
How to Treat Hepatocellular Carcinoma in Elderly Patients

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
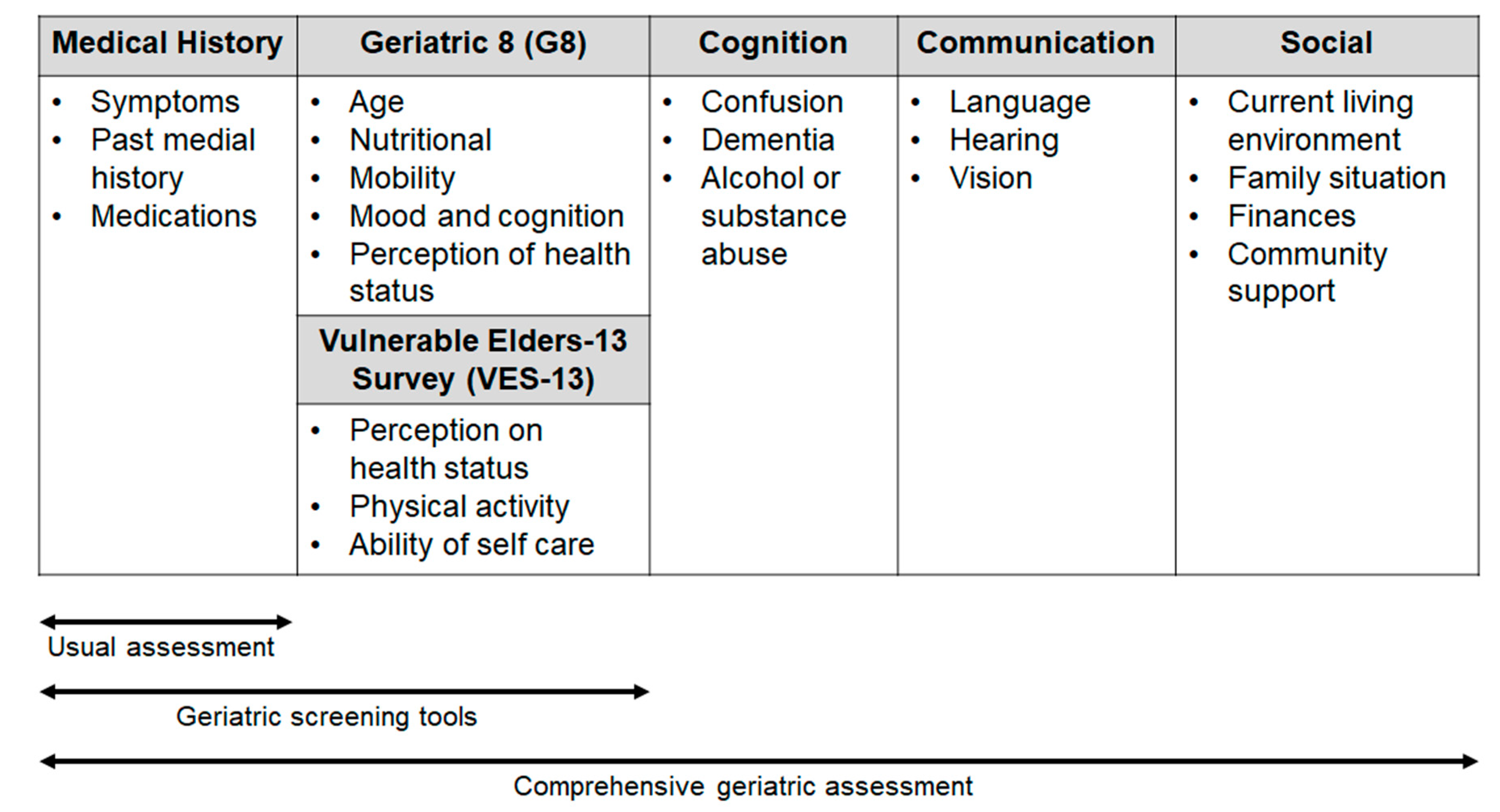
2. Geriatric Assessment and Scales: A Tool to Choose a Tailored Treatment for Elderly HCC Patients
3. HCC Treatment in Elderly Patients According to BCLC Stage
3.1. Early Stage HCC (BCLC Stage 0 or A)
3.1.1. Liver Transplantation
3.1.2. Liver Resection
3.1.3. Local Ablative Approaches
3.2. Intermediate-Stage HCC (BCLC Stage B)
3.3. Advanced Stage HCC (BCLC Stage C)
3.3.1. First-Line Treatment
3.3.2. Second-Line Treatment
3.3.3. Comorbidities and Contraindications
3.3.4. A Focus on Sarcopenia in Elderly HCC Patients
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- AIOM; AIRTUM Working Group. I Numeri del Cancro in Italia 2020; Intermedia Editore: Attigliano, Italy, 2020. [Google Scholar]
- Federico, P.; Petrillo, A.; Giordano, P.; Bosso, D.; Fabbrocini, A.; Ottaviano, M.; Rosanova, M.; Silvestri, A.; Tufo, A.; Cozzolino, A.; et al. Immune Checkpoint Inhibitors in Hepatocellular Carcinoma: Current Status and Novel Perspectives. Cancers 2020, 12, 3025. [Google Scholar] [CrossRef] [PubMed]
- Vogel, A.; Cervantes, A.; Chau, J.; Daniele, B.; Llovet, J.; Meyer, T.; Nault, J.; Neumann, U.; Ricke, C.; Sangro, B.; et al. Hepatocellular Carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29, iv238–iv255. [Google Scholar] [CrossRef]
- Llovet, J.M.; Fuster, J.; Bruix, J.; Barcelona-Clínic Liver Cancer Group. The Barcelona approach: Diagnosis, staging, and treatment of hepatocellular carcinoma. Liver Transplant. 2004, 10, S115–S120. [Google Scholar] [CrossRef] [PubMed]
- Hung, A.K.; Guy, J. Hepatocellular carcinoma in the elderly: Meta-analysis and systematic literature review. World J. Gastroenterol. 2015, 21, 12197–12210. [Google Scholar] [CrossRef]
- Yancik, R.; Ganz, P.A.; Varricchio, C.G.; Conley, B. Perspectives on comorbidity and cancer in older patient: Approaches to expend the knowledge base. J. Clin. Oncol. 2001, 19, 1147–1151. [Google Scholar] [CrossRef] [PubMed]
- Decoster, L.; van Puyvelde, S.K.; Mohile, U.; Wedding, U.; Basso, G.; Colloca, S.; Rostoft, J.; Overcash, H.; Wildiers, C.; Steer, G.; et al. Screening tools for multidimensional health problems warranting a geriatric assessment in older cancerpatients: An update on SIOG recommendations. Ann. Oncol. 2015, 26, 288–300. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Choi, H.C.; Jeong, S.H.; Lee, K.H.; Chung, J.I.; Park, Y.S.; Hwang, J.H.; Kim, J.W.; Kim, N.; Lee, N.H.; et al. Hepatocellular carcinoma in older adults: Clinical features, treatments, and survival. J. Am. Geriatr. Soc. 2011, 59, 241–250. [Google Scholar] [CrossRef]
- Berger, N.A.; Savvides, P.; Koroukian, S.M.; Kahana, E.F.; Deimling, G.T.; Rose, J.H.; Bowman, K.F.; Miller, R.H. Cancer in the elderly. Trans. Am. Clin. Climatol. Assoc. 2006, 117, 147–155. [Google Scholar] [PubMed]
- Extermann, M.; Boler, I.; Reich, R.R.; Lyman, G.H.; Brown, R.H.; DeFelice, J.; Levine, R.M.; Lubiner, E.T.; Reyes, P.; Schreiber, F.J.; et al. Predicting the risk of chemotherapy toxicity in older patients: The Chemotherapy Risk Assessment Scale for High-Age Patients (CRASH) score. Cancer 2012, 118, 3377–3386. [Google Scholar] [CrossRef] [PubMed]
- Mohile, S.G.; Dale, W.; Somerfield, M.R.; Schonberg, M.A.; Boyd, C.M.; Burhen, P.S.; Canin, B.; Cohen, H.J.; Holmes, H.M.; Hopkins, J.O.; et al. Practical assessment and management of vulnerabilities in older patients receiving chemotherapy: ASCO guideline for geriatric oncology. J. Clin. Oncol. 2018, 36, 2326–2347. [Google Scholar] [CrossRef]
- Bellera, C.A.; Rainfray, M.; Mathoulin-Pelissier, S.; Mertens, C.; Delva, F.; Fonck, M.; Soubeyran, P.L. Screening older cancer patients: First evaluation of the G-8 geriatric screening tool. Ann. Oncol. 2012, 23, 2166–2172. [Google Scholar] [CrossRef] [PubMed]
- Extermann, M.; Green, T.; Tiffenberg, G.; Rich, C.J. Validation of the senior adultoncology program (SAOP) 2 screening questionnaire. Crit. Rev. Oncol. Hematol. 2009, 69, 183–185. [Google Scholar]
- Dubianski, R.; Wildes, T.M.; Wildiers, H. SIOG guidelines-essential for good clinical practice in geriatric oncology. J. Geriatr. Oncol. 2019, 10, 196–198. [Google Scholar] [CrossRef] [PubMed]
- Stokoe, J.M.; Pearce, J.; Sinha, R.; Ring, A. G8 and VES-13 scores predict chemotherapytoxicity in older patients with cancer. J. Geriatr. Oncol. 2012, 3, S81. [Google Scholar] [CrossRef]
- Kenis, C.; Decoster, L.; van Puyvelde, K.; De Greve, J.; Conings, G.; Milisen, K.; Flamaing, J.; Lobelle, J.P.; Wildiers, H. Performance of two geriatric screening tools in older patients with cancer. J. Clin. Oncol. 2014, 32, 19–26. [Google Scholar] [CrossRef]
- Saliba, D.; Elliot, M.; Rubenstein, L.Z.; Solomon, D.H.; Young, R.T.; Kamberg, C.J.; Roth, C.; MacLean, C.H.; Shekelle, P.G.; Sloss, M.E.; et al. The Vulnetable Elders Survey: A tool for identifying vulnerable older people in the community. J. Am. Geriatr. Soc. 2001, 49, 1691–1699. [Google Scholar] [CrossRef] [Green Version]
- Soubeyran, P.; Bellera, C.; Goyard, J.; Heitz, D.; Cure, H.; Roussellot, H.; Albrand, G.; Servant, V.; Saint Jane, O.; Roy, C.; et al. Validation of the G8 screening tool in geriatriconcology: The ONCODAGE project. J. Clin. Oncol. 2011, 29. [Google Scholar] [CrossRef]
- Pottel, L.; Boterberg, T.; Pottel, H.; Goethals, L.; van Den Noortgate, N.; Duprez, F.; De Neve, F.; Rottey, S.; Geldhof, K.; van Eygen, K.; et al. Determination of an adequate screening tool for the identification of vulnerable elderly head and neck cancer patients treatedwith radio(chemo)therapy. J. Geriatr. Oncol. 2012, 3, 24–32. [Google Scholar] [CrossRef]
- Bednarsch, J.; Czigany, Z.; Heise, D.; Joechle, K.; Luedde, T.; Heij, L.; Bruners, P.; Ulmer, T.F.; Neumann, U.P.; Lang, S.A. Prognostic evaluation of HCC patients undergoing surgical resection: An analysis of 8 different staging systems. Langenbecks Arch. Surg. 2021, 406, 75–86. [Google Scholar] [CrossRef] [PubMed]
- Heinrich, S.; Sprinzl, M.; Schmidtmann, I.; Heil, E.; Koch, S.; Czauderna, C.; Heinrich, B.; Diggs, L.P.P.; Wörns, M.; Kloeckner, R.; et al. Validation of prognostic accuracy of MESH, HKLC, and BCLC classifications in a large German cohort of hepatocellular carcinoma patients. United Eur. Gastroenterol. J. 2020, 8, 444–452. [Google Scholar] [CrossRef] [Green Version]
- Gómez-Rodríguez, R.; Romero-Gutiérrez, M.; Artaza-Varasa, T.; González-Frutos, C.; Ciampi-Dopazo, J.J.; de-la-Cruz-Pérez, G.; Sánchez-Ruano, J.J. The value of the Barcelona Clinic Liver Cancer and alpha-fetoprotein in the prognosis of hepatocellular carcinoma. Rev. Esp. Enferm. Dig. 2012, 104, 298–304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reig, M.; Darnell, A.; Forner, A.; Rimola, J.; Ayuso, C.; Bruix, J. Systemic therapy for hepatocellular carcinoma: The issue of treatment stage migration and registration of progression using the BCLC-refined RECIST. Semin. Liver Dis. 2014, 34, 444–455. [Google Scholar] [CrossRef]
- Wehling, C.; Dill, M.T.; Olkus, A.; Springfeld, C.; Chang, D.H.; Naumann, P.; Longerich, T.; Kratochwil, C.; Mehrabi, A.; Merle, U.; et al. Treatment stage migration and treatment sequences in patients with hepatocellular carcinoma: Drawbacks and opportunities. J. Cancer Res. Clin. Oncol. 2021. [Google Scholar] [CrossRef]
- Marrero, J.A.; Kulik, L.M.; Sirlin, C.B.; Zhu, A.X.; Finn, R.S.; Abecassis, M.M.; Roberts, L.R.; Heimbach, J.K. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2018, 68, 723–750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vitale, A.; Trevisani, F.; Farinati, F.; Cillo, U. Treatment of Hepatocellular Carcinoma in the Precision Medicine Era: From Treatment Stage Migration to Therapeutic Hierarchy. Hepatology 2020, 72, 2206–2218. [Google Scholar] [CrossRef]
- Omata, M.; Cheng, A.L.; Kokudo, N.; Kudo, M.; Lee, J.M.; Jia, J.; Tateishi, R.; Han, K.-H.; Chawala, Y.K.; Shiina, S.; et al. Asia-Pacific clinical practice guidelines on the management of hepatocellular carcinoma: A 2017 update. Hepatol. Int. 2017, 11, 317–370. [Google Scholar] [PubMed] [Green Version]
- Raccomandazioni Multisocietarie Italiane (AISF, AIOM, IT-IHPBA, SIC, SIRM, SITO) per la Gestione Clinica Integrata del Paziente con Epatocarcinoma. Available online: https://www.webaisf.org/aisf-guidelines-e-position-papers/page/3/ (accessed on 1 December 2020).
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69. [Google Scholar] [CrossRef] [Green Version]
- Kutlu, O.C.; Chan, J.A.; Aloia, T.A.; Chun, Y.S.; Kaseb, A.O.; Passot, G.; Yamashita, S.; Vauthey, J.N.; Conrad, C. Comparative effectiveness of first-line radiofrequency ablation versus surgical resection and transplantation for patients with early hepatocellular carcinoma. Cancer 2017, 123, 1817–1827. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gil, E.; Kim, J.M.; Jeon, K.; Park, H.; Danbee, K.; Cho, J.; Suh, G.Y.; Park, J. Recipient Age and Mortality After Liver Transplantation: A Population-based Cohort Study. Transplantation 2018, 102, 2025–2032. [Google Scholar] [CrossRef] [PubMed]
- Sharpton, S.R.; Feng, S.; Hameed, B.; Yao, F.; Lai, J.C. Combined effects of recipient age and model for end-stage liver disease score on liver transplantation outcomes. Transplantation 2014, 98, 557–562. [Google Scholar] [CrossRef] [Green Version]
- Wilson, G.C.; Quillin, R.C.; Wima, K.; Sutton, J.M.; Hoehn, R.S.; Hanseman, D.J.; Paquette, I.M.; Paterno, F.; Woodle, E.S.; Abbott, D.E.; et al. Is liver transplantation safe and effective in elderly (≥70 years) recipients? A case-controlled analysis. HPB 2014, 16, 1088–1094. [Google Scholar] [CrossRef] [Green Version]
- Chu, K.K.W.; Chok, K.S.H. Is the treatment outcome of hepatocellular carcinoma inferior in elderly patients? World J. Gastroenterol. 2019, 25, 3563–3571. [Google Scholar] [CrossRef]
- Cescon, M.; Colecchia, A.; Cucchetti, A.; Peri, E.; Montrone, L.; Ercolani, G.; Festi, D.; Pinna, A.D. Value of transient elastography measured with FibroScan in predicting the outcome of hepatic resection for hepatocellular carcinoma. Ann. Surg. 2012, 256, 706–713. [Google Scholar] [CrossRef]
- Imamura, H.; Seyama, Y.; Kokudo, N.; Maema, A.; Sugawara, A.; Sano, K.; Takayama, T.; Makuuchi, M. One Thousand Fifty-Six Hepatectomies without Mortality in 8 Years. Arch. Surg. 2003, 138, 1198–1206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Gasperi, A.; Mazza, E.; Prosperi, M. Indocyanine green kinetics to assess liver function: Ready for a clinical dynamic assessment in major liver surgery? World J. Hepatol. 2016, 8, 355–367. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, A.; Koike, K.; Nishino, H. Clinical features and prognosis of elderly patients with hepatocellular carcinoma not indicated for surgical resection. Geriatr. Gerontol. Int. 2017, 17, 189–201. [Google Scholar] [CrossRef] [PubMed]
- Miki, D.; Aikata, H.; Uka, K.; Saneto, H.; Kawaoka, T.; Azakami, T.; Takaki, S.; Jeong, S.C.; Imamura, M.; Kawakami, Y.; et al. Clinicopathological features of elderly patients with hepatitis C virus-related hepatocellular carcinoma. J. Gastroenterol. 2008, 43, 550–557. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, H.; Kimura, T.; Kita, R.; Osaki, Y. Treatment for hepatocellular carcinoma in elderly patients: A literature review. J. Cancer 2013, 4, 635–643. [Google Scholar] [CrossRef] [Green Version]
- Shirabe, K.; Kajiyama, K.; Harimoto, N.; Gion, T.; Tsujita, E.; Abe, T.; Wakiyama, S.; Nagaie, T.; Maehara, Y. Early outcome following hepatic resection in patients older than 80 years of age. World J. Surg. 2009, 33, 1927–1932. [Google Scholar] [CrossRef] [PubMed]
- Randall, H.B.; Cao, S.; de Vera, M.E. Transplantation in elderly patients. Arch. Surg. 2003, 138, 1089–1092. [Google Scholar] [CrossRef] [Green Version]
- Orcutt, S.T.; Artinyan, A.; Li, L.T.; Silberfein, E.J.; Berger, D.H.; Albo, D.; Anaya, D.A. Postoperative mortality and need for transitional care following liver resection for metastatic disease in elderly patients: A population-level analysis of 4026 patients. HPB 2012, 14, 863–870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hutchins, L.F.; Unger, J.M.; Crowley, J.J.; Coltman, C.A.; Albain, K.S. Underrepresentation of patients 65 years of age or older in cancer-treatment trials. N. Engl. J. Med. 1999, 341, 2061–2067. [Google Scholar] [CrossRef] [PubMed]
- Oishi, K.; Itamoto, T.; Kohashi, T.; Matsugu, Y.; Nakahara, H.; Kitamoto, M. Safety of hepatectomy for elderly patients with hepatocellular carcinoma. World J. Gastroenterol. 2014, 20, 15028–15036. [Google Scholar] [CrossRef] [PubMed]
- Phan, K.; An, V.V.G.; Ha, H.; Phan, S.; Lam, V.; Pleass, H. Hepatic resection for malignant liver tumours in the elderly: A systematic review and meta-analysis. ANZ J. Surg. 2015, 85, 815–822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De La Fuente, S.G.; Bennett, K.M.; Scarborough, J.E. Functional status determines postoperative outcomes in elderly patients undergoing hepatic resections. J. Surg. Oncol. 2013, 107, 865–870. [Google Scholar] [CrossRef]
- Cieslak, K.P.; Baur, O.; Verheij, J.; Bennink, R.J.; van Gulik, T.M. Liver function declines with increased age. HPB 2016, 18, 691–696. [Google Scholar] [CrossRef] [Green Version]
- Tufo, A.; Dunne, D.F.; Manu, N.; Lacasia, C.; Jones, L.; de Liguori Carino, N.; Malik, A.Z.; Poston, G.J.; Fenwick, S.W. Changing outlook for colorectal liver metastasis resection in the elderly. Eur. J. Surg. Oncol. 2019, 45, 635–643. [Google Scholar] [CrossRef] [PubMed]
- Tufo, A.; Dunne, D.F.J.; Manu, N.; Joshi, H.; Lacasia, C.; Jones, L.; Malik, H.Z.; Poston, G.J.; Fenwick, S.W. Hepatectomy for octogenarians with colorectal liver metastasis in the era of enhanced recovery. Eur. J. Surg. Oncol. 2018, 44, 1040–1047. [Google Scholar] [CrossRef]
- Okamura, Y.; Sugiura, T.; Ito, T.; Yamamoto, Y.; Ashida, R.; Uesaka, K. The Short- and Long-Term Outcomes in Elderly Patients with Hepatocellular Carcinoma after Curative Surgery: A Case-Controlled Study with Propensity Score Matching. Eur. Surg. Res. 2019, 59, 380–390. [Google Scholar] [CrossRef]
- Cho, E.; Cho, H.A.; Jun, C.H.; Kim, H.J.; Cho, S.B.; Choi, S.K. A review of hepatocellular carcinoma in elderly patients focused on management and outcomes. Vivo 2019, 33, 1411–1420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reddy, S.K.; Barbas, A.S.; Turley, R.S.; Gamblin, T.C.; Geller, D.A.; Marsh, J.W.; Tsung, A.; Clary, B.M.; Lagoo-Deenadayalan, S. Major liver resection in elderly patients: A multi-institutional analysis. J. Am. Coll. Surg. 2011, 212, 787–795. [Google Scholar] [CrossRef] [PubMed]
- Song, W.; Wang, K.; Zhang, R.; Dai, Q.; Zou, S. The enhanced recovery after surgery (ERAS) program in liver surgery: A meta-analysis of randomized controlled trials. SpringerPlus 2016, 5, 207. [Google Scholar] [CrossRef] [Green Version]
- Wakabayashi, G.; Cherqui, D.; Geller, D.A.; Buell, J.F.; Kaneko, H.; Han, H.S.; Asbun, O.; O’Rourche, N.; Tanabe, M.; Koffron, A.J.; et al. Recommendations for laparoscopic liver resection: A report from the second international consensus conference held in Morioka. Ann. Surg. 2015, 261, 619–629. [Google Scholar] [CrossRef] [PubMed]
- Hilal, M.A.; Aldrighetti, L.; Dagher, I.; Edwin, B.; Troisi, R.I.; Alikhanov, R.; Aroori, S.; Belli, G.; Besselink, M.; Briceno, J.; et al. The Southampton Consensus Guidelines for Laparoscopic Liver Surgery: From Indication to Implementation. Ann. Surg. 2018, 268, 11–18. [Google Scholar] [CrossRef] [Green Version]
- Cheek, S.M.; Sucandy, I.; Tsung, A.; Marsh, J.W.; Geller, D.A. Evidence supporting laparoscopic major hepatectomy. J. Hepato-Biliary-Pancreatic Sci. 2016, 23, 257–259. [Google Scholar] [CrossRef] [Green Version]
- Morise, Z.; Ciria, R.; Cherqui, D.; Chen, K.H.; Belli, G.; Wakabayashi, G. Can we expand the indications for laparoscopic liver resection? A systematic review and meta-analysis of laparoscopic liver resection for patients with hepatocellular carcinoma and chronic liver disease. J. Hepato-Biliary-Pancreatic Sci. 2015, 22, 342–352. [Google Scholar] [CrossRef] [PubMed]
- Sposito, C.; Battiston, C.; Facciorusso, A.; Mazzola, M.; Muscarà, C.; Scotti, M.; Romito, R.; Mariani, L.; Mazzafferro, V. Propensity score analysis of outcomes following laparoscopic or open liver resection for hepatocellular carcinoma. Br. J. Surg 2016, 103, 871–880. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Huang, Z.; Guo, B.; Liu, S.; Xiao, W.; Liang, J. Short- and long-term outcomes of laparoscopic hepatectomy in elderly patients with hepatocellular carcinoma. J. BUON 2018, 23, 971–978. [Google Scholar]
- Dumronggittigule, W.; Han, H.S.; Ahn, S.; Yoon, Y.S.; Cho, J.Y.; Choi, Y.R. Laparoscopic versus Open Hepatectomy for Hepatocellular Carcinoma in Elderly Patients: A Single-Institutional Propensity Score Matching Comparison. Dig. Surg. 2020, 37, 495–504. [Google Scholar] [CrossRef]
- Nomi, T.; Hirokawa, F.; Kaibori, M.; Ueno, M.; Tanaka, S.; Hokuto, D.; Noda, T.; Nakai, T.; Ikoma, H.; Iida, H.; et al. Laparoscopic versus open liver resection for hepatocellular carcinoma in elderly patients: A multi-centre propensity score-based analysis. Surg. Endosc. 2020, 34, 658–666. [Google Scholar] [CrossRef] [PubMed]
- Sato, S.; Tanaka, K.; Nojiri, K.; Kumamoto, T.; Mori, R.; Taniguchi, K.; Matsuyama, R.; Takeda, K.; Ueda, M.; Akiyama, H.; et al. Hepatic Resection for Hepatocellular Carcinoma in the Elderly: Selecting Hepatectomy Procedures Based on Patient Age. Anticancer Res. 2015, 35, 6855–6860. [Google Scholar] [PubMed]
- Famularo, S.; Di Sandro, S.; Giani, A.; Angrisani, M.; Lauterio, A.; Romano, F.; Gianotti, L.; De Carlis, L. The impact of age and ageing on hepatocarcinoma surgery: Short- and long-term outcomes in a multicentre propensity-matched cohort. Liver Int. 2019, 39, 894–904. [Google Scholar] [CrossRef] [PubMed]
- Hirokawa, F.; Hayashi, M.; Miyamoto, Y.; Asakuma, M.; Shimizu, T.; Komeda, K.; Inoue, Y.; Takeshita, A.; Shibayama, Y.; Uchiyama, K. Surgical Outcomes and Clinical Characteristics of Elderly Patients Undergoing Curative Hepatectomy for Hepatocellular Carcinoma. J. Gastrointest. Surg. 2013, 17, 1929–1937. [Google Scholar] [CrossRef] [PubMed]
- Dajti, E.; Ravaioli, F.; Festi, D.; Colecchia, A. Clinical outcomes after treatment with di-rect-acting antivirals: Not all concern hepatocellular carcinoma risk. Hepatobiliary Surg. Nutr. 2020, 9, 505–507. [Google Scholar] [CrossRef] [PubMed]
- Ravaioli, F.; Conti, F.; Brillanti, S.; Andreone, P.; Mazzella, G.; Buonfiglioli, F.; Serio, I.; Verrucchi, G.; Reggiani, M.L.B.; Colli, A.; et al. Hepatocellular carcinoma risk assessment by the measurement of liver stiffness variations in HCV cirrhotics treated with direct acting antivirals. Dig. Liver Dis. 2018, 50, 573–579. [Google Scholar] [CrossRef] [PubMed]
- Marasco, G.; Colecchia, A.; Colli, A.; Ravaioli, F.; Casazza, G.; Reggiani, M.L.B.; Cucchetti, A.; Cescon, M.; Festi, D. Role of liver and spleen stiffness in predicting the recurrence of hepatocellular carcinoma after resection. J. Hepatol. 2019, 70, 440–448. [Google Scholar] [CrossRef]
- Itamoto, T.; Nakahara, H.; Amano, H.; Kohashi, T.; Ohdan, H.; Tashiro, H.; Asahara, T. Repeat hepatectomy for recurrent hepatocellular carcinoma. Surgery 2007, 141, 589–597. [Google Scholar] [CrossRef]
- Zhu, G.Q.; Sun, M.; Liao, W.T.; Yu, W.; Zhou, S.; Zhou, Z.; Shi, T.; Fan, J.; Zhou, J.; Qiu, L.; et al. Comparative efficacy and safety between ablative therapies or surgery for small hepatocellular carcinoma: A network meta-analysis. Expert Rev. Gastroenterol. Hepatol. 2018, 12, 935–945. [Google Scholar] [CrossRef] [PubMed]
- Yu, B.; Ding, Y.; Liao, X.; Wang, C.; Wang, B.; Chen, X. Radiofrequency ablation versus surgical resection in elderly patients with early-stage hepatocellular carcinoma in the era of organ shortage. Saudi J. Gastroenterol. 2018, 24, 317–325. [Google Scholar] [CrossRef]
- Kaibori, M.; Yoshii, K.; Hasegawa, K.; Ogawa, A.; Kubo, S.; Tateishi, R.; Izumi, N.; Kadoya, M.; Kudo, M.; Kumada, T.; et al. Treatment Optimization for Hepatocellular Carcinoma in Elderly Patients in a Japanese Nationwide Cohort. Ann. Surg. 2019, 270, 121–130. [Google Scholar] [CrossRef]
- Cucchetti, A.; Piscaglia, F.; Cescon, M.; Colecchia, A.; Bolondi, L.; Pinna, A.D. 265 Cost-effectiveness of hepatic resection versus percutaneous ablation for hepatocellular carcinoma within the Milan criteria. J. Hepatol. 2013, 58, S63–S227. [Google Scholar] [CrossRef]
- Jiang, Y.Q.; Wang, Z.X.; Deng, Y.N.; Yang, Y.; Wang, G.Y.; Chen, G.H. Efficacy of hepatic resection vs. radiofrequency ablation for patients with very-early-stage or early-stage hepatocellular carcinoma: A population-based study with stratification by age and tumor size. Front. Oncol. 2019, 9, 113. [Google Scholar] [CrossRef]
- Sala, M.; Fuster, J.; Llovet, J.M.; Navasa, M.; Solè, M.; Varela, M.; Pons, F.; Rimola, A.; Garcia-Valdecasas, J.C.; Brú, C.; et al. High pathological risk of recurrence after surgical resection for hepatocellular carcinoma: An indication for salvage liver transplantation. Liver Transpl. 2004, 10, 1294–1300. [Google Scholar] [CrossRef]
- Cho, S.W.; Steel, J.; Tsung, A.; Marsh, J.W.; Geller, D.A.; Gamblin, T.C. Safety of liver resection in the elderly: How important is age? Ann. Surg. Oncol. 2011, 18, 1088–1095. [Google Scholar] [CrossRef]
- Fujiwara, N.; Tateishi, R.; Kondo, M.; Minami, T.; Mikami, S.; Sato, M.; Uchino, K.; Enooku, K.; Masuzaki, R.; Nakagawa, H.; et al. Cause-specific mortality associated with aging in patients with hepatocellular carcinoma undergoing percutaneous radiofrequency ablation. Eur. J. Gastroenterol. Hepatol. 2014, 26, 1039–1046. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, H.; Osaki, Y.; Iguchi, E.; Takeda, H.; Ohara, Y.; Sakamoto, A.; Hatamaru, K.; Henmi, S.; Saito, S.; Nasu, A.; et al. Percutaneous radiofrequency ablation for hepatocellular carcinoma: Clinical outcome and safety in elderly patients. J. Gastrointest. Liver Dis. 2012, 21, 397–405. [Google Scholar]
- Huang, J.; Yan, L.; Cheng, Z.; Wu, H.; Du, L.; Wang, J.; Xu, J.; Zeng, Y. A randomized trial comparing radiofrequency ablation and surgical resection for HCC conforming to the Milan criteria. Ann. Surg. 2010, 252, 903–912. [Google Scholar] [CrossRef]
- Lee, Y.H.; Hsu, C.Y.; Chu, C.W.; Liu, P.H.; Hsia, C.Y.; Huang, Y.H.; Su, C.W.; Chiou, Y.Y.; Lin, H.C.; Huo, T.L. Radiofrequency ablation is better than surgical resection in patients with hepatocellular carcinoma within the Milan criteria and preserved liver function: A retrospective study using propensity score analyses. J. Clin. Gastroenterol. 2015, 49, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.A.; Shim, J.H.; Kim, M.J.; Kim, S.Y.; Won, H.J.; Shin, Y.M.; Kim, P.N.; Kim, K.H.; Lee, S.G.; Lee, H.C. Radiofrequency ablation as an alternative to hepatic resection for single small hepatocellular carcinomas. Br. J. Surg. 2016, 103, 126–135. [Google Scholar] [CrossRef]
- Miura, J.T.; Johnston, F.M.; Tsai, S.; Eastwood, D.; Banejree, A.; Christians, K.K.; Turaga, K.K.; Gamblin, T.C. Surgical resection versus ablation for hepatocellular carcinoma ≤ 3 cm: A population-based analysis. HPB 2015, 17, 896–901. [Google Scholar] [CrossRef] [Green Version]
- Ng, K.K.; Poon, R.T. Radiofrequency ablation for malignant liver tumor. Surg. Oncol. 2005, 14, 41–52. [Google Scholar] [CrossRef] [PubMed]
- Tan, H.Y.; Gong, J.F.; Yu, F.; Tang, W.H.; Yang, K. Long-Term Efficacy of Laparoscopic Radiofrequency Ablation in Early Hepatocellular Carcinoma: A Systematic Review and Meta-Analysis. J. Laparoendosc. Adv. Surg. Tech. 2019, 29, 770–779. [Google Scholar] [CrossRef] [PubMed]
- Han, J.; Fan, Y.C.; Wang, K. Radiofrequency ablation versus microwave ablation for early stage hepatocellular carcinoma: A PRISMA-compliant systematic review and meta-analysis. Medicine 2020, 99, e22703. [Google Scholar] [CrossRef] [PubMed]
- Cavagnaro, M.; Amabile, C.; Cassarino, S.; Tosoratti, N.; Pinto, R.; Lopresto, V. Influence of the target tissue size on the shape of ex vivo microwave ablation zones. Int. J. Hyperth. 2015, 31, 48–57. [Google Scholar] [CrossRef]
- Liang, P.; Yu, J.; Lu, M.D.; Dong, B.W.; Yu, X.L.; Zhou, X.D.; Hu, B.; Xie, M.X.; Cheng, W.; He, W.; et al. Practice guidelines for ultrasound-guided percutaneous microwave ablation for hepatic malignancy. World J. Gastroenterol. 2013, 19, 5430–5438. [Google Scholar] [CrossRef]
- Yu, J.; Yu, X.L.; Han, Z.Y.; Cheng, Z.G.; Liu, F.Y.; Zhai, H.Y.; Mu, M.J.; Liu, Y.M.; Liang, P. Percutaneous cooled-probe microwave versus radiofrequency ablation in early-stage hepatocellular carcinoma: A phase III randomised controlled trial. Gut 2017, 66, 1172–1173. [Google Scholar] [CrossRef] [Green Version]
- Liang, P.; Wang, Y.; Yu, X.L.; Dong, B. Malignant liver tumors: Treatment with percutaneous microwave ablation—Complications among cohort of 1136 patients. Radiology 2009, 251, 933–940. [Google Scholar] [CrossRef]
- Liang, P.; Yu, J.; Yu, X.L.; Wang, X.H.; Wei, Q.; Yu, S.Y.; Li, H.X.; Sun, H.T.; Zhang, Z.Y.; Liu, H.C.; et al. Percutaneous cooled-tip microwave ablation under ultrasound guidance for primary liver cancer: A multicentre analysis of 1363 treatment-naive lesions in 1007 patients in China. Gut 2012, 61, 1100–1101. [Google Scholar] [CrossRef]
- Facciorusso, A.; Di Maso, M.; Muscatiello, N. Microwave ablation versus radiofrequency ablation for the treatment of hepatocellular carcinoma: A systematic review and meta-analysis. Int. J. Hyperth. 2016, 32, 339–344. [Google Scholar] [CrossRef]
- Shen, X.; Ma, S.; Tang, X.; Wang, T.; Qi, X.; Chi, J.; Wang, Z.; Cui, D.; Zhang, Y.; Li, P.; et al. Clinical outcome in elderly Chinese patients with primary hepatocellular carcinoma treated with percutaneous microwave coagulation therapy (PMCT): A Strobe-compliant observational study. Medicine 2018, 97, e11618. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Cheng, Z.; Yu, J.; Li, K.; Hao, G.; Liu, F.; Han, Z.; Yu, X.; Liang, P. US-guided percutaneous microwave ablation for early-stage hepatocellular carcinoma in elderly patients is as effective as in younger patients: A 10-year experience. J. Cancer Res. Ther. 2020, 16, 292–300. [Google Scholar] [CrossRef] [PubMed]
- Di Costanzo, G.G.; Tortora, R.; D’Adamo, G.; De Luca, M.; Lampasi, F.; Addario, L.; Lanza, A.G.; Picciotto, F.P.; Tartaglione, M.T.; Cordone, G.; et al. Radiofrequency ablation versus laser ablation for the treatment of small hepatocellular carcinoma in cirrhosis: A randomized trial. J. Gastroenterol. Hepatol. 2015, 30, 559–565. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Wang, H.; Yang, W.; Hu, K.; Xie, H.; Hu, K.Q.; Bai, W.; Dong, Z.; Lu, Y.; Zeng, Z.; et al. Multicenter randomized controlled trial of percutaneous cryoablation versus radiofrequency ablation in hepatocellular carcinoma. Hepatology 2015, 61, 1579–1590. [Google Scholar] [CrossRef] [PubMed]
- Cheng, R.G.; Bhattacharya, R.; Yeh, M.M.; Padia, S.A. Irreversible electroporation can effectively ablate hepatocellular carcinoma to complete pathologic necrosis. J. Vasc. Interv. Radiol. 2015, 26, 1184–1188. [Google Scholar] [CrossRef] [PubMed]
- NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) Hepatobiliary Cancers Version 5. 2020. Available online: https://www.nccn.org. (accessed on 4 August 2020).
- Cheng, A.L.; Amarapurkar, D.; Chao, Y.; Chen, P.J.; Geschwind, J.F.; Goh, K.L.; Han, K.H.; Kudo, M.; Lee, H.C.; Lee, R.C.; et al. Re-evaluatingntransarterial chemoembolization for the treatment of hepatocellular carcinoma: Consensus recommendations and review by an International Expert Panel. Liver Int. 2014, 34, 174–183. [Google Scholar] [CrossRef] [PubMed]
- Bolondi, L.; Burroughs, A.; Dufour, J.F.; Galle, P.R.; Mazzaferro, V.; Piscaglia, F.; Raoul, J.L.; Sangro, B. Heterogeneity of patients with intermediate (BCLC B) Hepatocellular Carcinoma: Proposal for a subclassification to facilitate treatment decisions. Semin. Liver Dis. 2012, 32, 348–359. [Google Scholar] [CrossRef]
- Kudo, M.; Arizumi, T.; Ueshima, K.; Sakurai, T.; Kitano, M.; Nishida, N. Subclassification of BCLC B stage hepatocellular carcinoma and treatment strategies: Proposal of modified Bolondi’s subclassification (Kinki criteria). Dig. Dis. 2015, 33, 751–758. [Google Scholar] [CrossRef]
- Kudo, M. Heterogeneity and subclassification of Barcelona Clinic Liver Cancer Stage B. Liver Cancer 2016, 5, 91–96. [Google Scholar] [CrossRef]
- Raoul, J.L.; Sangro, B.; Forner, A.; Mazzaferro, V.; Piscaglia, F.; Bolondi, L.; Lencioni, R. Evolving strategies for the management of intermediate-stage hepatocellular carcinoma: Available evidence and expert opinion on the use of transarterial chemoembolization. Cancer Treat. Rev. 2011, 37, 212–220. [Google Scholar] [CrossRef] [PubMed]
- Kadalayil, L.; Benini, R.; Pallan, L.; O’Bernie, J.; Marelli, L.; Yu, D.; Hackshaw, A.; Fox, R.; Johnson, P.; Burrough, A.K.; et al. A simple prognostic scoring system for patients receiving transarterial embolization for hepatocellular cancer. Ann. Oncol. 2013, 24, 2565–2570. [Google Scholar] [CrossRef] [PubMed]
- Mondazzi, L.; Bottelli, R.; Brambilla, G.; Rampoldi, A.; Rezakovic, I.; Zavaglia, C.; Alberti, A.; Idèo, G. Transarterial oily chemoembolization for the treatment of hepatocellular carcinoma: A multivariate analysis of prognostic factors. Hepatology 1994, 19, 1115–1123. [Google Scholar] [CrossRef] [PubMed]
- Yau, T.; Yao, T.J.; Chan, P.; Epstein, R.J.; Ng, K.K.; Chok, S.H.; Cheung, T.T.; Fan, S.T.; Poon, R.T. The outcomes of elderly patients with hepatocellular carcinoma treated with transarterial chemoembolization. Cancer 2009, 115, 5507–5515. [Google Scholar] [CrossRef]
- Cheng, H.M.; Tanaka, T.; Nishiofuku, H.; Chanoki, Y.; Horiuchi, K.; Masada, T.; Tatsumoto, S.; Matsumoto, T.; Marugami, N.; Kichikawa, K. Safety and Prognosis of Transarterial Chemoembolization for Octogenarians with Hepatocellular Carcinoma. Cardiovasc. Interv. Radiol. 2019, 42, 1413–1419. [Google Scholar] [CrossRef]
- Cohen, M.J.; Levy, I.; Barak, O.; Bloom, A.I.; Fernandez-Ruiz, M.; Di Maio, M.; Perrone, F.; Poon, R.T.; Shouval, D.; Yau, T.; et al. Transarterial chemo-embolization is safe and effective for elderly advanced hepatocellular carcinoma patients: Results from an international database. Liver Int. 2014, 34, 1109–1117. [Google Scholar] [CrossRef]
- Liu, P.H.; Hsu, C.Y.; Lee, Y.H.; Hsia, C.Y.; Huang, Y.H.; Su, C.W.; Chiou, Y.Y.; Lin, H.C.; Huo, T.I. Uncompromised treatment efficacy in elderly patients with hepatocellular carcinoma: A propensity score analysis. Medicine 2014, 93, e264. [Google Scholar] [CrossRef] [PubMed]
- Aizumi, T.; Ueshima, K.; Minami, T.; Kono, M.; Chishina, H.; Takita, M.; Kitai, S.; Inoue, T.; Yada, N.; Hagiwara, S.; et al. Effectiveness of Sorafenib in Patients with Transcatheter Arterial Chemoembolization (TACE) Refractory and Intermediate-Stage Hepatocellular Carcinoma. Liver Cancer 2015, 4, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Ogasawara, S.; Chiba, T.; Ooka, Y.; Kanogawa, N.; Motoyama, T.; Suzuki, E.; Tawada, A.; Kanai, F.; Yoshikawa, M.; Yokosuka, O. Efficacy of sorafenib in intermediate-stage hepatocellular carcinoma patients refractory to transarterial chemoembolization. Oncology 2014, 87, 330–341. [Google Scholar] [CrossRef]
- Llover, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.; de Olivera, A.C.; Santoro, A.; Raoul, J.; Forner, A.; et al. Sorafenib in Advanced Hepatocellular Carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef]
- Cheng, A.L.; Kang, Y.K.; Chen, Z.; Tsao, C.J.; Qin, S.; Kim, J.S.; Luo, R.; Feng, J.; Ye, S.; Yang, T.S.; et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: A phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2009, 10, 25–34. [Google Scholar] [CrossRef]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J.W.; Han, G.; Jassem, J.; et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: A randomised phase 3 non-inferiority trial. Lancet 2018, 391, 1163–1173. [Google Scholar] [CrossRef] [Green Version]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef]
- Bruix, J.; Qin, S.; Merle, P.; Granito, A.; Huang, Y.H.; Bodoky, G.; Pracht, M.; Yokosuka, O.; Rosmorduc, O.; Breder, V.; et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017, 389, 56–66. [Google Scholar] [CrossRef] [Green Version]
- Abou-Alfa, G.K.; Meyer, T.; Cheng, A.L.; El-Khoueiry, A.B.; Rimassa, L.; Ryoo, B.Y.; Cicin, I.; Merle, P.; Chen, Y.; Park, J.W.; et al. Cabozantinib in Patients with Advanced and Progressing Hepatocellular Carcinoma. N. Engl. J. Med. 2015, 379, 54–63. [Google Scholar] [CrossRef]
- Zhu, A.; Park, J.O.; Ryoo, B.Y.; Yen, C.J.; Poon, R.; Pastorelli, D.; Blanc, J.; Chumg, H.C.; Baron, A.D.; Pfiffer, T.E.F.; et al. Ramucirumab versus placebo as second-line treatment in patients with advanced hepatocellular carcinoma following first-line therapy with sorafenib (REACH): A randomised, double-blind, multicentre, phase 3 trial. Lancet Oncol. 2015, 16, 859–870. [Google Scholar] [CrossRef]
- Zhu, A.X.; Kang, Y.K.; Yen, C.J.; Finn, R.S.; Galle, P.R.; Llovet, J.M.; Assenat, E.; Brandi, G.; Pracht, M.; Lim, H.Y.; et al. Ramucirumab after sorafenib in patients with advanced hepatocellular carcinoma and increased α-fetoprotein concentrations (REACH-2): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019, 20, 282–296. [Google Scholar] [CrossRef]
- Lang, L. FDA approves sorafenib for patients with inoperable liver cancer. Gastroenterology 2008, 134, 379. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency. Summary of Product Characteristics. Available online: https://www.ema.europa.eu/en/documents/product-information/nexavar-epar-product-information_en.pdf (accessed on 5 March 2021).
- Wilhelm, S.M.; Carter, C.; Tang, L.; Wilkie, D.; McNabola, A.; Rong, H.; Chen, C.; Zhang, X.; Vincent, P.; McHugh, M.; et al. BAY 43-9006 exhibits broad spectrum oral antitumor activity and targets the RAF/MEK/ERK pathway and receptor tyrosine kinases involved in tumor progression and angiogenesis. Cancer Res. 2004, 64, 7099–7109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Medicines Agency. Nexavar Epar Scientific Discussion. Available online: https://www.ema.europa.eu/en/documents/scientific-discussion/nexavar-epar-scientific-discussion_en.pdf (accessed on 5 March 2021).
- Li, Y.; Gao, Z.H.; Qu, X.J. The adverse effects of sorafenib in patients with advanced cancers. Basic Clin. Pharmacol. Toxicol. 2015, 116, 216–221. [Google Scholar] [CrossRef] [PubMed]
- Bruix, J.; Cheng, A.L.; Meinhardt, G.; Nakajima, K.; De Sanctis, Y.; Llovet, J. Prognostic factors and predictors of sorafenib benefit in patients with hepatocellular carcinoma: Analysis of two phase III studies. J. Hepatol. 2017, 67, 999–1008. [Google Scholar] [CrossRef] [Green Version]
- Hajiev, S.; Allara, E.; Motedayen-Aval, L.; Arizumi, T.; Bettinger, D.; Pirisi, M.; Rimassa, L.; Pressiani, T.; Personeni, N.; Giordano, L.; et al. Impact of age on sorafenib outcomes in hepatocellular carcinoma: An international cohort study. Br. J. Cancer 2020. [Google Scholar] [CrossRef]
- Reiss, K.A.; Yu, S.; Mamtani, R.; Mehta, R.; D’Addeo, K.; Wileyto, E.P.; Taddei, T.H.; Kaplan, D.E. Starting dose of sorafenib for the treatment of hepatocellular carcinoma: A retrospective, multi-institutional study. J. Clin. Oncol. 2017, 35, 3575–3581. [Google Scholar] [CrossRef]
- Cabanillas, M.E.; Habra, M.A. Lenvatinib: Role in thyroid cancer and other solid tumors. Cancer Treat. Rev. 2016, 42, 47–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hussein, Z.; Mizuo, H.; Hayato, S.; Namiki, M.; Shumaker, R. Clinical Pharmacokinetic and Pharmacodynamic Profile of Lenvatinib, an Orally Active, Small-Molecule, Multitargeted Tyrosine Kinase Inhibitor. Eur. J. Drug Metab. Pharmacokinet. 2017, 42, 903–914. [Google Scholar] [CrossRef]
- Tada, T.; Kumada, T.; Hiraoka, A.; Michitaka, K.; Atsukawa, M.; Hirooka, M.; Takaguchi, K.; Kariyama, K.; Itobayashi, E.; Tajiri, K.; et al. Safety and efficacy of lenvatinib in elderly patients with unresectable hepatocellular carcinoma: A multicenter analysis with propensity score matching. Hepatol. Res. 2020, 50, 75–83. [Google Scholar] [CrossRef] [Green Version]
- Li, D.; Toh, H.C.; Merle, P.; Tsuchiya, K.; Hernandez, S.; Shao, H.; Mulla, S.; Ding, B.; Kudo, M. Atezolizumab + Bevacizumab vs. Sorafenib for Unresectable Hepatocellular Carcinoma (HCC): Results from Older Adults Enrolled in IMbrave150, Abstract O-8. In Proceedings of the ESMO World Congress on Gastrointestinal Cancer 2020, Online, 1–4 July 2020. [Google Scholar]
- U.S. Food and Drug. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/regorafenib (accessed on 1 December 2020).
- U.S. Food and Drug. Available online: https://www.fda.gov/drugs/fda-approves-cabozantinib-hepatocellular-carcinoma (accessed on 1 December 2020).
- U.S. Food and Drug. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-ramucirumab-hepatocellular-carcinoma (accessed on 1 December 2020).
- U.S. Food and Drug. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-grants-accelerated-approval-nivolumab-hcc-previously-treated-sorafenib (accessed on 1 December 2020).
- U.S. Food and Drug. Available online: https://www.fda.gov/drugs/fda-grants-accelerated-approval-pembrolizumab-hepatocellular-carcinoma (accessed on 1 December 2020).
- European Medicines Agency. Available online: https://www.ema.europa.eu/en/documents/variation-report/stivarga-h-c-2573-ii-0020-epar-assessment-report-variation_en.pdf (accessed on 1 December 2020).
- European Medicines Agency. Available online: https://www.ema.europa.eu/en/documents/variation-report/cabometyx-h-c-004163-ii-0005-epar-assessment-report-variation_en.pdf (accessed on 1 December 2020).
- European Medicines Agency. Available online: https://www.ema.europa.eu/en/documents/smop/chmppost-authorisation-summary-positive-opinion-cyramza-ii-27_en.pdf (accessed on 1 December 2020).
- Wilhelm, S.M.; Dumas, J.; Adnane, L.; Lynch, M.; Carter, C.A.; Shutz, G.; Thierauch, H.; Zopf, D. Regorafenib (BAY 73-4506): A new oral multikinase inhibitor of angiogenic, stromal and oncogenic receptor tyrosine kinases with potent preclinical antitumor activity. Int. J. Cancer 2011, 129, 245–255. [Google Scholar] [CrossRef] [PubMed]
- Gerisch, M.; Hafner, F.T.; Lang, D.; Radtke, M.; Diefenbach, K.; Cleton, A.; Lettieri, J. Mass balance, metabolic disposition, and pharmacokinetics of a single oral dose of regorafenib in healthy human subjects. Cancer Chemother. Pharmacol. 2018, 81, 195–206. [Google Scholar] [CrossRef] [Green Version]
- Keunecke, A.; Hoefman, S.; Drenth, H.J.; Zisowsky, J.; Cleton, A.; Ploeger, B.A. Population pharmacokinetics of regorafenib in solid tumours: Exposure in clinical practice considering enterohepatic circulation and food intake. Br. J. Clin. Pharmacol. 2020, 86, 2362–2376. [Google Scholar] [CrossRef]
- Yakes, F.M.; Chen, J.; Tan, J.; Yamaguchi, K.; Shi, Y.; Yu, P.; Qian, F.; Chu, F.; Bentzien, F.; Cancilla, B.; et al. Cabozantinib (XL184), a novel MET and VEGFR2 inhibitor, simultaneously suppresses metastasis, angiogenesis, and tumor growth. Mol. Cancer Ther. 2011, 10, 2298–2308. [Google Scholar] [CrossRef] [Green Version]
- Debaillon Vesque, A.; Decraecker, M.; Blanc, J.F. Profile of Cabozantinib for the Treatment of Hepatocellular Carcinoma: Patient Selection and Special Considerations. J. Hepatocell. Carcinoma 2020, 7, 91–99. [Google Scholar] [CrossRef]
- Kudo, M.; Galle, P.R.; Llovet, J.M.; Finn, R.S.; Vogel, A.; Motomura, K.; Assenat, E.; Merle, P.; Brandi, G.; Daniele, B.; et al. Ramucirumab in elderly patients with hepatocellular carcinoma and elevated alpha-fetoprotein after sorafenib in REACH and REACH-2. Liver Int. 2020, 40, 2008–2020. [Google Scholar] [CrossRef] [PubMed]
- El-Khoueiry, A.B.; Sangro, B.; Yau, T.; Crocenzi, T.S.; Kudo, M.; Hsu, C.; Kim, T.Y.; Choo, S.P.; Trojan, J.; Welling, T.H.; et al. Nivolumab in patients with advanced hepatocellular carcinoma (CheckMate 040): An open-label, non-comparative, phase 1/2 dose escalation and expansion trial. Lancet 2017, 389, 2492–2502. [Google Scholar] [CrossRef]
- Zhu, A.X.; Finn, R.S.; Edeline, J.; Cattan, S.; Ogasawara, S.; Palmer, D.; Verslype, C.; Zagonel, V.; Fartoux, L.; Vogel, A.; et al. KEYNOTE-224 investigators. Pembrolizumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib (KEYNOTE-224): A non-randomised, open-label phase 2 trial. Lancet Oncol. 2018, 19, 940–952. [Google Scholar] [CrossRef]
- Holt, P.R. Intestinal malabsorption in the elderly. Dig. Dis. 2007, 25, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Cabrera, M.A.; Dip, R.M.; Furlan, M.O.; Rodrigues, S.L. Use of drugs that act on the cytochrome P450 system in the elderly. Clinics 2009, 64, 273–278. [Google Scholar] [CrossRef] [Green Version]
- Yan, T.; Lu, L.; Xie, C.; Chen, T.; Peng, X.; Zhu, L.; Wang, L.; Li, Q.; Shi, J.; Zhou, F.; et al. Severely Impaired and Dysregulated Cytochrome P450 Expression and Activities in Hepatocellular Carcinoma: Implications for Personalized Treatment in Patients. Mol. Cancer Ther. 2015, 14, 2874–2886. [Google Scholar] [CrossRef] [Green Version]
- Klotz, U. Pharmacokinetics and drug metabolism in the elderly. Drug Metab. Rev. 2009, 41, 67–76. [Google Scholar] [CrossRef]
- Choi, W.M.; Lee, D.; Shim, J.H.; Kim, K.M.; Lim, Y.S.; Lee, H.C.; Yoo, C.; Park, S.R.; Ryu, M.H.; Ryoo, B.Y.; et al. Effectiveness and Safety of Nivolumab in Child—Pugh B Patients with Hepatocellular Carcinoma: A Real-World Cohort Study. Cancers 2020, 12, 1968. [Google Scholar] [CrossRef]
- Kim, Y.J.; Jang, B.K.; Kim, E.S.; Chung, W.J.; Park, K.S.; Cho, B.; Hwang, J.S. Hepatocellular carcinoma in the elderly: Clinical characteristics, treatment, survival analysis in Korean patients older than 70 years. J. Korean Med. Sci. 2012, 27, 1147–1154. [Google Scholar] [CrossRef] [PubMed]
- Tsukioka, G.; Kakizaki, S.; Sohara, N.; Sato, S.; Takagi, H.; Arai, H.; Abe, T.; Toyoda, M.; Katakai, K.; Kojima, A.; et al. Hepatocellular carcinoma in extremely elderly patients: An analysis of clinical characteristics, prognosis and patient survival. World J. Gastroenterol. 2006, 12, 48–53. [Google Scholar] [CrossRef] [Green Version]
- Dunne, R.F.; Loh, K.P.; Williams, G.R.; Jatoi, A.; Mustian, K.M.; Mohile, S.G. Cachexia and Sarcopenia in Older Adults with Cancer: A Comprehensive Review. Cancers 2019, 11, 1861. [Google Scholar] [CrossRef] [Green Version]
- Harimoto, N.; Yoshizumi, T.; Shimokawa, M.; Sakata, M.; Kimura, K.; Itoh, S.; Ikegami, T.; Ikeda, T.; Shirabe, K.; Maehara, Y. Sarcopenia is a poor prognostic factor following hepatic resection in patients aged 70 years and older with hepatocellular carcinoma. Hepatol. Res. 2016, 46, 1247–1255. [Google Scholar] [CrossRef]
- Antonelli, G.; Gigante, E.; Iavarone, M.; Begini, P.; Sangiovanni, A.; Iannicelli, E.; Biondetti, P.; Pellicelli, A.M.; Miglioresi, L.; Marchetti, P.; et al. Sarcopenia is associated with reduced survival in patients with advanced hepatocellular carcinoma undergoing sorafenib treatment. United Eur. Gastroenterol. J. 2018, 6, 1039–1048. [Google Scholar] [CrossRef] [PubMed]
- Amanuma, M.; Nagai, H.; Igarashi, Y. Sorafenib Might Induce Sarcopenia in Patients With Hepatocellular Carcinoma by Inhibiting Carnitine Absorption. Anticancer Res. 2020, 40, 4173–4182. [Google Scholar] [CrossRef]
- Okubo, H.; Ando, H.; Ishizuka, K.; Kitagawa, R.; Okubo, S.; Saito, H.; Kokubu, S.; Miyazaki, A.; Ikejima, K.; Shiina, S.; et al. Carnitine insufficiency is associated with fatigue during lenvatinib treatment in patients with hepatocellular carcinoma. PLoS ONE 2020, 15, e0229772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marasco, G.; Serenari, M.; Renzulli, M.; Alemanni, L.V.; Rossini, B.; Pettinari, I.; Dajti, E.; Ravaioli, F.; Golfieri, R.; Cescon, M.; et al. Clinical impact of sarcopenia assessment in patients with hepatocellular carcinoma undergoing treatments. J. Gastroenterol. 2020, 55, 927–943. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Trial | Drug(s) | Primary Endpoint | Elderly (%) | Elderly (Efficacy) |
|---|---|---|---|---|
| First line | ||||
| SHARP [112] | Sorafenib vs. placebo | OS: 10.7 vs. 7.9 months (p < 0.001) | Combined analysis: ≥75 y: 16.8% | Combined analysis: <75 y vs. ≥75 y: no difference (p = 0.6304) |
| Asia-Pacific [113] | Sorafenib vs. placebo | OS: 6.5 vs. 4.2 months (p = 0.014) | ||
| REFLECT [114] | Lenvatinib vs. sorafenib | OS: 13.6 vs. 12.3 months (non-inferior) | 65–75 y: 30%≥75 y: 13% | PFS <65 vs. ≥65 y: no difference OS <65 vs. ≥65 y: no difference |
| IMbrave150 [115] | Atezolizumab + bevacizumab vs. sorafenib | 1y-OS: 67.2% vs. 54.6% (p < 0.001) | NR | OS <65 vs. ≥65 y: no difference |
| Second line | ||||
| RESORCE [116] | Regorafenib vs. placebo | OS: 10.6 vs. 7.8 months (p < 0.0001) | ≥65 y: 45% | OS ≥65 y: comparable to overall population |
| CELESTIAL [117] | Cabozantinib vs. placebo | OS: 10.2 vs. 8 months (p = 0.005) | ≥65 y: 48.5% | PFS <65 vs. ≥65 y: no difference OS <65 vs. ≥65 y: no difference |
| REACH [118] | Ramucirumab vs. placebo | OS: 9.2 vs. 7.6 months (p = 0.14) | Pooled analysis: 65–75 y: 18.6% ≥75 y: 9.3% | Pooled analysis: OS <65 vs. 65–75 vs. ≥75 y: no difference |
| REACH-2 [119] | Ramucirumab vs. placebo | OS: 8.5 vs. 7.3 months (p = 0.019) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Federico, P.; Giunta, E.F.; Pappalardo, A.; Tufo, A.; Marte, G.; Attademo, L.; Fabbrocini, A.; Petrillo, A.; Daniele, B. How to Treat Hepatocellular Carcinoma in Elderly Patients. Pharmaceuticals 2021, 14, 233. https://doi.org/10.3390/ph14030233
Federico P, Giunta EF, Pappalardo A, Tufo A, Marte G, Attademo L, Fabbrocini A, Petrillo A, Daniele B. How to Treat Hepatocellular Carcinoma in Elderly Patients. Pharmaceuticals. 2021; 14(3):233. https://doi.org/10.3390/ph14030233
Chicago/Turabian StyleFederico, Piera, Emilio Francesco Giunta, Annalisa Pappalardo, Andrea Tufo, Gianpaolo Marte, Laura Attademo, Antonietta Fabbrocini, Angelica Petrillo, and Bruno Daniele. 2021. "How to Treat Hepatocellular Carcinoma in Elderly Patients" Pharmaceuticals 14, no. 3: 233. https://doi.org/10.3390/ph14030233