominantly [31] from cohort studies, and reported relative risks for total cancer mortality. One used only case-control studies [24], and reported on total cancer risk from multiple sites combined. All 8 of the meta-analyses provided risk estimates for categorial analyses (highest vs. lowest intakes), and 7 reported risk estimates for dose-response analyses. In virtually all instances, whole grain intake was associated with significantly lower cancer risk in both highest intake vs. lowest intake analyses and in dose-response analyses (Table 1). For the meta-analyses of cohort studies, high intake of whole grains was associated with a 6% to 12% lower risk of cancer mortality [20,21,22,26,29,31,33]. In the dose-response analyses, doses between 50 and 90 g/day were associated with a 9% to 20% lower cancer mortality risk [20,21,22,29,33]. Doses in the range of 15 to 30 g/day were associated with risk reductions of 3% to 11% [26,31,33]. Collectively, the 7 dose-response analyses presented in Table 1 indicate that each 30 g/day intake of whole grains (~1 serving) is associated with a ~7% reduction in cancer mortality risk.
In the one meta-analysis that relied solely on case-control studies [24], a pooled analysis of 40 case-control studies (Table 1) indicated that when comparing the highest vs. lowest intake of whole grains, the highest intake category was associated with a 34% lower risk of cancer.
In summary, even though 8 meta-analyses have been published on the association between whole grain intake and total cancer mortality, it must be noted that 6 of meta-analyses [20,21,22,26,29,33] relied on essentially the same 6 cohort studies for determination of risk estimates [81,82,83,84,85,87], all from the United States or Europe. The data from Huang et al. (NIH-AARP Diet and Health Study) [82], Jacobs et al. (Iowa Women’s Health Study) [83], and Wu et al. (Nurses’ Health Study I and Health Professionals Follow-up Study) [85] were used in all 6 of these meta-analyses, the data from Buil–Cosiales et al. (PREDIMED trial) [81] and Johnsen et al. (HELGA cohort) [84] were used in 5 of the meta-analyses, and data from Jacobs et al. (Norwegian County Study) [87] were used in 4 of these meta-analyses (see Supplementary Table S2). Thus, it is not surprising that the risk reductions associated with whole grain intake were similar across these meta-analyses.
3.2. Whole Grain Intake and Site-Specific Cancer Risk
Eleven of the published meta-analyses provided risk estimates for whole grain intake and site-specific cancer risk, including colorectal [16,19,24,26,28,32], colon and rectal [16,19,28], gastric [24,32,35,36], pancreatic [24,25], breast [24,30], prostate [26,34], esophageal [24,32], oral [24], endometrial [24], brain [24], and non-Hodgkin’s lymphoma [24]. All results are presented in Table 2 and are described below. With few exceptions, whole grain intake was associated with lower risk of site-specific cancers.
3.2.1. Colorectal, Colon, and Rectal Cancer
Without exception, all six meta-analyses reported significantly lower colorectal cancer risk associated with whole grain intake (Table 2). Four of these were based entirely on cohort studies [16,19,26,28], one entirely on case-control studies [24], and one used both cohort and case-control studies [32]. In the five meta-analyses comparing the highest vs. lowest intake groups, participants with the highest intake of whole grains had an 11% to 21% lower risk of colorectal cancer. In the four dose-response analyses, colorectal cancer risk was reduced by 17% for each 90 g/day [19,28], by 5% for each 30 g/day [16], and by 3% for each 15 g/day [26]. When adjusting for dose, the combined results of these four dose-response analyses [16,19,26,28] suggest that colorectal cancer risk is reduced by approximately 15% to 17% per 90 g/day intake of whole grains.
For colon cancer, all three meta-analyses reported lower risk associated with whole grain intake. In the highest vs. lowest intake comparisons, high intake of whole grains was associated with a 15% to 18% lower risk of colon cancer. In the dose-response analyses, colon cancer risk was reduced by 14% to 18% for each 90 g/day [19,28] and by 3% for each 30 g/day [16] consumption of whole grains.
By contrast, for rectal cancer only one of the three meta-analyses reported a significantly lower risk associated with whole grain intake. Although the relative risks in categorical and dose-response analyses ranged between 0.80 and 0.94, only the 20% lower risk reported by Schwingshackl et al. [16] in the highest vs. lowest intake comparisons was statistically significant.
3.2.2. Gastric Cancer
Four meta-analyses have been published on the association between whole grain intake and gastric cancer risk [24,32,35,36]. All four, which relied primarily [32,35,36] or entirely [24] on case-control studies, reported 13% to 39% lower risk when comparing highest vs. lowest intake groups. No dose-response analyses have been published.
3.2.3. Pancreatic Cancer
Two meta-analyses have been published on the association between whole grain intake and pancreatic cancer risk. In a meta-analysis of 4 case-control studies, Jacobs et al. [24] reported a 30% lower risk of pancreatic cancer in a comparison of highest vs. lowest consumption of whole grains. Using data from 3 case-control studies, one cohort study, and the point estimate from the earlier meta-analysis by Jacobs et al. [24], the meta-analysis by Lei et al. [25] indicated a 24% lower risk of pancreatic cancer in comparing highest vs. lowest intakes of whole grains.
3.2.4. Prostate Cancer
Three meta-analyses have been published on the association between whole grain intake and risk of prostate cancer, including 2 categorical analyses [26,34] and 1 dose-response analysis [26]. In contrast to the site-specific cancers discussed above, none of the meta-analyses indicated a benefit for whole grain intake. In fact, one of the meta-analyses indicated a 10% higher risk of prostate cancer when comparing highest vs. lowest intake groups [26] (Table 2).
3.2.5. Breast Cancer
Three meta-analyses have been published on breast cancer, including 2 categorical analyses [24,30] and 1 dose-response analysis [30]. In the meta-analysis by Xiao et al. [30], which included 4 cohort studies and 7 case-control studies, whole grain intake was associated with a 16% lower risk of breast cancer when comparing highest vs. lowest intake categories. In the dose-response analysis that included 3 cohort studies and 3 case-control studies, each 50 g per day increase in whole grain intake was associated with a 17% lower risk of breast cancer.
In an earlier meta-analysis by Jacobs et al. [24], which included only 2 case-control studies, whole grain consumption was not associated with a significantly lower risk of breast cancer, although the odds ratio of 0.86 was similar to the statistically significant relative risk of 0.84 reported in the more recent meta-analysis of Xiao et al. [30] (Table 2).
3.2.6. Esophageal Cancer
3.2.7. Other Cancers
Limited data have been published on other cancers, including oral, brain, endometrial, and non-Hodgkin’s lymphoma. For each of these cancers, only one meta-analysis has been published, using case-control studies [24]. In categorical analyses, the highest intake group for whole grains was associated with a 43% lower risk of oral/pharyngeal/tongue cancer, a 33% lower risk of brain cancer, a 45% lower risk of endometrial cancer, and a 59% lower risk of non-Hodgkin’s lymphoma.
3.3. Refined Grain Intake and Cancer
In contrast to whole grains, only a few meta-analyses have been published on the association between refined grain intake and cancer, including total cancer [20], colorectal cancer [16], colon cancer [16], and gastric cancer [35,36]. All results are presented in Table 3.
3.3.1. Total Cancer
3.3.2. Colorectal Cancer
Schwingshackl et al. [16] included 3 cohort studies in meta-analyses on the association between refined grain intake and colorectal cancer [95,103] and colon cancer [95,112]. In comparison of the highest vs. lowest intakes, refined grain consumption was not associated with colorectal cancer but was associated with a 27% higher risk of colon cancer.
3.3.3. Gastric Cancer
Two meta-analyses have reported on the association between refined grain intake and risk of gastric cancer. Using highest vs. lowest intake comparisons from 18 case-control studies, Wang et al. [35] reported that refined grain intake was associated with a 36% higher risk of gastric cancer. In a smaller meta-analysis by Xu et al. [36], which included 1 cohort study and 2 case-control studies, the highest intake group of refined grains had a 65% greater risk of gastric cancer compared to the lowest intake group.
4. Discussion
Published meta-analyses reviewed herein demonstrate that whole grain intake is consistently associated with lower risk of total cancer mortality. This was observed in both categorical and dose-response analyses. Consistently lower risks for colorectal, colon, gastric, pancreatic, and esophageal cancers were also observed. These findings are congruent with the findings of expert reports and public health recommendations that advocate for greater consumption of whole grains [2,3,10]. Many countries include whole grains in their dietary recommendations [153]. For example, the United States dietary guidelines recommend that Americans consume at least 3 servings per day of whole grains, with a serving defined as 1 ounce-equivalent (~28 g) of a whole grain food [3]. Only 2% to 7% of the U.S. population achieves this goal [154,155], with whole grain intake the averaging <1 serving per day [10,155]. Consequently, the dose-response analyses in Table 1 and Table 2 suggest that significant reductions in total, colorectal, and colon cancer risk may be achieved by increasing whole grain intake above current levels.
In contrast to these findings, whole grain intake was not associated with decreased risk of prostate cancer. Only two publications reported meta-analyses on whole grain intake and prostate cancer risk (Table 2). The only meta-analysis that reported a higher prostate cancer risk was associated with whole grain intake included only 3 studies. It is also important to note that of the 9 studies included in the meta-analyses on prostate cancer, 4 of them did not provide a definition of whole grains (Supplementary Table S2). Thus, conclusions about the association between whole grain intake and prostate cancer should be interpreted with these limitations in mind.
Unlike the results for whole grains, meta-analyses revealed no consistent findings on the association between refined grain intake and cancer risk. Three of the meta-analyses indicated that refined grain intake may be associated with higher risk of colon and gastric cancer. In contrast, one meta-analysis reported a 6% lower risk of total cancer mortality associated with higher intake of refined grains. There are several important limitations to the meta-analyses on refined grains, and these are discussed below. Nevertheless, the limited and inconsistent findings from these meta-analyses on refined grains analyzed as a separate food category are not entirely supportive of the data from dietary pattern analyses showing that a Western dietary pattern that includes refined grains is usually associated with higher risk of cancer [11,12,13,14,15].
4.1. Mechanisms for Reduced Cancer Risk Associated with Whole Grain Intake
Whole grains may reduce cancer risk via a number of mechanisms, as reviewed previously [9,156,157,158]. Whole grain intake is correlated with cereal fiber intake [159,160,161]. Three meta-analyses have shown that cereal fiber is associated with reduced cancer risk [19,162,163], and two of these focused solely on colorectal cancer risk [19,162]. This may be particularly relevant for interpretation of the consistent findings of meta-analyses showing whole grain intake associated with reduced risk of colorectal cancer [16,19,24,26,28,32]. Cereal fiber increases fecal bulk and reduces gastrointestinal transit time [164], which could dilute carcinogens and reduce their absorption. Whole grain consumption, particularly from wheat, increases production of short-chain fatty acids, such as butyrate. Butyrate is a major energy source of normal human colon cells [165]. Butyrate has also been shown to inhibit growth of cancerous cells, mainly by inducing apoptosis [166], and has been shown to be protective against colorectal cancer [167,168]. Whole grain intake is associated with lower body mass index and central adiposity [169], which could have the effect of reducing adiposity-related cancers.
Not all meta-analyses and systematic reviews show uniformly lower cancer risks associated with cereal fiber intake [170,171,172]. However, these meta-analyses focused on breast, endometrial, and renal cancer, which suggests that cereal fiber may be more important for reducing colorectal cancer risk, as discussed above. It should be noted, however, that whole grain intake is associated with significantly lower cancer risk even after adjusting for cereal fiber intake [82]. Thus, the consistent finding of lower risk of total and site-specific cancers associated with whole grain intake may be due to other properties of whole grains [173]. For example, in contrast to the meta-analyses reporting no association between cereal fiber intake and risk of breast or endometrial cancer [170,171], Xiao et al. [30] reported lower breast cancer risk associated with whole grain intake in both categorical and dose-response analyses, and Jacobs et al. [24] reported lower risk of endometrial cancer in highest vs. lowest whole grain intake groups (Table 2). Whole grain foods are a major source of antioxidants and phenolic acids, which can reduce oxidative damage [173]. Whole grain foods contain significant quantities of bioactive compounds that have anticarcinogenic properties [156,157,173,174]. The collective anticarcinogenic impacts of these bioactive compounds likely explain much of the findings from prospective cohort studies [157,173].
4.2. Strengths and Weaknesses of the Meta-Analyses
A major weakness in the literature summarized in this review is the lack of consistency in the definitions of whole grains and refined grains in studies included in the meta-analyses (Supplementary Tables S2 and S3). Although many studies provided detailed descriptions of foods defined as whole grains [53,71,83,85,91,92,93,94,95,96,98,100,105,108,110,115,121,132,133,134], a number of them did not. For example, many studies included only one whole grain food in the definition of whole grains, such as whole grain bread or whole meal bread [42,43,44,45,46,52,54,65,66,67,68,69,74,75,76,79,80,86,87,88,90,103,106,109,119,138]. Even more problematic, 17 studies provided no definition of whole grains [73,81,97,99,101,104,107,111,112,114,116,120,122,126,127,130,135]. Two cohort studies defined whole grains as foods containing >25% whole grains or bran [82,117], which suggests that whole grain foods could have included a substantial amount of non-whole grain foods. Future research must include more comprehensive definitions of whole grain foods to better understand the association between whole grain intake and cancer risk.
Whereas whole grains are typically defined to include staple grain foods such as bread, cereals, and pasta, many studies have included indulgent grain foods in their definition of refined grains [5]. In the studies used in the meta-analyses presented in Table 3, refined grains have been defined to include cookies, doughnuts, sugar and layer cake [118], sweet buns [95,112,118], pancakes and waffles [83,95,112,117,118], muffins [83,112], and pizza [83,112,117]. These represent very commonly consumed foods and frequently contain high amounts of sugar and/or fat. It is plausible that consuming large amounts of indulgent grain foods may offset any beneficial effects of staple grain foods. It is also important to note that most of the studies used in the meta-analyses did not specifically define refined grains (Supplementary Table S3). Lastly, the number of studies included in the meta-analyses on refined grains was comparatively small. Three of the meta-analyses included only 2 studies, and 1 meta-analysis included only 3 studies. Although one meta-analysis included 18 studies, 14 of the publications used in that meta-analysis did not provide a definition for refined grains (Supplementary Table S3). For these reasons, and relative lack of published data, the associations between refined grain intake and cancer risk must be viewed very cautiously.
On the other hand, refined grain foods are an important source of dietary fiber due to the fact that refined grain consumption is much greater than whole grain consumption [175,176]. Based on National Health and Nutrition Examination Survey data in the United States, for example, 39% of dietary fiber comes from grain foods that contain no whole grain [175]. Thus, refined grains from staple grain foods are an important source of cereal fiber, and cereal fiber consumption has been shown to be associated with reduced risk of cancer [19,162,163]. Research on the distinct associations between consumption of staple and indulgent foods made with refined grains is needed.
It is also important to acknowledge that 6 of the 9 meta-analyses on total cancer mortality relied on essentially the same 6 cohort studies for determination of relative risks [81,82,83,84,85,87]. These cohorts, as well as all others included in the meta-analyses of total cancer mortality, are all from the United States or Europe. Results from these cohorts may not be broadly generalizable to other populations throughout the world. In addition, it is acknowledged that only 1 author performed the search and selection of the meta-analyses included in this review. However, three databases were used in the search, and all selected meta-analyses identified in the initial search were further evaluated by hand-searching their reference lists and examining citation records to find additional meta-analyses. This process yielded 3 additional publications that satisfied inclusion criteria. Thus, the author is confident that the search methodology identified all relevant meta-analyses.
Despite these weaknesses, the meta-analyses reviewed have some notable strengths. With two exceptions, all meta-analyses reported no publication bias that might confound interpretation of the results. The only meta-analysis that reported a significant Egger’s test was that of Zhang et al. [32] on esophageal cancer. Jacobs et al. [24] did not report data on bias or heterogeneity. Most of the meta-analyses reported statistically significant I2, which suggests that variation across studies was not due to chance. The considerable differences in definitions of whole and refined grains may also have contributed to the significant heterogeneity across studies.
5. Conclusions
Meta-analyses consistently show that whole grain consumption is associated with lower risk of total cancer mortality. Risk reductions for the highest intakes of whole grains ranged between 5% and 12%. In dose-response analyses, each 30 g/day intake of whole grains was associated with a ~7% lower risk of cancer mortality. For site-specific cancers, meta-analyses indicate that whole grain intake is consistently associated with lower cancer risk, with the strongest evidence for colorectal, gastric, pancreatic, and esophageal cancers. The only cancer for which whole grain intake was not associated with lower risk was prostate cancer. Overall, these meta-analyses of cohort and case-control studies support the recommendations for increased whole grain consumption [2,3].
Refined grain intake may reduce the risk of total cancer, but the meta-analysis included only 2 studies. High intake of refined grain may increase risk of gastric cancer, but these conclusions must be viewed skeptically due to the weaknesses described above. Considerably more research is necessary on the association between refined grain intake and cancer risk before definitive conclusions can be drawn and evidence-based dietary guidelines established.
Supplementary Materials
The following are available online at https://www.mdpi.com/2072-6643/12/12/3756/s1, Table S1: Characteristics of the meta-analyses included in this review; Table S2: Characteristics of studies included in the meta-analyses on the association between whole grain intake and cancer risk; Table S3: Characteristics of studies included in the meta-analyses on the association between refined grain intake and cancer risk.
Funding
This research was supported in part by a grant from the American Bakers Association.
Conflicts of Interest
The author is a member of the scientific advisory boards for the Grain Foods Foundation, the Wheat Foods Council, and Ardent Mills, L.L.C.
References
- Kyro, C.; Tjonneland, A. Whole grains and public health. BMJ 2016, 353, i3046. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Cancer Research Fund; American Institute for Cancer Research. Diet, Nutrition, Physical Activity and Cancer: A Global Perspective. Available online: http://dietandcancerreport.org (accessed on 15 September 2020).
- U.S. Department of Health and Human Services; U.S. Department of Agriculture. 2015–2020 Dietary Guidelines for Americans 8th Edition. Available online: http://health.gov/dietaryguidelines/2015/guidelines/ (accessed on 11 June 2020).
- Gaesser, G.A. Carbohydrate quantity and quality in relation to body mass index. J. Am. Diet. Assoc. 2007, 107, 1768–1780. [Google Scholar] [CrossRef] [PubMed]
- Gaesser, G.A. Perspective: Refined grains and health: Genuine risk, or guilt by association? Adv. Nutr. 2019, 10, 361–371. [Google Scholar] [CrossRef] [PubMed]
- Williams, P.G. Evaluation of the evidence between consumption of refined grains and health outcomes. Nutr. Rev. 2012, 70, 80–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- AACC Committee to Define Whole Grain. AACC members agree on definition of whole grain. Cereal Foods World 2000, 45, 79. Available online: https://www.aaccnet.org/initiatives/definitions/Documents/WholeGrains/wgflyer.pdf (accessed on 7 November 2020).
- Jones, J.M.; Garcia, C.G.; Braun, H.J. Perspective: Whole and refined grains and health-evidence supporting “Make half your grains whole”. Adv. Nutr. 2020, 11, 492–506. [Google Scholar] [CrossRef] [Green Version]
- Makarem, N.; Nicholson, J.M.; Bandera, E.V.; McKeown, N.M.; Parekh, N. Consumption of whole grains and cereal fiber in relation to cancer risk: A systematic review of longitudinal studies. Nutr. Rev. 2016, 74, 353–373. [Google Scholar] [CrossRef] [Green Version]
- Office of Disease Prevention and Health Promotion. Report of the Dietary Guidelines Advisory Committee on the Dietary Guidelines of Americans 2015 to the Secretary of Agriculture and the Secretary of Health and Human Services. Available online: https://health.gov/dietaryguidelines/2015-scientific-report/ (accessed on 11 June 2020).
- Bertuccio, P.; Rosato, V.; Andreano, A.; Ferraroni, M.; Decarli, A.; Edefonti, V.; La Vecchia, C. Dietary patterns and gastric cancer risk: A systematic review and meta-analysis. Ann. Oncol. 2013, 24, 1450–1458. [Google Scholar] [CrossRef]
- Fabiani, R.; Minelli, L.; Bertarelli, G.; Bacci, S. A western dietary pattern increases prostate cancer risk: A systematic review and meta-analysis. Nutrients 2016, 8, 626. [Google Scholar] [CrossRef]
- Garcia-Larsen, V.; Morton, V.; Norat, T.; Moreira, A.; Potts, J.F.; Reeves, T.; Bakolis, I. Dietary patterns derived from principal component analysis (PCA) and risk of colorectal cancer: A systematic review and meta-analysis. Eur. J. Clin. Nutr. 2019, 73, 366–386. [Google Scholar] [CrossRef]
- Lu, P.Y.; Shu, L.; Shen, S.S.; Chen, X.J.; Zhang, X.Y. Dietary patterns and pancreatic cancer risk: A meta-analysis. Nutrients 2017, 9, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shu, L.; Wang, X.Q.; Wang, S.F.; Wang, S.; Mu, M.; Zhao, Y.; Sheng, J.; Tao, F.B. Dietary patterns and stomach cancer: A meta-analysis. Nutr. Cancer 2013, 65, 1105–1115. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Schwedhelm, C.; Hoffmann, G.; Knuppel, S.; Laure Preterre, A.; Iqbal, K.; Bechthold, A.; De Henauw, S.; Michels, N.; Devleesschauwer, B.; et al. Food groups and risk of colorectal cancer. Int. J. Cancer 2018, 142, 1748–1758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwingshackl, L.; Schwedhelm, C.; Hoffmann, G.; Lampousi, A.M.; Knuppel, S.; Iqbal, K.; Bechthold, A.; Schlesinger, S.; Boeing, H. Food groups and risk of all-cause mortality: A systematic review and meta-analysis of prospective studies. Am. J. Clin. Nutr. 2017, 105, 1462–1473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Aune, D.; Chan, D.S.; Lau, R.; Vieira, R.; Greenwood, D.C.; Kampman, E.; Norat, T. Dietary fibre, whole grains, and risk of colorectal cancer: Systematic review and dose-response meta-analysis of prospective studies. BMJ 2011, 343, d6617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aune, D.; Keum, N.; Giovannucci, E.; Fadnes, L.T.; Boffetta, P.; Greenwood, D.C.; Tonstad, S.; Vatten, L.J.; Riboli, E.; Norat, T. Whole grain consumption and risk of cardiovascular disease, cancer, and all cause and cause specific mortality: Systematic review and dose-response meta-analysis of prospective studies. BMJ 2016, 353, i2716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benisi-Kohansal, S.; Saneei, P.; Salehi-Marzijarani, M.; Larijani, B.; Esmaillzadeh, A. Whole-grain intake and mortality from all causes, cardiovascular disease, and cancer: A systematic review and dose-response meta-analysis of prospective cohort studies. Adv. Nutr. 2016, 7, 1052–1065. [Google Scholar] [CrossRef] [Green Version]
- Chen, G.C.; Tong, X.; Xu, J.Y.; Han, S.F.; Wan, Z.X.; Qin, J.B.; Qin, L.Q. Whole-grain intake and total, cardiovascular, and cancer mortality: A systematic review and meta-analysis of prospective studies. Am. J. Clin. Nutr. 2016, 104, 164–172. [Google Scholar] [CrossRef] [Green Version]
- Haas, P.; Machado, M.J.; Anton, A.A.; Silva, A.S.; de Francisco, A. Effectiveness of whole grain consumption in the prevention of colorectal cancer: Meta-analysis of cohort studies. Int. J. Food Sci. Nutr. 2009, 60 (Suppl. 6), 1–13. [Google Scholar] [CrossRef]
- Jacobs, D.R., Jr.; Marquart, L.; Slavin, J.; Kushi, L.H. Whole-grain intake and cancer: An expanded review and meta-analysis. Nutr. Cancer 1998, 30, 85–96. [Google Scholar] [CrossRef] [PubMed]
- Lei, Q.; Zheng, H.; Bi, J.; Wang, X.; Jiang, T.; Gao, X.; Tian, F.; Xu, M.; Wu, C.; Zhang, L.; et al. Whole grain intake reduces pancreatic cancer risk: A meta-analysis of observational studies. Medicine (Baltimore) 2016, 95, e2747. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, A.; Mann, J.; Cummings, J.; Winter, N.; Mete, E.; Te Morenga, L. Carbohydrate quality and human health: A series of systematic reviews and meta-analyses. Lancet 2019, 393, 434–445. [Google Scholar] [CrossRef] [Green Version]
- Schwingshackl, L.; Schwedhelm, C.; Galbete, C.; Hoffmann, G. Adherence to mediterranean diet and risk of cancer: An updated systematic review and meta-analysis. Nutrients 2017, 9, 63. [Google Scholar] [CrossRef]
- Vieira, A.R.; Abar, L.; Chan, D.S.M.; Vingeliene, S.; Polemiti, E.; Stevens, C.; Greenwood, D.; Norat, T. Foods and beverages and colorectal cancer risk: A systematic review and meta-analysis of cohort studies, an update of the evidence of the WCRF-AICR Continuous Update Project. Ann. Oncol. 2017, 28, 1788–1802. [Google Scholar] [CrossRef]
- Wei, H.; Gao, Z.; Liang, R.; Li, Z.; Hao, H.; Liu, X. Whole-grain consumption and the risk of all-cause, CVD and cancer mortality: A meta-analysis of prospective cohort studies. Br. J. Nutr. 2016, 116, 514–525. [Google Scholar] [CrossRef] [Green Version]
- Xiao, Y.; Ke, Y.; Wu, S.; Huang, S.; Li, S.; Lv, Z.; Yeoh, E.K.; Lao, X.; Wong, S.; Kim, J.H.; et al. Association between whole grain intake and breast cancer risk: A systematic review and meta-analysis of observational studies. Nutr. J. 2018, 17, 87. [Google Scholar] [CrossRef]
- Zhang, B.; Zhao, Q.; Guo, W.; Bao, W.; Wang, X. Association of whole grain intake with all-cause, cardiovascular, and cancer mortality: A systematic review and dose-response meta-analysis from prospective cohort studies. Eur. J. Clin. Nutr. 2018, 72, 57–65. [Google Scholar] [CrossRef]
- Zhang, X.F.; Wang, X.K.; Tang, Y.J.; Guan, X.X.; Guo, Y.; Fan, J.M.; Cui, L.L. Association of whole grains intake and the risk of digestive tract cancer: A systematic review and meta-analysis. Nutr. J. 2020, 19, 52. [Google Scholar] [CrossRef]
- Zong, G.; Gao, A.; Hu, F.B.; Sun, Q. Whole grain intake and mortality from all causes, cardiovascular disease, and cancer: A meta-analysis of prospective cohort studies. Circulation 2016, 133, 2370–2380. [Google Scholar] [CrossRef] [Green Version]
- Wang, R.J.; Tang, J.E.; Chen, Y.; Gao, J.G. Dietary fiber, whole grains, carbohydrate, glycemic index, and glycemic load in relation to risk of prostate cancer. Oncol. Targets Ther. 2015, 8, 2415–2426. [Google Scholar] [CrossRef] [Green Version]
- Wang, T.; Zhan, R.; Lu, J.; Zhong, L.; Peng, X.; Wang, M.; Tang, S. Grain consumption and risk of gastric cancer: A meta-analysis. Int. J. Food Sci. Nutr. 2020, 71, 164–175. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Yang, J.; Du, L.; Li, K.; Zhou, Y. Association of whole grain, refined grain, and cereal consumption with gastric cancer risk: A meta-analysis of observational studies. Food Sci. Nutr. 2019, 7, 256–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef]
- Whiting, P.; Savovic, J.; Higgins, J.P.; Caldwell, D.M.; Reeves, B.C.; Shea, B.; Davies, P.; Kleijnen, J.; Churchill, R.; Group, R. ROBIS: A new tool to assess risk of bias in systematic reviews was developed. J. Clin. Epidemiol. 2016, 69, 225–234. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Bidoli, E.; Franceschi, S.; Talamini, R.; Barra, S.; La Vecchia, C. Food consumption and cancer of the colon and rectum in north-eastern Italy. Int. J. Cancer 1992, 50, 223–229. [Google Scholar] [CrossRef]
- Boeing, H.; Frentzel-Beyme, R.; Berger, M.; Berndt, V.; Gores, W.; Korner, M.; Lohmeier, R.; Menarcher, A.; Mannl, H.F.; Meinhardt, M.; et al. Case-control study on stomach cancer in Germany. Int. J. Cancer 1991, 47, 858–864. [Google Scholar] [CrossRef]
- Boeing, H.; Jedrychowski, W.; Wahrendorf, J.; Popiela, T.; Tobiasz-Adamczyk, B.; Kulig, A. Dietary risk factors in intestinal and diffuse types of stomach cancer: A multicenter case-control study in Poland. Cancer Causes Control 1991, 2, 227–233. [Google Scholar] [CrossRef]
- Boeing, H.; Schlehofer, B.; Blettner, M.; Wahrendorf, J. Dietary carcinogens and the risk for glioma and meningioma in Germany. Int. J. Cancer 1993, 53, 561–565. [Google Scholar] [CrossRef] [PubMed]
- Bueno de Mesquita, H.B.; Maisonneuve, P.; Runia, S.; Moerman, C.J. Intake of foods and nutrients and cancer of the exocrine pancreas: A population-based case-control study in The Netherlands. Int. J. Cancer 1991, 48, 540–549. [Google Scholar] [CrossRef] [PubMed]
- Centonze, S.; Boeing, H.; Leoci, C.; Guerra, V.; Misciagna, G. Dietary habits and colorectal cancer in a low-risk area. Results from a population-based case-control study in southern Italy. Nutr. Cancer 1994, 21, 233–246. [Google Scholar] [CrossRef]
- Decarli, A.; Liati, P.; Negri, E.; Franceschi, S.; La Vecchia, C. Vitamin A and other dietary factors in the etiology of esophageal cancer. Nutr. Cancer 1987, 10, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Franceschi, S.; Barra, S.; La Vecchia, C.; Bidoli, E.; Negri, E.; Talamini, R. Risk factors for cancer of the tongue and the mouth. A case-control study from northern Italy. Cancer 1992, 70, 2227–2233. [Google Scholar] [CrossRef]
- Franceschi, S.; Levi, F.; Negri, E.; Fassina, A.; La Vecchia, C. Diet and thyroid cancer: A pooled analysis of four European case-control studies. Int. J. Cancer 1991, 48, 395–398. [Google Scholar] [CrossRef] [PubMed]
- Franceschi, S.; Serraino, D.; Carbone, A.; Talamini, R.; La Vecchia, C. Dietary factors and non-Hodgkin’s lymphoma: A case-control study in the northeastern part of Italy. Nutr. Cancer 1989, 12, 333–341. [Google Scholar] [CrossRef]
- Giles, G.G.; McNeil, J.J.; Donnan, G.; Webley, C.; Staples, M.P.; Ireland, P.D.; Hurley, S.F.; Salzberg, M. Dietary factors and the risk of glioma in adults: Results of a case-control study in Melbourne, Australia. Int. J. Cancer 1994, 59, 357–362. [Google Scholar] [CrossRef]
- Gold, E.B.; Gordis, L.; Diener, M.D.; Seltser, R.; Boitnott, J.K.; Bynum, T.E.; Hutcheon, D.F. Diet and other risk factors for cancer of the pancreas. Cancer 1985, 55, 460–467. [Google Scholar] [CrossRef]
- Goodman, M.T.; Wilkens, L.R.; Hankin, J.H.; Lyu, L.C.; Wu, A.H.; Kolonel, L.N. Association of soy and fiber consumption with the risk of endometrial cancer. Am. J. Epidemiol. 1997, 146, 294–306. [Google Scholar] [CrossRef] [Green Version]
- Hansson, L.E.; Nyren, O.; Bergstrom, R.; Wolk, A.; Lindgren, A.; Baron, J.; Adami, H.O. Diet and risk of gastric cancer. A population-based case-control study in Sweden. Int. J. Cancer 1993, 55, 181–189. [Google Scholar] [CrossRef] [PubMed]
- La Vecchia, C.; Decarli, A.; Fasoli, M.; Gentile, A. Nutrition and diet in the etiology of endometrial cancer. Cancer 1986, 57, 1248–1253. [Google Scholar] [CrossRef]
- La Vecchia, C.; Decarli, A.; Franceschi, S.; Gentile, A.; Negri, E.; Parazzini, F. Dietary factors and the risk of breast cancer. Nutr. Cancer 1987, 10, 205–214. [Google Scholar] [CrossRef] [PubMed]
- La Vecchia, C.; Decarli, A.; Negri, E.; Parazzini, F.; Gentile, A.; Cecchetti, G.; Fasoli, M.; Franceschi, S. Dietary factors and the risk of epithelial ovarian cancer. J. Natl. Cancer Inst. 1987, 79, 663–669. [Google Scholar] [PubMed]
- La Vecchia, C.; Negri, E.; D’Avanzo, B.; Franceschi, S.; Decarli, A.; Boyle, P. Dietary indicators of laryngeal cancer risk. Cancer Res. 1990, 50, 4497–4500. [Google Scholar] [PubMed]
- La Vecchia, C.; Negri, E.; Decarli, A.; D’Avanzo, B.; Franceschi, S. A case-control study of diet and gastric cancer in northern Italy. Int. J. Cancer 1987, 40, 484–489. [Google Scholar] [CrossRef]
- La Vecchia, C.; Negri, E.; Decarli, A.; D’Avanzo, B.; Franceschi, S. Risk factors for hepatocellular carcinoma in northern Italy. Int. J. Cancer 1988, 42, 872–876. [Google Scholar] [CrossRef]
- La Vecchia, C.; Negri, E.; Decarli, A.; D’Avanzo, B.; Gallotti, L.; Gentile, A.; Franceschi, S. A case-control study of diet and colorectal cancer in northern Italy. Int. J. Cancer 1988, 41, 492–498. [Google Scholar] [CrossRef]
- La Vecchia, C.; Negri, E.; Decarli, A.; D’Avanzo, B.; Liberati, C.; Franceschi, S. Dietary factors in the risk of bladder cancer. Nutr. Cancer 1989, 12, 93–101. [Google Scholar] [CrossRef]
- Levi, F.; Franceschi, S.; Negri, E.; La Vecchia, C. Dietary factors and the risk of endometrial cancer. Cancer 1993, 71, 3575–3581. [Google Scholar] [CrossRef]
- Levi, F.; La Vecchia, C.; Gulie, C.; Negri, E. Dietary factors and breast cancer risk in Vaud, Switzerland. Nutr. Cancer 1993, 19, 327–335. [Google Scholar] [CrossRef] [PubMed]
- Mack, T.M.; Yu, M.C.; Hanisch, R.; Henderson, B.E. Pancreas cancer and smoking, beverage consumption, and past medical history. J. Natl. Cancer Inst. 1986, 76, 49–60. [Google Scholar] [PubMed]
- McLaughlin, J.K.; Gridley, G.; Block, G.; Winn, D.M.; Preston-Martin, S.; Schoenberg, J.B.; Greenberg, R.S.; Stemhagen, A.; Austin, D.F.; Ershow, A.G.; et al. Dietary factors in oral and pharyngeal cancer. J. Natl. Cancer Inst. 1988, 80, 1237–1243. [Google Scholar] [CrossRef] [PubMed]
- Olsen, G.W.; Mandel, J.S.; Gibson, R.W.; Wattenberg, L.W.; Schuman, L.M. A case-control study of pancreatic cancer and cigarettes, alcohol, coffee and diet. Am. J. Public Health 1989, 79, 1016–1019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peters, R.K.; Garabrant, D.H.; Yu, M.C.; Mack, T.M. A case-control study of occupational and dietary factors in colorectal cancer in young men by subsite. Cancer Res. 1989, 49, 5459–5468. [Google Scholar] [PubMed]
- Pickle, L.W.; Greene, M.H.; Ziegler, R.G.; Toledo, A.; Hoover, R.; Lynch, H.T.; Fraumeni, J.F., Jr. Colorectal cancer in rural Nebraska. Cancer Res. 1984, 44, 363–369. [Google Scholar] [PubMed]
- Serraino, D.; Franceschi, S.; Talamini, R.; Frustaci, S.; La Vecchia, C. Non-occupational risk factors for adult soft-tissue sarcoma in northern Italy. Cancer Causes Control 1991, 2, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Slattery, M.L.; Berry, T.D.; Potter, J.; Caan, B. Diet diversity, diet composition, and risk of colon cancer (United States). Cancer Causes Control 1997, 8, 872–882. [Google Scholar] [CrossRef]
- Talamini, R.; Franceschi, S.; La Vecchia, C.; Serraino, D.; Barra, S.; Negri, E. Diet and prostatic cancer: A case-control study in northern Italy. Nutr. Cancer 1992, 18, 277–286. [Google Scholar] [CrossRef]
- Tavani, A.; Pregnolato, A.; Negri, E.; Franceschi, S.; Serraino, D.; Carbone, A.; La Vecchia, C. Diet and risk of lymphoid neoplasms and soft tissue sarcomas. Nutr. Cancer 1997, 27, 256–260. [Google Scholar] [CrossRef]
- Trichopoulos, D.; Ouranos, G.; Day, N.E.; Tzonou, A.; Manousos, O.; Papadimitriou, C.; Trichopoulos, A. Diet and cancer of the stomach: A case-control study in Greece. Int. J. Cancer 1985, 36, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Tuyns, A.J.; Kaaks, R.; Haelterman, M. Colorectal cancer and the consumption of foods: A case-control study in Belgium. Nutr. Cancer 1988, 11, 189–204. [Google Scholar] [CrossRef] [PubMed]
- Tuyns, A.J.; Kaaks, R.; Haelterman, M.; Riboli, E. Diet and gastric cancer. A case-control study in Belgium. Int. J. Cancer 1992, 51, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Winn, D.M.; Ziegler, R.G.; Pickle, L.W.; Gridley, G.; Blot, W.J.; Hoover, R.N. Diet in the etiology of oral and pharyngeal cancer among women from the southern United States. Cancer Res. 1984, 44, 1216–1222. [Google Scholar] [PubMed]
- Witte, J.S.; Longnecker, M.P.; Bird, C.L.; Lee, E.R.; Frankl, H.D.; Haile, R.W. Relation of vegetable, fruit, and grain consumption to colorectal adenomatous polyps. Am. J. Epidemiol. 1996, 144, 1015–1025. [Google Scholar] [CrossRef] [Green Version]
- Wu-Williams, A.H.; Yu, M.C.; Mack, T.M. Life-style, workplace, and stomach cancer by subsite in young men of Los Angeles County. Cancer Res. 1990, 50, 2569–2576. [Google Scholar] [PubMed]
- Yu, M.C.; Garabrant, D.H.; Peters, J.M.; Mack, T.M. Tobacco, alcohol, diet, occupation, and carcinoma of the esophagus. Cancer Res. 1988, 48, 3843–3848. [Google Scholar] [PubMed]
- Buil-Cosiales, P.; Zazpe, I.; Toledo, E.; Corella, D.; Salas-Salvado, J.; Diez-Espino, J.; Ros, E.; Fernandez-Creuet Navajas, J.; Santos-Lozano, J.M.; Aros, F.; et al. Fiber intake and all-cause mortality in the Prevencion con Dieta Mediterranea (PREDIMED) study. Am. J. Clin. Nutr. 2014, 100, 1498–1507. [Google Scholar] [CrossRef]
- Huang, T.; Xu, M.; Lee, A.; Cho, S.; Qi, L. Consumption of whole grains and cereal fiber and total and cause-specific mortality: Prospective analysis of 367,442 individuals. BMC Med. 2015, 13, 59. [Google Scholar] [CrossRef] [Green Version]
- Jacobs, D.R., Jr.; Andersen, L.F.; Blomhoff, R. Whole-grain consumption is associated with a reduced risk of noncardiovascular, noncancer death attributed to inflammatory diseases in the Iowa Women’s Health Study. Am. J. Clin. Nutr. 2007, 85, 1606–1614. [Google Scholar] [CrossRef] [Green Version]
- Johnsen, N.F.; Frederiksen, K.; Christensen, J.; Skeie, G.; Lund, E.; Landberg, R.; Johansson, I.; Nilsson, L.M.; Halkjaer, J.; Olsen, A.; et al. Whole-grain products and whole-grain types are associated with lower all-cause and cause-specific mortality in the Scandinavian HELGA cohort. Br. J. Nutr. 2015, 114, 608–623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, H.; Flint, A.J.; Qi, Q.; van Dam, R.M.; Sampson, L.A.; Rimm, E.B.; Holmes, M.D.; Willett, W.C.; Hu, F.B.; Sun, Q. Association between dietary whole grain intake and risk of mortality: Two large prospective studies in US men and women. JAMA Intern. Med. 2015, 175, 373–384. [Google Scholar] [CrossRef] [PubMed]
- Appleby, P.N.; Key, T.J.; Burr, M.L.; Thorogood, M. Mortality and fresh fruit consumption. IARC Sci. Publ. 2002, 156, 131–133. [Google Scholar] [PubMed]
- Jacobs, D.R., Jr.; Meyer, H.E.; Solvoll, K. Reduced mortality among whole grain bread eaters in men and women in the Norwegian County Study. Eur. J. Clin. Nutr. 2001, 55, 137–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Key, T.J.; Thorogood, M.; Appleby, P.N.; Burr, M.L. Dietary habits and mortality in 11,000 vegetarians and health conscious people: Results of a 17 year follow up. BMJ 1996, 313, 775–779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aarestrup, J.; Kyro, C.; Christensen, J.; Kristensen, M.; Wurtz, A.M.; Johnsen, N.F.; Overvad, K.; Tjonneland, A.; Olsen, A. Whole grain, dietary fiber, and incidence of endometrial cancer in a Danish cohort study. Nutr. Cancer 2012, 64, 1160–1168. [Google Scholar] [CrossRef]
- Bakken, T.; Braaten, T.; Olsen, A.; Kyro, C.; Lund, E.; Skeie, G. Consumption of Whole-Grain Bread and Risk of Colorectal Cancer among Norwegian Women (the NOWAC Study). Nutrients 2016, 8, 40. [Google Scholar] [CrossRef] [Green Version]
- Egeberg, R.; Olsen, A.; Christensen, J.; Johnsen, N.F.; Loft, S.; Overvad, K.; Tjonneland, A. Intake of whole-grain products and risk of prostate cancer among men in the Danish diet, cancer and health cohort study. Cancer Causes Control 2011, 22, 1133–1139. [Google Scholar] [CrossRef]
- Egeberg, R.; Olsen, A.; Loft, S.; Christensen, J.; Johnsen, N.F.; Overvad, K.; Tjonneland, A. Intake of whole grain products and risk of breast cancer by hormone receptor status and histology among postmenopausal women. Int. J. Cancer 2009, 124, 745–750. [Google Scholar] [CrossRef]
- Jacobs, D.R., Jr.; Meyer, K.A.; Kushi, L.H.; Folsom, A.R. Is whole grain intake associated with reduced total and cause-specific death rates in older women? The Iowa Women’s Health Study. Am. J. Public Health 1999, 89, 322–329. [Google Scholar] [CrossRef] [Green Version]
- Kyro, C.; Skeie, G.; Loft, S.; Landberg, R.; Christensen, J.; Lund, E.; Nilsson, L.M.; Palmqvist, R.; Tjonneland, A.; Olsen, A. Intake of whole grains from different cereal and food sources and incidence of colorectal cancer in the Scandinavian HELGA cohort. Cancer Causes Control 2013, 24, 1363–1374. [Google Scholar] [CrossRef] [PubMed]
- Larsson, S.C.; Giovannucci, E.; Bergkvist, L.; Wolk, A. Whole grain consumption and risk of colorectal cancer: A population-based cohort of 60,000 women. Br. J. Cancer 2005, 92, 1803–1807. [Google Scholar] [CrossRef] [PubMed]
- Nimptsch, K.; Kenfield, S.; Jensen, M.K.; Stampfer, M.J.; Franz, M.; Sampson, L.; Brand-Miller, J.C.; Willett, W.C.; Giovannucci, E. Dietary glycemic index, glycemic load, insulin index, fiber and whole-grain intake in relation to risk of prostate cancer. Cancer Causes Control 2011, 22, 51–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tabung, F.; Steck, S.E.; Su, L.J.; Mohler, J.L.; Fontham, E.T.; Bensen, J.T.; Hebert, J.R.; Zhang, H.; Arab, L. Intake of grains and dietary fiber and prostate cancer aggressiveness by race. Prostate Cancer 2012, 2012, 323296. [Google Scholar] [CrossRef]
- Egeberg, R.; Olsen, A.; Loft, S.; Christensen, J.; Johnsen, N.F.; Overvad, K.; Tjonneland, A. Intake of wholegrain products and risk of colorectal cancers in the diet, cancer and health cohort study. Br. J. Cancer 2010, 103, 730–734. [Google Scholar] [CrossRef]
- McCarl, M.; Harnack, L.; Limburg, P.J.; Anderson, K.E.; Folsom, A.R. Incidence of colorectal cancer in relation to glycemic index and load in a cohort of women. Cancer Epidemiol. Biomark. Prev. 2006, 15, 892–896. [Google Scholar] [CrossRef] [Green Version]
- Schatzkin, A.; Mouw, T.; Park, Y.; Subar, A.F.; Kipnis, V.; Hollenbeck, A.; Leitzmann, M.F.; Thompson, F.E. Dietary fiber and whole-grain consumption in relation to colorectal cancer in the NIH-AARP Diet and Health Study. Am. J. Clin. Nutr. 2007, 85, 1353–1360. [Google Scholar] [CrossRef] [Green Version]
- Fung, T.T.; Hu, F.B.; Wu, K.; Chiuve, S.E.; Fuchs, C.S.; Giovannucci, E. The Mediterranean and Dietary Approaches to Stop Hypertension (DASH) diets and colorectal cancer. Am. J. Clin. Nutr. 2010, 92, 1429–1435. [Google Scholar] [CrossRef] [Green Version]
- Pietinen, P.; Malila, N.; Virtanen, M.; Hartman, T.J.; Tangrea, J.A.; Albanes, D.; Virtamo, J. Diet and risk of colorectal cancer in a cohort of Finnish men. Cancer Causes Control 1999, 10, 387–396. [Google Scholar] [CrossRef]
- Sanjoaquin, M.A.; Appleby, P.N.; Thorogood, M.; Mann, J.I.; Key, T.J. Nutrition, lifestyle and colorectal cancer incidence: A prospective investigation of 10998 vegetarians and non-vegetarians in the United Kingdom. Br. J. Cancer 2004, 90, 118–121. [Google Scholar] [CrossRef] [Green Version]
- Vulcan, A.; Brandstedt, J.; Manjer, J.; Jirstrom, K.; Ohlsson, B.; Ericson, U. Fibre intake and incident colorectal cancer depending on fibre source, sex, tumour location and tumour, node, metastasis stage. Br. J. Nutr. 2015, 114, 959–969. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCullough, M.L.; Robertson, A.S.; Chao, A.; Jacobs, E.J.; Stampfer, M.J.; Jacobs, D.R.; Diver, W.R.; Calle, E.E.; Thun, M.J. A prospective study of whole grains, fruits, vegetables and colon cancer risk. Cancer Causes Control 2003, 14, 959–970. [Google Scholar] [CrossRef] [PubMed]
- Abu Mweis, S.S.; Tayyem, R.F.; Shehadah, I.; Bawadi, H.A.; Agraib, L.M.; Bani-Hani, K.E.; Al-Jaberi, T.; Al-Nusairr, M. Food groups and the risk of colorectal cancer: Results from a Jordanian case-control study. Eur. J. Cancer Prev. 2015, 24, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Angelo, S.N.; Lourenco, G.J.; Magro, D.O.; Nascimento, H.; Oliveira, R.A.; Leal, R.F.; Ayrizono Mde, L.; Fagundes, J.J.; Coy, C.S.; Lima, C.S. Dietary risk factors for colorectal cancer in Brazil: A case control study. Nutr. J. 2016, 15, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, X.; Wu, K.; Zhang, X.; Nishihara, R.; Cao, Y.; Fuchs, C.S.; Giovannucci, E.L.; Ogino, S.; Chan, A.T.; Song, M. Dietary intake of fiber, whole grains and risk of colorectal cancer: An updated analysis according to food sources, tumor location and molecular subtypes in two large US cohorts. Int. J. Cancer 2019, 145, 3040–3051. [Google Scholar] [CrossRef] [PubMed]
- Tayyem, R.F.; Bawadi, H.A.; Shehadah, I.; Agraib, L.M.; Al-Awwad, N.J.; Heath, D.D.; Bani-Hani, K.E. Consumption of Whole Grains, Refined Cereals, and Legumes and Its Association with Colorectal Cancer among Jordanians. Integr. Cancer Ther. 2016, 15, 318–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Um, C.Y.; Campbell, P.T.; Carter, B.; Wang, Y.; Gapstur, S.M.; McCullough, M.L. Association between grains, gluten and the risk of colorectal cancer in the Cancer Prevention Study-II Nutrition Cohort. Eur. J. Nutr. 2020, 59, 1739–1749. [Google Scholar] [CrossRef]
- Williams, C.D.; Satia, J.A.; Adair, L.S.; Stevens, J.; Galanko, J.; Keku, T.O.; Sandler, R.S. Dietary patterns, food groups, and rectal cancer risk in Whites and African-Americans. Cancer Epidemiol. Biomark. Prev. 2009, 18, 1552–1561. [Google Scholar] [CrossRef] [Green Version]
- Wu, K.; Hu, F.B.; Fuchs, C.; Rimm, E.B.; Willett, W.C.; Giovannucci, E. Dietary patterns and risk of colon cancer and adenoma in a cohort of men (United States). Cancer Causes Control 2004, 15, 853–862. [Google Scholar] [CrossRef]
- La Vecchia, C.; Decarli, A.; Negri, E.; Parazzini, F. Epidemiological aspects of diet and cancer: A summary review of case-control studies from northern Italy. Oncology 1988, 45, 364–370. [Google Scholar] [CrossRef]
- Mathew, A.; Gangadharan, P.; Varghese, C.; Nair, M.K. Diet and stomach cancer: A case-control study in South India. Eur. J. Cancer Prev. 2000, 9, 89–97. [Google Scholar] [CrossRef] [PubMed]
- McCullough, M.L.; Robertson, A.S.; Jacobs, E.J.; Chao, A.; Calle, E.E.; Thun, M.J. A prospective study of diet and stomach cancer mortality in United States men and women. Cancer Epidemiol. Biomark. Prev. 2001, 10, 1201–1205. [Google Scholar]
- Chatenoud, L.; La Vecchia, C.; Franceschi, S.; Tavani, A.; Jacobs, D.R., Jr.; Parpinel, M.T.; Soler, M.; Negri, E. Refined-cereal intake and risk of selected cancers in italy. Am. J. Clin. Nutr. 1999, 70, 1107–1110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kasum, C.M.; Jacobs, D.R., Jr.; Nicodemus, K.; Folsom, A.R. Dietary risk factors for upper aerodigestive tract cancers. Int. J. Cancer 2002, 99, 267–272. [Google Scholar] [CrossRef]
- Lissowska, J.; Gail, M.H.; Pee, D.; Groves, F.D.; Sobin, L.H.; Nasierowska-Guttmejer, A.; Sygnowska, E.; Zatonski, W.; Blot, W.J.; Chow, W.H. Diet and stomach cancer risk in Warsaw, Poland. Nutr. Cancer 2004, 48, 149–159. [Google Scholar] [CrossRef]
- Jedrychowski, W.; Boeing, H.; Popiela, T.; Wahrendorf, J.; Tobiasz-Adamczyk, B.; Kulig, J. Dietary practices in households as risk factors for stomach cancer: A familial study in Poland. Eur. J. Cancer Prev. 1992, 1, 297–304. [Google Scholar] [CrossRef]
- Munoz, S.E.; Ferraroni, M.; La Vecchia, C.; Decarli, A. Gastric cancer risk factors in subjects with family history. Cancer Epidemiol. Biomark. Prev. 1997, 6, 137–140. [Google Scholar]
- Chan, J.M.; Wang, F.; Holly, E.A. Whole grains and risk of pancreatic cancer in a large population-based case-control study in the San Francisco Bay Area, California. Am. J. Epidemiol. 2007, 166, 1174–1185. [Google Scholar] [CrossRef] [Green Version]
- Jansen, R.J.; Robinson, D.P.; Stolzenberg-Solomon, R.Z.; Bamlet, W.R.; de Andrade, M.; Oberg, A.L.; Hammer, T.J.; Rabe, K.G.; Anderson, K.E.; Olson, J.E.; et al. Fruit and vegetable consumption is inversely associated with having pancreatic cancer. Cancer Causes Control 2011, 22, 1613–1625. [Google Scholar] [CrossRef]
- La Vecchia, C.; Chatenoud, L.; Negri, E.; Franceschi, S. Session: Whole cereal grains, fibre and human cancer wholegrain cereals and cancer in Italy. Proc. Nutr. Soc. 2003, 62, 45–49. [Google Scholar] [CrossRef]
- Stolzenberg-Solomon, R.Z.; Pietinen, P.; Taylor, P.R.; Virtamo, J.; Albanes, D. Prospective study of diet and pancreatic cancer in male smokers. Am. J. Epidemiol. 2002, 155, 783–792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chatenoud, L.; Tavani, A.; La Vecchia, C.; Jacobs, D.R., Jr.; Negri, E.; Levi, F.; Franceschi, S. Whole grain food intake and cancer risk. Int. J. Cancer 1998, 77, 24–28. [Google Scholar] [CrossRef]
- Deneo-Pellegrini, H.; De Stefani, E.; Ronco, A.; Mendilaharsu, M. Foods, nutrients and prostate cancer: A case-control study in Uruguay. Br. J. Cancer 1999, 80, 591–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drake, I.; Sonestedt, E.; Gullberg, B.; Ahlgren, G.; Bjartell, A.; Wallstrom, P.; Wirfalt, E. Dietary intakes of carbohydrates in relation to prostate cancer risk: A prospective study in the Malmo Diet and Cancer cohort. Am. J. Clin. Nutr. 2012, 96, 1409–1418. [Google Scholar] [CrossRef]
- Hardin, J.; Cheng, I.; Witte, J.S. Impact of consumption of vegetable, fruit, grain, and high glycemic index foods on aggressive prostate cancer risk. Nutr. Cancer 2011, 63, 860–872. [Google Scholar] [CrossRef] [Green Version]
- Jain, M.G.; Hislop, G.T.; Howe, G.R.; Ghadirian, P. Plant foods, antioxidants, and prostate cancer risk: Findings from case-control studies in Canada. Nutr. Cancer 1999, 34, 173–184. [Google Scholar] [CrossRef]
- Lewis, J.E.; Soler-Vila, H.; Clark, P.E.; Kresty, L.A.; Allen, G.O.; Hu, J.J. Intake of plant foods and associated nutrients in prostate cancer risk. Nutr. Cancer 2009, 61, 216–224. [Google Scholar] [CrossRef]
- Adzersen, K.H.; Jess, P.; Freivogel, K.W.; Gerhard, I.; Bastert, G. Raw and cooked vegetables, fruits, selected micronutrients, and breast cancer risk: A case-control study in Germany. Nutr. Cancer 2003, 46, 131–137. [Google Scholar] [CrossRef]
- Farvid, M.S.; Cho, E.; Eliassen, A.H.; Chen, W.Y.; Willett, W.C. Lifetime grain consumption and breast cancer risk. Breast Cancer Res. Treat. 2016, 159, 335–345. [Google Scholar] [CrossRef]
- Mourouti, N.; Kontogianni, M.D.; Papavagelis, C.; Psaltopoulou, T.; Kapetanstrataki, M.G.; Plytzanopoulou, P.; Vassilakou, T.; Malamos, N.; Linos, A.; Panagiotakos, D.B. Whole grain consumption and breast cancer: A case-control study in women. J. Am. Coll. Nutr. 2016, 35, 143–149. [Google Scholar] [CrossRef]
- Nicodemus, K.K.; Jacobs, D.R., Jr.; Folsom, A.R. Whole and refined grain intake and risk of incident postmenopausal breast cancer (United States). Cancer Causes Control 2001, 12, 917–925. [Google Scholar] [CrossRef] [PubMed]
- Sonestedt, E.; Borgquist, S.; Ericson, U.; Gullberg, B.; Landberg, G.; Olsson, H.; Wirfalt, E. Plant foods and oestrogen receptor alpha- and beta-defined breast cancer: Observations from the Malmo Diet and Cancer cohort. Carcinogenesis 2008, 29, 2203–2209. [Google Scholar] [CrossRef] [PubMed]
- Tajaddini, A.; Pourzand, A.; Sanaat, Z.; Pirouzpanah, S. Dietary resistant starch contained foods and breast cancer risk: A case-control study in northwest of Iran. Asian Pac. J. Cancer Prev. 2015, 16, 4185–4192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yun, S.H.; Kim, K.; Nam, S.J.; Kong, G.; Kim, M.K. The association of carbohydrate intake, glycemic load, glycemic index, and selected rice foods with breast cancer risk: A case-control study in South Korea. Asia Pac. J. Clin. Nutr. 2010, 19, 383–392. [Google Scholar]
- Chen, H.; Ward, M.H.; Graubard, B.I.; Heineman, E.F.; Markin, R.M.; Potischman, N.A.; Russell, R.M.; Weisenburger, D.D.; Tucker, K.L. Dietary patterns and adenocarcinoma of the esophagus and distal stomach. Am. J. Clin. Nutr. 2002, 75, 137–144. [Google Scholar] [CrossRef] [Green Version]
- Jessri, M.; Rashidkhani, B.; Hajizadeh, B.; Jacques, P.F. Adherence to Mediterranean-style dietary pattern and risk of esophageal squamous cell carcinoma: A case-control study in Iran. J. Am. Coll. Nutr. 2012, 31, 338–351. [Google Scholar] [CrossRef]
- Levi, F.; Pasche, C.; Lucchini, F.; Chatenoud, L.; Jacobs, D.R., Jr.; La Vecchia, C. Refined and whole grain cereals and the risk of oral, oesophageal and laryngeal cancer. Eur. J. Clin. Nutr. 2000, 54, 487–489. [Google Scholar] [CrossRef] [Green Version]
- Sewram, V.; Sitas, F.; O’Connell, D.; Myers, J. Diet and esophageal cancer risk in the Eastern Cape Province of South Africa. Nutr. Cancer 2014, 66, 791–799. [Google Scholar] [CrossRef]
- Skeie, G.; Braaten, T.; Olsen, A.; Kyro, C.; Tjonneland, A.; Landberg, R.; Nilsson, L.M.; Wennberg, M.; Overvad, K.; Asli, L.A.; et al. Intake of whole grains and incidence of oesophageal cancer in the HELGA Cohort. Eur. J. Epidemiol. 2016, 31, 405–414. [Google Scholar] [CrossRef]
- De Stefani, E.; Correa, P.; Boffetta, P.; Deneo-Pellegrini, H.; Ronco, A.L.; Mendilaharsu, M. Dietary patterns and risk of gastric cancer: A case-control study in Uruguay. Gastric Cancer 2004, 7, 211–220. [Google Scholar] [CrossRef]
- Gao, C.M.; Takezaki, T.; Ding, J.H.; Li, M.S.; Tajima, K. Protective effect of allium vegetables against both esophageal and stomach cancer: A simultaneous case-referent study of a high-epidemic area in Jiangsu Province, China. Jpn. J. Cancer Res. 1999, 90, 614–621. [Google Scholar] [CrossRef] [PubMed]
- Hoshiyama, Y.; Sasaba, T. A case-control study of single and multiple stomach cancers in Saitama Prefecture, Japan. Jpn. J. Cancer Res. 1992, 83, 937–943. [Google Scholar] [CrossRef] [PubMed]
- Inoue, M.; Tajima, K.; Kobayashi, S.; Suzuki, T.; Matsuura, A.; Nakamura, T.; Shirai, M.; Nakamura, S.; Inuzuka, K.; Tominaga, S. Protective factor against progression from atrophic gastritis to gastric cancer--data from a cohort study in Japan. Int. J. Cancer 1996, 66, 309–314. [Google Scholar] [CrossRef]
- Li, J.Y.; Ershow, A.G.; Chen, Z.J.; Wacholder, S.; Li, G.Y.; Guo, W.; Li, B.; Blot, W.J. A case-control study of cancer of the esophagus and gastric cardia in Linxian. Int. J. Cancer 1989, 43, 755–761. [Google Scholar] [CrossRef] [PubMed]
- Machida-Montani, A.; Sasazuki, S.; Inoue, M.; Natsukawa, S.; Shaura, K.; Koizumi, Y.; Kasuga, Y.; Hanaoka, T.; Tsugane, S. Association of Helicobacter pylori infection and environmental factors in non-cardia gastric cancer in Japan. Gastric Cancer 2004, 7, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Navarro Silvera, S.A.; Mayne, S.T.; Risch, H.; Gammon, M.D.; Vaughan, T.L.; Chow, W.H.; Dubrow, R.; Schoenberg, J.B.; Stanford, J.L.; West, A.B.; et al. Food group intake and risk of subtypes of esophageal and gastric cancer. Int. J. Cancer 2008, 123, 852–860. [Google Scholar] [CrossRef] [Green Version]
- Ramon, J.M.; Serra, L.; Cerdo, C.; Oromi, J. Dietary factors and gastric cancer risk. A case-control study in Spain. Cancer 1993, 71, 1731–1735. [Google Scholar] [CrossRef]
- Sumathi, B.; Ramalingam, S.; Navaneethan, U.; Jayanthi, V. Risk factors for gastric cancer in South India. Singap. Med. J. 2009, 50, 147–151. [Google Scholar]
- You, W.C.; Blot, W.J.; Chang, Y.S.; Ershow, A.G.; Yang, Z.T.; An, Q.; Henderson, B.; Xu, G.W.; Fraumeni, J.F., Jr.; Wang, T.G. Diet and high risk of stomach cancer in Shandong, China. Cancer Res. 1988, 48, 3518–3523. [Google Scholar] [CrossRef]
- Oldways Whole Grains Council. Whole Grain Guidelines Worldwide. Available online: https://wholegrainscouncil.org/whole-grains-101/how-much-enough/whole-grain-guidelines-worldwide (accessed on 20 September 2020).
- Krebs-Smith, S.M.; Guenther, P.M.; Subar, A.F.; Kirkpatrick, S.I.; Dodd, K.W. Americans do not meet federal dietary recommendations. J. Nutr. 2010, 140, 1832–1838. [Google Scholar] [CrossRef]
- O’Neil, C.E.; Nicklas, T.A.; Zanovec, M.; Cho, S. Whole-grain consumption is associated with diet quality and nutrient intake in adults: The National Health and Nutrition Examination Survey, 1999-2004. J. Am. Diet. Assoc. 2010, 110, 1461–1468. [Google Scholar] [CrossRef] [PubMed]
- Slavin, J. Why whole grains are protective: Biological mechanisms. Proc. Nutr. Soc. 2003, 62, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Slavin, J. Whole grains and human health. Nutr. Res. Rev. 2004, 17, 99–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xie, M.; Liu, J.; Tsao, R.; Wang, Z.; Sun, B.; Wang, J. Whole grain consumption for the prevention and treatment of breast cancer. Nutrients 2019, 11, 1769. [Google Scholar] [CrossRef] [Green Version]
- Fung, T.T.; Hu, F.B.; Pereira, M.A.; Liu, S.; Stampfer, M.J.; Colditz, G.A.; Willett, W.C. Whole-grain intake and the risk of type 2 diabetes: A prospective study in men. Am. J. Clin. Nutr. 2002, 76, 535–540. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.; Manson, J.E.; Stampfer, M.J.; Hu, F.B.; Giovannucci, E.; Colditz, G.A.; Hennekens, C.H.; Willett, W.C. A prospective study of whole-grain intake and risk of type 2 diabetes mellitus in US women. Am. J. Public Health 2000, 90, 1409–1415. [Google Scholar] [CrossRef] [Green Version]
- McKeown, N.M.; Yoshida, M.; Shea, M.K.; Jacques, P.F.; Lichtenstein, A.H.; Rogers, G.; Booth, S.L.; Saltzman, E. Whole-grain intake and cereal fiber are associated with lower abdominal adiposity in older adults. J. Nutr. 2009, 139, 1950–1955. [Google Scholar] [CrossRef]
- Ben, Q.; Sun, Y.; Chai, R.; Qian, A.; Xu, B.; Yuan, Y. Dietary fiber intake reduces risk for colorectal adenoma: A meta-analysis. Gastroenterology 2014, 146, 689–699. [Google Scholar] [CrossRef]
- Hajishafiee, M.; Saneei, P.; Benisi-Kohansal, S.; Esmaillzadeh, A. Cereal fibre intake and risk of mortality from all causes, CVD, cancer and inflammatory diseases: A systematic review and meta-analysis of prospective cohort studies. Br. J. Nutr. 2016, 116, 343–352. [Google Scholar] [CrossRef]
- de Vries, J.; Miller, P.E.; Verbeke, K. Effects of cereal fiber on bowel function: A systematic review of intervention trials. World J. Gastroenterol. 2015, 21, 8952–8963. [Google Scholar] [CrossRef]
- Topping, D.L.; Clifton, P.M. Short-chain fatty acids and human colonic function: Roles of resistant starch and nonstarch polysaccharides. Physiol. Rev. 2001, 81, 1031–1064. [Google Scholar] [CrossRef] [PubMed]
- Young, G.P.; Hu, Y.; Le Leu, R.K.; Nyskohus, L. Dietary fibre and colorectal cancer: A model for environment--gene interactions. Mol. Nutr. Food Res. 2005, 49, 571–584. [Google Scholar] [CrossRef] [PubMed]
- Johnson, I.T.; Williamson, G.; Musk, S.R. Anticarcinogenic factors in plant foods: A new class of nutrients? Nutr. Res. Rev. 1994, 7, 175–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wattenberg, L.W. Inhibition of carcinogenesis by minor dietary constituents. Cancer Res. 1992, 52, 2085s–2091s. [Google Scholar]
- Harland, J.I.; Garton, L.E. Whole-grain intake as a marker of healthy body weight and adiposity. Public Health Nutr. 2008, 11, 554–563. [Google Scholar] [CrossRef] [Green Version]
- Aune, D.; Chan, D.S.; Greenwood, D.C.; Vieira, A.R.; Rosenblatt, D.A.; Vieira, R.; Norat, T. Dietary fiber and breast cancer risk: A systematic review and meta-analysis of prospective studies. Ann. Oncol. 2012, 23, 1394–1402. [Google Scholar] [CrossRef]
- Chen, K.; Zhao, Q.; Li, X.; Zhao, J.; Li, P.; Lin, S.; Wang, H.; Zang, J.; Xiao, Y.; Xu, W.; et al. Dietary fiber intake and endometrial cancer risk: A systematic review and meta-analysis. Nutrients 2018, 10, 945. [Google Scholar] [CrossRef] [Green Version]
- Huang, T.B.; Ding, P.P.; Chen, J.F.; Yan, Y.; Zhang, L.; Liu, H.; Liu, P.C.; Che, J.P.; Zheng, J.H.; Yao, X.D. Dietary fiber intake and risk of renal cell carcinoma: Evidence from a meta-analysis. Med. Oncol. 2014, 31, 125. [Google Scholar] [CrossRef]
- Fardet, A. New hypotheses for the health-protective mechanisms of whole-grain cereals: What is beyond fibre? Nutr. Res. Rev. 2010, 23, 65–134. [Google Scholar] [CrossRef] [Green Version]
- Bach Knudsen, K.E.; Norskov, N.P.; Bolvig, A.K.; Hedemann, M.S.; Laerke, H.N. Dietary fibers and associated phytochemicals in cereals. Mol. Nutr. Food Res. 2017, 61. [Google Scholar] [CrossRef]
- Kranz, S.; Dodd, K.W.; Juan, W.Y.; Johnson, L.K.; Jahns, L. Whole grains contribute only a small proportion of dietary fiber to the U.S. diet. Nutrients 2017, 9, 153. [Google Scholar] [CrossRef] [PubMed]
- Ahluwalia, N.; Herrick, K.A.; Terry, A.L.; Hughes, J.P. Contribution of Whole Grains to Total Grains Intake among Adults Aged 20 and over: United States, 2013–2016; NCHS Data Brief No. 341; CDC: Atlanta, GA, USA, 2019.
Figure 1.
Flow chart of publication selection (see text for further details on search terms and filters used).
Figure 1.
Flow chart of publication selection (see text for further details on search terms and filters used).


{kind=link}
Table 1.
Whole grain intake and risk of cancer mortality *: Results from meta-analyses of observational cohort and case-control studies.
Table 1.
Whole grain intake and risk of cancer mortality *: Results from meta-analyses of observational cohort and case-control studies.
| Meta-Analysis | Highest vs. Lowest Intakes | Dose Response | ||
|---|---|---|---|---|
| Number of Cohorts or Case-Control Studies Included [References] | Relative Risk or Odds Ratio (95% CI) | Number of Cohorts or Case-Control Studies Included [References] | Relative Risk or Odds Ratio (95% CI) | |
| Jacobs et al., 1998 [24] | 45 [41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80] | 0.66 (0.60–0.72) | ||
| Aune et al., 2016 [20] | 6 [81,82,83,84,85] | 0.89 (0.82–0.96) | 6 [81,82,83,84,85] | 0.85 (0.80–0.91) 90 g/day |
| Benisi-Kohansel et al., 2016 [21] | 7 [81,82,83,85,86,87] | 0.94 (0.91–0.98) | 3 [82,83,85] | 0.90 (0.83–0.98) 90 g/day |
| Chen et al., 2016 [22] | 8 [81,82,83,84,85,87,88] | 0.89 (0.84–0.95) | 6 [81,82,83,84,85] | 0.82 (0.69–0.86) 50 g/day |
| Wei et al., 2016 [29] | 8 [81,82,83,84,85,87] | 0.89 (0.82–0.96) | 7 [81,82,83,84,85] | 0.91 (0.84–0.98) 90 g/day |
| Zong et al., 2016 [33] | 10 [82,83,84,85,87,88] | 0.88 (0.83–0.94) | 10 [82,83,84,85,87,88] | 0.80 (0.72–0.89) 70 g/day 0.85 (0.76–0.94) 50 g/day 0.89 (0.79–0.99) 30 g/day 0.96 (0.91–1.01) 10 g/day |
| Zhang et al., 2018 [31] | 14 [82,85,87,89,90,91,92,93,94,95,96,97] | 0.94 (0.87–1.01) | 14 [82,85,87,89,90,91,92,93,94,95,96,97] | 0.97 (0.95–0.99) 28 g/day |
| Reynolds et al., 2019 [26] | 5 [81,82,83,84,85] | 0.84 (0.76–0.92) | 7 [81,82,83,84,85] | 0.95 (0.93–0.97) 15 g/day |
CI = confidence interval; * all meta-analyses reported total cancer mortality except for the case-control meta-analysis of Jacobs et al., who reported total cancer risk for multiple sites combined. Unfilled field indicates that no meta-analyses were performed. g/day refers to the dose of whole grain intake associated with the corresponding relative risk or odds ratio in the dose-response analysis.
Table 2.
Whole grain intake and risk of site-specific cancer: Results from meta-analyses of observational cohort and case-control studies.
Table 2.
Whole grain intake and risk of site-specific cancer: Results from meta-analyses of observational cohort and case-control studies.
| Meta-Analysis | Highest vs. Lowest Intakes | Dose Response | Cancer Site | ||
|---|---|---|---|---|---|
| Number of Cohorts or Case-Control Studies Included [References] | Relative Risk or Odds Ratio (95% CI) | Number of Cohorts or Case-Control Studies Included [References] | Relative Risk or Odds Ratio (95% CI) | ||
| Jacobs et al., 1998 [24] | 7 [41,46,61,68,69,71,75] | 0.79 (0.69–0.89) | Colorectal | ||
| Aune et al., 2011 [19] | 4 [95,98,99,100] | 0.79 (0.72–0.86) | 6 [95,98,99,100,101] | 0.83 (0.78–0.89) | Colorectal 90 g/day |
| Vieira et al., 2017 [28] | 6 [94,95,100,102] | 0.83 (0.79–0.89) | Colorectal 90 g/day | ||
| Schwingshackl et al., 2018 [16] | 10 [90,94,95,99,100,101,102,103,104] | 0.88 (0.83–0.94) | 9 [90,94,95,99,100,101,102,104] | 0.95 (0.93–0.97) | Colorectal 30 g/day |
| Reynolds et al., 2019 [26] | 7 [90,94,95,98,101,102,105] | 0.87 (0.79–0.96) | 8 [90,94,95,98,101,102,105] | 0.97 (0.95–0.99) | Colorectal 15 g/day |
| Zhang et al., 2020 [32] | 25 [46,68,71,90,94,95,98,99,100,101,105,106,107,108,109,110,111,112] | 0.89 (0.84–0.93) | Colorectal | ||
| Aune et al., 2011 [19] | 5 [95,98,100,105,112] | 0.82 (0.72–0.92) | 4 [95,98,100,105] | 0.86 (0.79–0.94) | Colon 90 g/day |
| Vieira et al., 2017 [28] | 4 [94,95,100,105] | 0.82 (0.73–0.92) | Colon 90 g/day | ||
| Schwingshackl et al., 2018 [16] | 7 [90,94,95,100,104,105,112] | 0.85 (0.77–0.93) | 6 [90,94,95,100,104] | 0.97 (0.95–0.99) | Colon 30 g/day |
| Aune et al., 2011 [19] | 3 [95,98,100] | 0.80 (0.59–1.07) | 3 [95,98,100] | 0.80 (0.56–1.14) | Rectal 90 g/day |
| Vieira et al., 2017 [28] | 3 [94,95,100] | 0.81 (0.54–1.20) | Rectal 90 g/day | ||
| Schwingshackl et al., 2018 [16] | 5 [90,94,95,100,104] | 0.80 (0.64–0.98) | 5 [90,94,95,100,104] | 0.94 (0.88–1.01) | Rectal 30 g/day |
| Jacobs et al., 1998 [24] | 7 [42,43,54,59,74,76,79] | 0.57 (0.47–0.67) | Gastric | ||
| Wang et al., 2020 [35] | 5 [42,43,113,114,115] | 0.87 (0.79–0.95) | Gastric | ||
| Xu et al., 2019 [36] | 3 [116,117,118] | 0.61 (0.40–0.83) | Gastric | ||
| Zhang et al., 2020 [32] | 12 [42,43,54,79,113,115,116,117,118,119,120] | 0.64 (0.53–0.79) | Gastric | ||
| Jacobs et al., 1998 [24] | 4 [45,52,65,67] | 0.70 (0.54–0.86) | Pancreatic | ||
| Lei et al., 2016 [25] | 5 [24,121,122,123,124] | 0.76 (0.64–0.91) | Pancreatic | ||
| Wang et al., 2015 [34] | 8 [91,96,125,126,127,128,129,130] | 1.13 (0.98–1.30) | Prostate | ||
| Reynolds et al., 2019 [26] | 3 [91,96,127] | 1.10 (1.02–1.19) | 2 [91,96,127] | 1.02 (0.98–1.05) | Prostate 15 g/day |
| Jacobs et al., 1998 [24] | 2 [56,64] | 0.86 (0.67–1.05) | Breast | ||
| Xiao et al., 2018 [30] | 11 [56,64,92,125,131,132,133,134,135,136,137] | 0.84 (0.74–0.96) | 6 [92,131,132,135,136,137] | 0.83 (0.73–0.93) | Breast 50 g/day |
| Jacobs et al., 1998 [24] | 2 [47,80] | 0.52 (0.09–0.95) | Esophageal | ||
| Zhang et al., 2020 [32] | 7 [117,138,139,140,141,142] | 0.54 (0.44–0.67) | Esophageal | ||
| Jacobs et al., 1998 [24] | 4 [48,58,66,77] | 0.57 (0.38–0.76) | Oral | ||
| Jacobs et al., 1998 [24] | 2 [44,51] | 0.67 (0.48–0.86) | Brain | ||
| Jacobs et al., 1998 [24] | 3 [53,55,63] | 0.55 (0.41–0.69) | Endometrial | ||
| Jacobs et al., 1998 [24] | 2 [50,73] | 0.41 (0.37–0.45) | Non-Hodgkin’s lymphoma | ||
CI = confidence interval. Unfilled fields indicate that no meta-analyses were performed. g/day refers to the dose of whole grain intake associated with the corresponding relative risk or odds ratio in the dose-response analysis.
Table 3.
Refined grain intake and cancer risk: Results from meta-analyses of observational cohort and case-control studies.
Table 3.
Refined grain intake and cancer risk: Results from meta-analyses of observational cohort and case-control studies.
| Meta-Analysis | Highest vs. Lowest Intakes | Dose Response | Cancer | ||
|---|---|---|---|---|---|
| Number of Cohorts or Case-Control Studies Included [References] | Relative Risk or Odds Ratio (95% CI) | Number of Cohorts or Case-Control Studies Included [References] | Relative Risk or Odds Ratio (95% CI) | ||
| Aune et al., 2016 [20] | 2 [83,85] | 0.94 (0.90–0.99) | Total cancer 90 g/day | ||
| Schwingshackl et al., 2018 [16] | 2 [95,103] | 1.46 (0.80–2.67) | Colorectal | ||
| Schwingshackl et al., 2018 [16] | 2 [95,112] | 1.27 (1.02–1.57) | Colon | ||
| Xu et al., 2019 [36] | 3 [116,117,118] | 1.65 (1.36–1.94) | Gastric | ||
| Wang et al., 2020 [35] | 18 [54,59,113,114,116,118,143,144,145,146,147,148,149,150,151,152] | 1.36 (1.21–1.54) | Gastric | ||
CI = confidence interval. Unfilled fields indicate that no meta-analyses were performed. g/day refers to the dose of whole grain intake associated with the corresponding relative risk or odds ratio in the dose-response analysis.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Gaesser, G.A. Whole Grains, Refined Grains, and Cancer Risk: A Systematic Review of Meta-Analyses of Observational Studies. Nutrients 2020, 12, 3756. https://doi.org/10.3390/nu12123756
AMA Style
Gaesser GA. Whole Grains, Refined Grains, and Cancer Risk: A Systematic Review of Meta-Analyses of Observational Studies. Nutrients. 2020; 12(12):3756. https://doi.org/10.3390/nu12123756
Chicago/Turabian StyleGaesser, Glenn A. 2020. "Whole Grains, Refined Grains, and Cancer Risk: A Systematic Review of Meta-Analyses of Observational Studies" Nutrients 12, no. 12: 3756. https://doi.org/10.3390/nu12123756
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.