Dietary Changes over 25 Years in Tianjin Residents: Findings from the 1986–1988, 2000–2004, and 2008–2011 Nutrition Surveys

Abstract
:1. Introduction
2. Experimental Section
2.1. Data Sources and Subjects

{kind=link}
{kind=link}
| Population Group | 1986–1988 | 2000–2004 | 2008–2011 | |||
|---|---|---|---|---|---|---|
| Urban (%) | Rural (%) | Urban (%) | Rural (%) | Urban (%) | Rural (%) | |
| Sex | ||||||
| Male | 7061 (48.5) | 1603 (49.3) | 8076 (49.1) | 5426 (49.4) | 4674 (47.2) | 3737 (49.0) |
| Female | 7488 (51.5) | 1649 (50.7) | 8385 (50.9) | 5555 (50.6) | 5222 (52.8) | 3891 (51.0) |
| Total | 14,549 | 3252 | 16,461 | 10,981 | 9896 | 7628 |
| Age (years) | ||||||
| 18–29 | 3577 (24.6) | 826 (25.3) | 2316 (14.1) | 2888 (26.3) | 1017 (10.3) | 1985 (26.0) |
| 30–39 | 3334 (22.9) | 760 (23.4) | 4111 (25.0) | 2712 (24.7) | 2723 (27.5) | 1840 (24.1) |
| 40–49 | 2990 (20.6) | 659 (20.3) | 3137 (19.0) | 2559 (23.3) | 2672 (27.0) | 1755 (23.0) |
| 50–59 | 2464 (16.9) | 650 (20.0) | 3979 (24.2) | 1787 (16.3) | 1898 (19.2) | 1419 (18.6) |
| 60– | 2184 (15.0) | 357 (11.0) | 2918 (17.7) | 1035 (9.4) | 1586 (16.0) | 629 (8.3) |
| Total | 14,549 | 3252 | 16,461 | 10,981 | 9896 | 7628 |
2.2. Dietary Analysis

2.3. Statistical Analysis
3. Results
3.1. Food Consumption Patterns
3.1.1. Proportions for Different Food Groups
3.1.2. Average Intakes for Different Food Groups
Cereals
Vegetables and Fruits
Animal Foods
Beans and Bean Products
| Food Category | Urban | Rural | 2002 NNHS | Food Guide a | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1986–1988 | 2000–2004 | 2008–2011 | p Value | 1986–1988 | 2000–2004 | 2008–2011 | p Value | Urban | Rural | in 2007 | |
| Plant foods | |||||||||||
| Cereals and grain products | 394.67 ± 41.97 | 242.06 ± 10.12 ** | 391.22 ± 40.77 ## | 0.000 | 483.03 ± 34.95 | 464.49 ± 84.28 | 442.26 ± 31.41 | 0.807 | 366.1 | 415.3 | 250~400 b |
| Potatoes and starches | 39.03 ± 16.27 | 36.00 ± 2.29 | 29.92 ± 4.04 | 0.565 | 31.30 ± 6.9 | 33.33 ± 11.80 | 42.67 ± 13.72 | 0.523 | 31.9 | 56.2 | --- |
| Beans and their products | 21.23 ± 5.49 | 15.51 ± 10.52 | 98.28 ± 24.80 **## | 0.000 | 12.23 ± 2.56 | 10.14 ± 6.67 | 65.44 ± 20.60 **## | 0.001 | 15.5 | 16.2 | 30–50 |
| Vegetables | 272.67 ± 58.52 | 374.62 ± 19.62 * | 289.07 ± 82.72 | 0.011 | 203.83 ± 46.98 | 320.76 ± 66.8 | 279.34 ± 58.96 | 0.069 | 251.9 | 284.1 | 300–500 |
| Fruits | 48.27 ± 6.90 | 208.82 ± 14.10 ** | 220.49 ± 58.23 ** | 0.000 | 8.67 ± 6.40 | 89.45 ± 5.67 ** | 219.18 ± 56.38 **## | 0.000 | 69.3 | 36.6 | 200–400 |
| Vegetable oils | 37.63 ± 7.50 | 24.10 ± 2.61 ** | 27.23 ± 4.63 * | 0.018 | 17.00 ± 3.84 | 25.11 ± 2.60 | 29.76 ± 5.43 * | 0.012 | 40.2 | 29.9 | 25–30 c |
| others | 56.90 ± 28.40 | 66.20 ± 11.39 | 89.15 ± 35.11 | 0.323 | 20.97 ± 6.73 | 10.61 ± 0.61 | 76.00 ± 20.23 **## | 0.000 | --- | --- | --- |
| Animal foods | |||||||||||
| Meats and poultry and their products | 83.50 ± 2.34 | 96.21 ± 3.65 | 80.34 ± 14.04 # | 0.024 | 19.93 ± 4.84 | 32.14 ± 0.69 * | 64.40 ± 8.51 **## | 0.000 | 104.4 | 69.9 | 50–75 |
| Fish and shellfish | 62.50 ± 8.34 | 49.62 ± 12.67 | 48.58 ± 7.88 | 0.206 | 26.73 ± 8.36 | 23.13 ± 3.34 | 37.93 ± 7.18 # | 0.043 | 44.9 | 24.4 | 50–100 |
| Egg and egg products | 72.43 ± 11.96 | 54.43 ± 3.65 * | 65.53 ± 20.51 * | 0.018 | 29.87 ± 5.76 | 38.53 ± 8.14 | 60.72 ± 23.70 | 0.062 | 33.2 | 19.9 | 25–50 |
| Milk and dairy products | 44.00 ± 6.71 | 61.32 ± 13.39 | 74.19 ± 2.78 # | 0.045 | 0.13 ± 0.06 | 7.20 ± 9.32 | 22.92 ± 10.02 * | 0.046 | 65.8 | 11.2 | 300 |
| Animal oils and fats | 0.70 ± 0.17 | 0.08 ± 0.05 ** | 1.34 ± 0.84 ## | 0.007 | 6.47 ± 2.27 | 2.31 ± 0.73 * | 3.93 ± 0.97* | 0.013 | 3.8 | 10.5 | --- |
| Total | 1133.53 ± 62.02 | 1228.97 ± 70.48 | 1415.34 ± 44.18 ** | 0.006 | 860.16 ± 12.17 | 1057. 20 ± 39.56 * | 1344.55 ± 60.54 **# | 0.000 | --- | --- | --- |
Oils
3.2. Caloric and Nutrient Intakes
3.2.1. Caloric Intakes
3.2.2. Nutrients Intakes and Selected Nutrients Intakes as Percent of RNI or AI
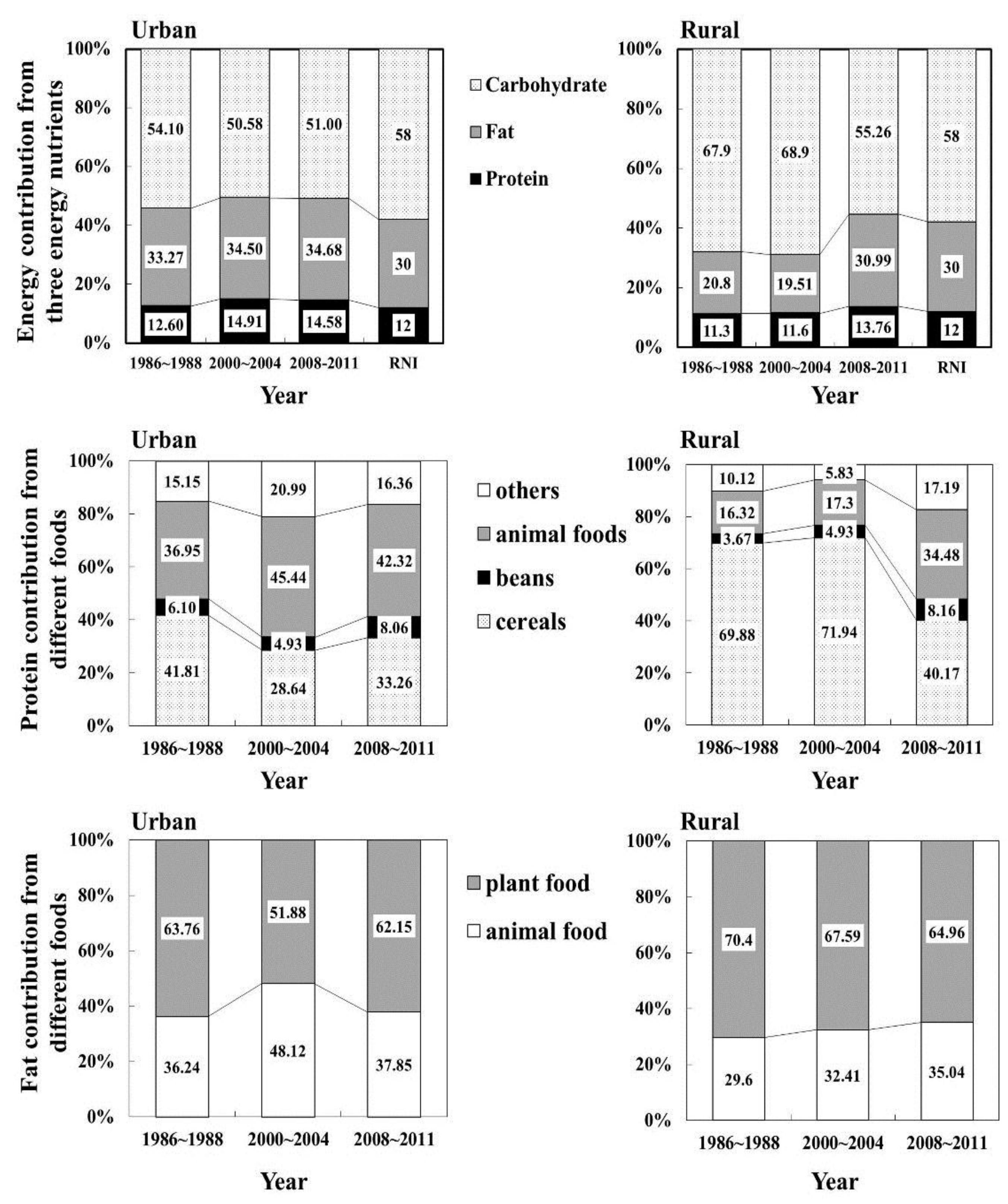
3.3. Composition of Energy, Protein and Fat
| Energy/Nutrients | Urban | Rural | RNI/AI | ||||||
|---|---|---|---|---|---|---|---|---|---|
| 1986–1988 | 2000–2004 | 2008–2011 | p Value | 1986–1988 | 2000–2004 | 2008–2011 | p Value | ||
| (%) | (%) | (%) | (%) | (%) | (%) | ||||
| Energy (kcal) | 2649.07 ± 272.18 | 1977.61 ± 92.86 ** | 2142.45 ± 156.31 * | 0.003 | 2290.77 ± 71.12 | 2421.90 ± 96.30 | 2280.49 ± 38.91 | 0.098 | 2400 |
| (110.38) | (82.40) | (89.25) | (95.45) | (100.91) | (95.02) | ||||
| Protein (g) | 83.63 ± 7.07 | 73.81 ± 4.97 | 78.08 ± 1.05 | 0.104 | 64.60 ± 2.31 | 70.26 ± 4.29 | 78.41 ± 0.58 ** | 0.010 | 75 |
| (111.51) | (98.41) | (104.11) | (86.13) | (93.68) | (104.55) | ||||
| Fat (g) | 98.20 ± 13.95 | 75.91 ± 4.85 * | 81.21 ± 5.16 | 0.025 | 52.83 ± 4.25 | 52.47 ± 2.34 | 78.43 ± 9.09 **## | 0.001 | |
| Carbohydrate (g) | 357.57 ± 33.42 | 250.19 ± 10.37 ** | 275.02 ± 26.11 * | 0.001 | 389.87 ± 25.54 | 417.45 ± 20.00 | 315.24 ± 30.77 *## | 0.004 | |
| Dietary fiber (g) | 6.03 ± 0.55 | 10.13 ± 0.50 | 17.20 ± 7.95 **# | 0.015 | 5.27 ± 0.32 | 16.24 ± 2.58 ** | 18.41 ± 7.82 **## | 0.006 | 25 |
| (24.12) | (40.52) | (68.80) | (21.08) | (64.96) | (73.64) | ||||
| Retinol Equiv. (μg) | 1377.00 ± 136.54 | 444.38 ± 122.22 ** | 624.15 ± 27.10 ** | 0.000 | 590.20 ± 73.72 | 426.469 ± 153.89 | 576.24 ± 94.85 | 0.217 | 800 |
| (172.13) | (55.55) | (78.02) | (73.78) | (53.31) | (72.03) | ||||
| Thiamine (mg) | 1.93 ± 0.40 | 1.01 ± 0.08 | 1.10 ± 0.10 | 0.002 | 2.40 ± 0.17 | 1.44 ± 0.14 ** | 1.12 ± 0.07 ** | 0.000 | 1.4 |
| (137.86) | (72.14) | (78.57) | (171.43) | (102.86) | (80.00) | ||||
| Riboflavin (mg) | 1.13 ± 0.12 | 1.10 ± 0.08 ** | 1.16 ± 0.17 * | 0.744 | 0.73 ± 0.06 | 0.75 ± 0.04 | 1.14 ± 0.20 **## | 0.002 | 1.4 |
| (80.71) | (78.57) | (82.86) | (52.14) | (53.57) | (81.43) | ||||
| Niacin (mg) | 15.33 ± 0.85 | 18.05 ± 0.72 ** | 17.03 ± 0.22 | 0.004 | 14.40 ± 0.46 | 15.09 ± 0.76 | 16.91 ± 0.39 **# | 0.010 | 14 |
| (109.5) | (128.93) | (121.64) | (102.86) | (107.79) | (120.78) | ||||
| Ascorbic acid (mg) | 94.00 ± 21.17 | 165.43 ± 45.41 | 101.33 ± 0.03 | 0.055 | 58.13 ± 11.02 | 85.20 ± 24.19 | 95.29 ± 8.57 | 0.137 | 100 |
| (94.00) | (165.43) | (101.33) | (58.13) | (85.2) | (95.29) | ||||
| Calcium (mg) | 475.1 ± 67.05 | 611.25 ± 92.44 | 625.15 ± 57.97 | 0.936 | 406.83 ± 30.03 | 482.40 ± 34.29 * | 504.86 ± 97.01 **## | 0.000 | 800 |
| (59.39) | (76.41) | (78.14) | (50.85) | (60.3) | (63.11) | ||||
| Iron (mg) | 28.03 ± 2.80 | 24.20 ± 1.24 | 24.02 ± 2.88 | 0.081 | 25.90 ± 1.21 | 20.76 ± 1.36 | 25.26 ± 1.12 **# | 0.002 | 15 |
| (186.87) | (161.33) | (160.13) | (172.67) | (138.4) | (168.4) | ||||
| Zinc (mg) | 11.51 ± 1.07 | 12.09 ± 1.41 | 12.90 ± 1.43 | 0.546 | 10.12 ± 0.36 | 13.22 ± 0.43 * | 12.87 ± 1.47 * | 0.001 | 15 |
| (76.73) | (80.60) | (86.00) | (67.47) | (88.13) | (85.8) | ||||
| Selenium (μg) | 46.93 ± 3.67 | 60.51 ± 8.93 | 64.28 ± 3.52 | 0.053 | 25.31 ± 0.49 | 40.52 ± 2.06 * | 61.70 ± 7.17 **# | 0.000 | 50 |
| (93.86) | (121.02) | (128.56) | (50.62) | (81.04) | (123.4) | ||||
| Cholesterol (mg) | 486.26 ± 58.29 | 498.69 ± 45.93 | 509.72 ± 107.69 | 0.916 | 191.53 ± 29.71 | 247.82 ± 54.93 | 451.27 ± 25.03 **## | 0.001 | 300 |
| (162.09) | (166.23) | (169.91) | (63.84) | (82.61) | (150.42) | ||||
| Food Category | Urban | Rural | ||||
|---|---|---|---|---|---|---|
| 1986–1988 | 2000–2004 | 2008–2011 | 1986–1988 | 2000–2004 | 2008–2011 | |
| Cereals and grain products | 48.61 | 37.54 | 41.90 | 68.68 | 74.53 | 48.73 |
| Beans and their products | 2.24 | 2.02 | 3.35 | 1.12 | 1.48 | 3.28 |
| Potatoes and starches | 1.16 | 1.45 | 1.59 | 1.05 | 0.10 | 1.48 |
| Animal foods | 16.79 | 24.54 | 20.73 | 5.18 | 7.74 | 16.56 |
| Pure energy foods | 16.51 | 16.19 | 15.24 | 17.27 | 12.04 | 15.92 |
| Others | 14.68 | 18.26 | 17.19 | 6.70 | 4.10 | 14.03 |
| Total | 100.00 | 100.00 | 100.00 | 100.00 | 100.00 | 100.00 |

4. Discussion
5. Conclusions
Supplementary Files
Supplementary File 1Acknowledgments
Author Contributions
Conflicts of Interest
References
- Popkin, B.M. Will China’s Nutrition Transition Overwhelm Its Health Care System and Slow Economic Growth? Health Aff. 2008, 27, 1064–1076. [Google Scholar] [CrossRef] [PubMed]
- Du, S.; Lu, B.; Zhai, F.; Popkin, B.M. A New Stage of the Nutrition Transition in China. Public Health Nutr. 2002, 5, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Piazza, A. Food Consumption and Nutritional Status in the P.R.C. In Westview Special Studies on East Asia; Westview Press: Boulder, CO, USA, 1986. [Google Scholar]
- Popkin, B.M.; Keyou, G.; Zhai, F.; Guo, X.; Ma, H.; Zohoori, N. The nutrition transition in China: A cross-sectional analysis. Eur. J. Clin. Nutr. 1993, 47, 333–346. [Google Scholar] [PubMed]
- World Bank. World Development Indicators; World Bank: Washington, DC, USA, 2009. [Google Scholar]
- Campbell, T.C.; Parpia, B.; Chen, J. Diet, lifestyle, and the etiology of coronary artery disease: The Cornell China study. Am. J. Cardiol. 1998, 82, 18T–21T. [Google Scholar] [CrossRef]
- Popkin, B.M.; Horton, S.; Kim, S.; Mahal, A.; Shuigao, J. Trends in diet, nutritional status, and diet-related noncommunicable diseases in China and India: The economic costs of the nutrition transition. Nutr. Rev. 2001, 59, 379–390. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B.M.; Horton, S.; Kim, S. The Nutrition Transition and Prevention of Diet-Related Chronic Diseases in Asia and the Pacific. Food Nutr. Bull. 2001, 22, s1–s58. [Google Scholar]
- Popkin, B.M.; Kim, S.; Rusev, E.R.; Du, S.; Zizza, C. Measuring the full economic costs of diet, physical activity and obesity-related chronic diseases. Obes. Rev. 2006, 7, 271–293. [Google Scholar] [CrossRef] [PubMed]
- Zhai, F.; Wang, H.; Du, S.; He, Y.; Wang, Z.; Ge, K.; Popkin, B.M. Prospective study on nutrition transition in China. Nutr. Rev. 2009, 67, S56–S61. [Google Scholar] [CrossRef] [PubMed]
- Ge, K. The transition of Chinese dietary guidelines and food guide pagoda. Asia Pac. J. Clin. Nutr. 2011, 20, 439–446. [Google Scholar] [PubMed]
- Wang, D.S.; Xu, G.C.; Wang, Z.L.; Che, S.P.; Mo, J.X.; Ren, D.L.; Jin, J.M.; Zhang, W.Q. Nutritional problems and improvement measures of Tianjin urban and rural residents dietary. Tianjin Yi Xue Yuan Xue Bao 1991, 15, 1–6. [Google Scholar]
- Wang, X.; Huang, G.W.; Tian, H.G.; Dong, S.R.; Yin, H.G.; Cao, X.H. Investigation on dietary nutrition of urban residents in Tianjin from 2000 to 2004. Chin. J. Public Health 2007, 23, 1245–1247. [Google Scholar]
- Huang, G.W.; Tian, H.G.; Wang, X.; Dong, S.R.; Yin, H.G.; Cao, X.H. Dietary survey of urban and rural residents in tianjin from 2000 to 2004. Acta Nutr. Sin. 2007, 29, 435–437. [Google Scholar]
- Li, Y.; He, Y.; Zhai, F.; Yang, X.; Hu, X.; Zhao, W.; Ma, G.S. Comparison of assessment of food intakes by using 3 dietary survey methods. Clin. J. Prev. Med. 2006, 40, 273–280. [Google Scholar]
- Yang, Y.X.; Wang, G.Y.; Pan, X.C. Chinese Center for Disease Control and Prevention nutrition and food security. In China Food Composition; Peking University Medical Press: Peking, China, 2009. [Google Scholar]
- Wang, L.D. Comprehensive Report of Chinese National Nutrition and Health Survey in 2002; People‘s Medical Publishing House: Peking, China, 2005. [Google Scholar]
- Zhai, F.Y.; He, Y.N.; Ma, G.S.; Li, Y.P.; Wang, Z.H.; Hu, Y.S.; Zhao, L.Y.; Cui, Z.H.; Li, Y.; Yang, X.G. Study on the current status and trend of food consumption among Chinese population. Zhonghua Liu Xing Bing Xue Za Zhi 2005, 26, 485–488. [Google Scholar] [PubMed]
- Chinese Nutrition Society. Dietary Guidelines for Chinese Residents; The Tibet People’s Publishing House: Tibet, China, 2010. [Google Scholar]
- National Bureau of Statistics of China. Indices for Total Amount and Rapidity of Socioeconomic Development. In Part 1–2, China Statistical yearbook 2010; China Statistical Publisher: Beijing. Available online: http://www.stats.gov.cn/tjsj/ndsj/ (accessed on 14 January 2016).
- Liang, H.; Huang, W.; Wang, J.Y. Shenzhen citizens’ cognitive level on “Guidance on Chinese people’s Meal Nutrition”. Occup. Health 2005, 21, 10–13. [Google Scholar]
- Popkin, B.M. An overview on the nutrition transition and its health implications: The Bellagio meeting. Public Health Nutr. 2002, 5, 93–103. [Google Scholar] [PubMed]
- Popkin, B.M. The Nutrition Transition in the Developing World. Dev. Policy Rev. 2003, 21, 581–597. [Google Scholar] [CrossRef]
- Wang, H.; Du, S.; Zhai, F.; Popkin, B.M. Trends in the distribution of body mass index among Chinese adults, aged 20–45 years (1989–2000). Int. J. Obes. (Lond.) 2007, 31, 272–278. [Google Scholar] [CrossRef] [PubMed]
- Beaglehole, R. Global cardiovascular disease prevention: Time to get serious. Lancet 2001, 358, 661–663. [Google Scholar] [CrossRef]
- Ezzati, M.; Lopez, A.D.; Rodgers, A.; Vander Hoorn, S.; Murray, C.J.; Comparative Risk Assessment Collaborating Group. Selected major risk factors and global and regional burden of disease. Lancet 2002, 360, 1347–1360. [Google Scholar] [CrossRef]
- Popkin, B.M. Understanding global nutrition dynamics as a step towards controlling cancer incidence. Nat. Rev. Cancer 2007, 7, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Critchley, J.; Liu, J.; Zhao, D.; Wei, W.; Capewell, S. Explaining the increase in coronary heart disease mortality in Beijing between 1984 and 1999. Circulation 2004, 110, 1236–1244. [Google Scholar] [CrossRef] [PubMed]
- Wallingford, J.C.; Yuhas, R.; Du, S.; Zhai, F.; Popkin, B.M. Fatty acids in Chinese edible oils: Value of direct analysis as a basis for labeling. Food Nutr. Bull. 2004, 25, 330–336. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B.M.; Du, S. Dynamics of the nutrition transition toward the animal foods sector in China and its implications: A worried perspective. J. Nutr. 2003, 133, S3898–S3906. [Google Scholar]
- Jing, Y.; Lu, G.S.; Wang, L.; Zhou, Y.J.; Sun, J.; Bai, Y. Epidemiological study of anemia in 18 to 60 years old population in Tianjin area. J. Prev. Med. Clin. PLA 2012, 30, 406–408. [Google Scholar]
- Basuli, D.; Stevens, R.G.; Torti, F.M.; Torti, S.V. Epidemiological associations between iron and cardiovascular disease and diabetes. Front. Pharmacol. 2014, 5, 117. [Google Scholar] [PubMed]
- Felipe, A.; Guadalupe, E.; Druso, P.; Carlos, M.; Pablo, S.; Oscar, C.; Luis, V.; Diego, M.; Jaime, R.; Inés, U.; Federico, L. Serum Ferritin Is Associated with Metabolic Syndrome and Red Meat Consumption. Oxid. Med. Cell. Longev. 2015, 2015, 769739. [Google Scholar] [CrossRef] [PubMed]
- Du, S.; Mroz, TA.; Zhai, F.; Popkin, B.M. Rapid income growth adversely affects diet quality in China–particularly for the poor! Soc. Sci. Med. 2004, 59, 1505–1515. [Google Scholar] [CrossRef] [PubMed]
- Foster, G.D.; Wyatt, H.R.; Hill, J.O.; McGuckin, B.G.; Brill, C.; Mohammed, B.S.; Szapary, P.O.; Rader, D.J.; Edman, J.S.; Klein, S. A randomized trial of a low-carbohydrate diet for obesity. N. Engl. J. Med. 2003, 348, 2082–2090. [Google Scholar] [CrossRef] [PubMed]
- Leitzmann, C. Vegetarian diets: What are the advantages? Forum Nutr. 2005, 57, 147–156. [Google Scholar] [PubMed]
- Sabaté, J. The contribution of vegetarian diets to human health. Forum Nutr. 2003, 56, 218–220. [Google Scholar] [PubMed]
- Dietary Guidelines for Americans 2010. Available online: http://health.gov/dietaryguidelines/dga2010/DietaryGuidelines2010.pdf (accessed on 14 January 2016).
- Astrup, A.; Meinert Larsen, T.; Harper, A. Atkins and other low-carbohydrate diets: Hoax or an effective tool for weight loss? Lancet 2004, 364, 897–899. [Google Scholar] [CrossRef]
- Dansinger, M.L.; Gleason, J.A.; Griffith, J.L.; Selker, H.P.; Schaefer, E.J. Comparison of the Atkins, Ornish, Weight Watchers, and Zone diets for weight loss and heart disease risk reduction: A randomized trial. JAMA 2005, 293, 43–53. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Yang, J.; Marventano, S.; Micek, A.; Galvano, F.; Kales, S.N. Nut consumption on all-cause, cardiovascular, and cancer mortality risk: A systematic review and meta-analysis of epidemiologic studies. Am. J. Clin. Nutr. 2015, 101, 783–793. [Google Scholar] [CrossRef] [PubMed]
- Gerber, P.J.; Vellinga, T.V.; Steinfeld, H. Issues and options in addressing the environmental consequences of livestock sector’s growth. Meat Sci. 2010, 84, 244–247. [Google Scholar] [CrossRef] [PubMed]
- Horrigan, L.; Lawrence, R.S.; Walker, P. How sustainable agriculture can address the environmental and human health harms of industrial agriculture. Environ. Health Perspect. 2002, 110, 445–456. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Beydoun, M.A.; Caballero, B.; Gary, T.L.; Lawrence, R. Trends and correlates in meat consumption patterns in the US adult population. Public Health Nutr. 2010, 13, 1333–1345. [Google Scholar] [CrossRef] [PubMed]
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, X.; Wu, Y.; Zhang, X.; Zhang, M.; Huang, G. Dietary Changes over 25 Years in Tianjin Residents: Findings from the 1986–1988, 2000–2004, and 2008–2011 Nutrition Surveys. Nutrients 2016, 8, 62. https://doi.org/10.3390/nu8020062
Wang X, Wu Y, Zhang X, Zhang M, Huang G. Dietary Changes over 25 Years in Tianjin Residents: Findings from the 1986–1988, 2000–2004, and 2008–2011 Nutrition Surveys. Nutrients. 2016; 8(2):62. https://doi.org/10.3390/nu8020062
Chicago/Turabian StyleWang, Xuan, Yuntang Wu, Xumei Zhang, Meilin Zhang, and Guowei Huang. 2016. "Dietary Changes over 25 Years in Tianjin Residents: Findings from the 1986–1988, 2000–2004, and 2008–2011 Nutrition Surveys" Nutrients 8, no. 2: 62. https://doi.org/10.3390/nu8020062