A Validation Study of Freezing of Gait (FoG) Detection and Machine-Learning-Based FoG Prediction Using Estimated Gait Characteristics with a Wearable Accelerometer

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Related Work
2.1. Digital Mediums to Detect PD
2.2. Wearables-Based Activity Detection and Validation for the Diagnosis of Parkinson Disease
3. Materials and Methods
3.1. Data Collection and Experimental Procedure
- (1)
- Patients who were diagnosed with PD clinically [33],
- (2)
- Age between 40 and 80,
- (3)
- Hoehn and Yahr stages 2–4,
- (4)
- Patients who showed gait disturbance.
3.2. Study Design
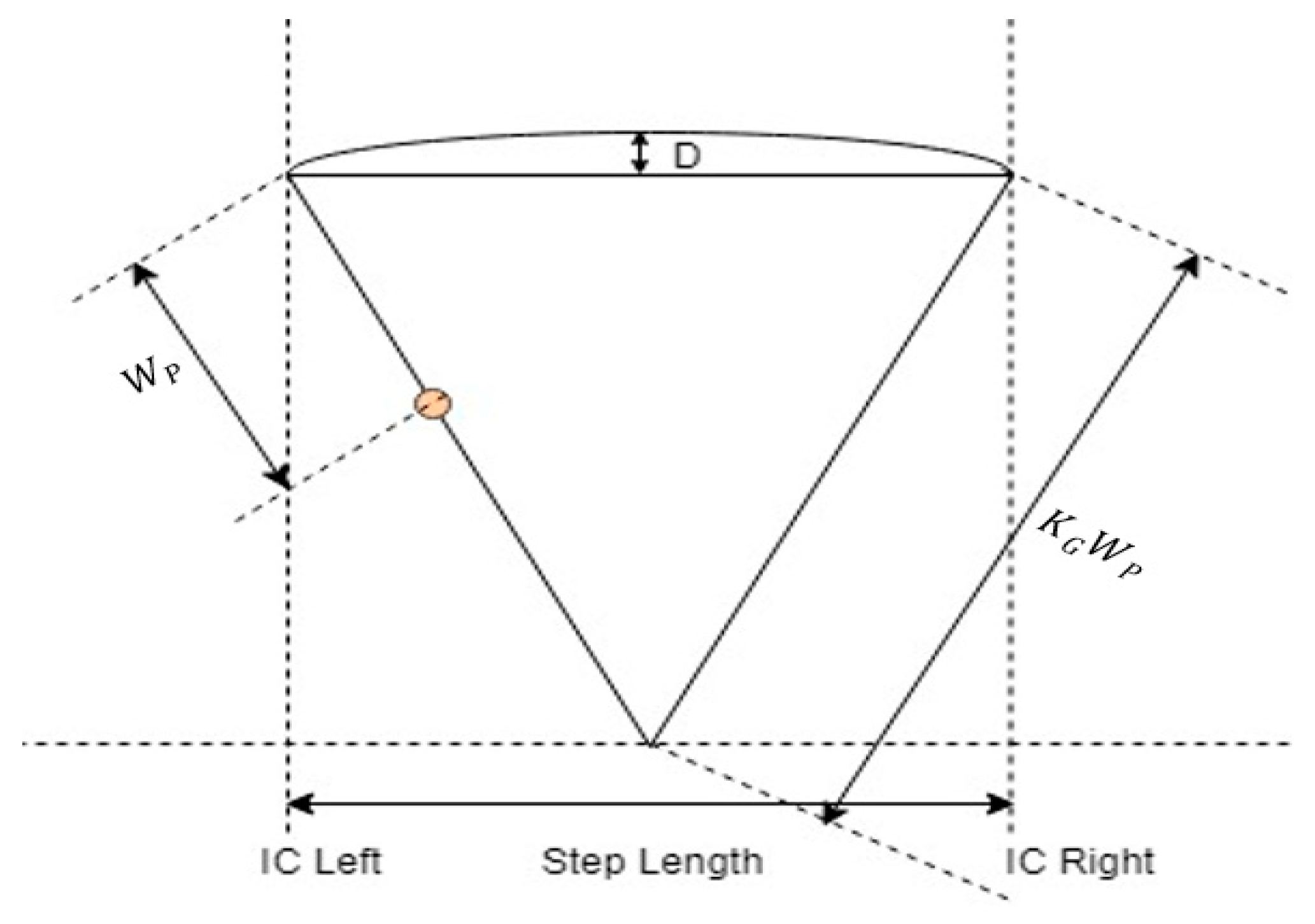
3.3. Gait Cycle Detection with Wearable Accelerometer
3.4. Estimation of Spatiotemporal Gait Parameters and Feature Selection
3.5. Need of Machine Learning Techniques and Its Perfromance Measurement
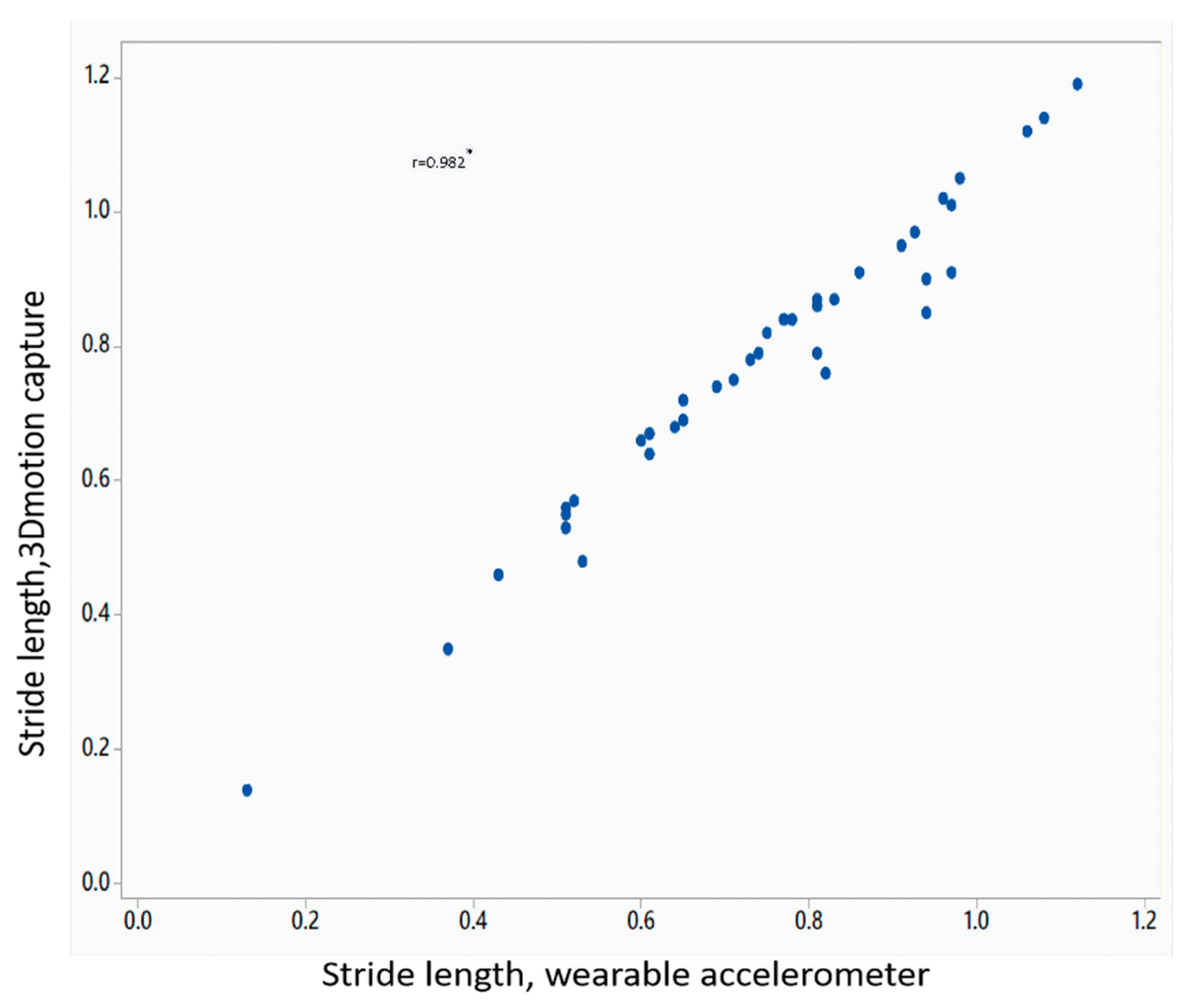
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Fahn, S. The freezing phenomenon in parkinsonism. Adv. Neurol. 1995, 67, 53–63. [Google Scholar] [PubMed]
- Giladi, N.; Treves, T.A.; Simon, E.S.; Shabtai, H.; Orlov, Y.; Kandinov, B.; Paleacu, D.; Korczyn, A.D. Freezing of gait in patients with advanced Parkinson’s disease. J. Neural Transm. 2001, 108, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Bloem, B.R.; Hausdorff, J.M.; Visser, J.E.; Giladi, N. Falls and freezing of gait in Parkinson’s disease: A review of two interconnected, episodic phenomena. Mov. Disord. 2004, 19, 871–884. [Google Scholar] [CrossRef] [PubMed]
- Moreau, C.; Defebvre, L.; Bleuse, S.; Blatt, J.L.; Duhamel, A.; Bloem, B.R.; Destée, A.; Krystkowiak, P. Externally provoked freezing of gait in open runways in advanced Parkinson’s disease results from motor and mental collapse. J. Neural Transm. 2008, 115, 1431–1436. [Google Scholar] [CrossRef] [PubMed]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [PubMed]
- Schaafsma, J.D.; Balash, Y.; Gurevich, T.; Bartels, A.L.; Hausdorff, J.M.; Giladi, N. Characterization of freezing of gait subtypes and the response of each to levodopa in Parkinson’s disease. Eur. J. Neurol. 2003, 10, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Snijders, A.H.; Haaxma, C.A.; Hagen, Y.J.; Munneke, M.; Bloem, B.R. Freezer or non-freezer: Clinical assessment of freezing of gait. Park. Relat. Disord. 2012, 18, 149–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fahn, S. Members of the UPDRS development committee. Unified Parkinson’s disease rating scale. Recent Dev. Parkinson’s Dis. 1987, 2, 293–304. [Google Scholar]
- Martínez-Martín, P.; Gil-Nagel, A.; Gracia, L.M.; Gómez, J.B.; Martinez-Sarries, J.; Bermejo, F.; Cooperative Multicentric Group. Unified Parkinson’s disease rating scale characteristics and structure. Mov. Disord. 1994, 9, 76–83. [Google Scholar]
- Baas, H.; Stecker, K.; Fischer, P.A. Value and appropriate use of rating scales and apparative measurements in quantification of disability in Parkinson’s disease. J. Neural Transm. Park. Dis. Dement. Sect. 1993, 5, 45–61. [Google Scholar] [CrossRef] [PubMed]
- Goetz, C.G.; Stebbins, G.T.; Shale, H.M.; Lang, A.E.; Chernik, D.A.; Chmura, T.A.; Ahlskog, J.E.; Dorflinger, E.E. Utility of an objective dyskinesia rating scale for Parkinson’s disease: Inter-and intrarater reliability assessment. Mov. Disord. 1994, 9, 390–394. [Google Scholar] [CrossRef] [PubMed]
- Steffen, T.M.; Hacker, T.A.; Mollinger, L. Age-and gender-related test performance in community-dwelling elderly people: Six-Minute Walk Test, Berg Balance Scale, Timed Up & Go Test, and gait speeds. Phys. Ther. 2002, 82, 128–137. [Google Scholar] [PubMed]
- Lusardi, M.M.; Pellecchia, G.L.; Schulman, M. Functional performance in community living older adults. J. Geriatr. Phys. Ther. 2003, 26, 14–22. [Google Scholar] [CrossRef]
- Viccaro, L.J.; Perera, S.; Studenski, S.A. Is timed up and go better than gait speed in predicting health, function, and falls in older adults? J. Am. Geriatr. Soc. 2011, 59, 887–892. [Google Scholar] [CrossRef] [PubMed]
- Nocera, J.R.; Stegemöller, E.L.; Malaty, I.A.; Okun, M.S.; Marsiske, M.; Hass, C.J. Using the Timed Up & Go test in a clinical setting to predict falling in Parkinson’s disease. Arch. Phys. Med. Rehabil. 2013, 94, 1300–1305. [Google Scholar] [PubMed]
- Giladi, N.; Shabtai, H.; Simon, E.S.; Biran, S.; Tal, J.; Korczyn, A.D. Construction of freezing of gait questionnaire for patients with Parkinsonism. Park. Relat. Disord. 2000, 6, 165–170. [Google Scholar] [CrossRef]
- Giladi, N.; Tal, J.; Azulay, T.; Rascol, O.; Brooks, D.J.; Melamed, E.; Oertel, W.; Poewe, W.H.; Stocchi, F.; Tolosa, E. Validation of the freezing of gait questionnaire in patients with Parkinson’s disease. Mov. Disord. 2009, 24, 655–661. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, M.H.; Hariz, G.M.; Wictorin, K.; Miller, M.; Forsgren, L.; Hagell, P. Development and testing of a self administered version of the Freezing of Gait Questionnaire. BMC Neurol. 2010, 10, 85. [Google Scholar] [CrossRef] [PubMed]
- Nieuwboer, A.; Weerdt, W.D.; Dom, R.; Lesaffre, E. A frequency and correlation analysis of motor deficits in Parkinson patients. Disabil. Rehabil. 1998, 20, 142–150. [Google Scholar] [CrossRef] [PubMed]
- Maetzler, W.; Klucken, J.; Horne, M. A clinical view on the development of technology-based tools in managing Parkinson’s disease. Mov. Disord. 2016, 31, 1263–1271. [Google Scholar] [CrossRef] [PubMed]
- Lipsmeier, F.; Taylor, K.I.; Kilchenmann, T.; Wolf, D.; Scotland, A.; Schjodt-Eriksen, J.; Cheng, W.Y.; Fernandez-Garcia, I.; Siebourg-Polster, J.; Jin, L.; et al. Evaluation of Smartphone-Based Testing to Generate Exploratory Outcome Measures in a Phase 1 Parkinson’s Disease Clinical Trial. Mov. Disord. 2018, 33, 1287–1297. [Google Scholar] [CrossRef] [PubMed]
- San Luciano, M.; Wang, C.; Ortega, R.A.; Yu, Q.; Boschung, S.; Soto-Valencia, J.; Bressman, S.B.; Lipton, R.B.; Pullman, S.; Saunders-Pullman, R. Digitized spiral drawing: A possible biomarker for early Parkinson’s disease. PLoS ONE 2016, 11, e0162799. [Google Scholar] [CrossRef] [PubMed]
- Walker, R.W.; Zietsma, R.; Gray, W.K. Could a new sensory pen assist in the early diagnosis of Parkinson’s? Expert Rev. Med. Devices 2014, 11, 243–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuhner, A.; Schubert, T.; Maurer, C.; Burgard, W. An online system for tracking the performance of Parkinson’s patients. In Proceedings of the 2017 IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS), Vancouver, BC, Canada, 24–28 September 2017; pp. 1664–1669. [Google Scholar]
- Prasad, R.; Babu, S.; Siddaiah, N.; Rao, K. A review on techniques for diagnosing and monitoring patients with Parkinson’s disease. J. Biosens. Bioelectron. 2016, 7, 203. [Google Scholar]
- Han, J.H.; Lee, W.J.; Ahn, T.B.; Jeon, B.S.; Park, K.S. Gait analysis for freezing detection in patients with movement disorder using three dimensional acceleration system. In Proceedings of the 25th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Cancun, Mexico, 17–21 September 2003; Volume 2, pp. 1863–1865. [Google Scholar]
- Moore, S.T.; Yungher, D.A.; Morris, T.R.; Dilda, V.; MacDougall, H.G.; Shine, J.M.; Naismith, S.L.; Lewis, S.J. Autonomous identification of freezing of gait in Parkinson’s disease from lower-body segmental accelerometry. J. Neuroeng. Rehabil. 2013, 10, 19. [Google Scholar] [CrossRef] [PubMed]
- Azevedo Coste, C.; Sijobert, B.; Pissard-Gibollet, R.; Pasquier, M.; Espiau, B.; Geny, C. Detection of freezing of gait in Parkinson disease: Preliminary results. Sensors 2014, 14, 6819–6827. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Martín, D.; Samà, A.; Pérez-López, C.; Català, A.; Arostegui, J.M.M.; Cabestany, J.; Bayés, À.; Alcaine, S.; Mestre, B.; Prats, A.; et al. Home detection of freezing of gait using support vector machines through a single waist-worn triaxial accelerometer. PLoS ONE 2017, 12, e0171764. [Google Scholar] [CrossRef] [PubMed]
- Mileti, I.; Germanotta, M.; Di Sipio, E.; Imbimbo, I.; Pacilli, A.; Erra, C.; Petracca, M.; Rossi, S.; Del Prete, Z.; Bentivoglio, A.R.; et al. Measuring Gait Quality in Parkinson’s disease through Real-Time Gait Phase Recognition. Sensors 2018, 18, 919. [Google Scholar] [CrossRef] [PubMed]
- Schlachetzki, J.C.; Barth, J.; Marxreiter, F.; Gossler, J.; Kohl, Z.; Reinfelder, S.; Gassner, H.; Aminian, K.; Eskofier, B.M.; Winkler, J.; et al. Wearable sensors objectively measure gait parameters in Parkinson’s disease. PLoS ONE 2017, 12, e0183989. [Google Scholar] [CrossRef] [PubMed]
- Jeon, H.; Lee, W.; Park, H.; Lee, H.; Kim, S.; Kim, H.; Jeon, B.; Park, K. Automatic classification of tremor severity in Parkinson’s disease using a wearable device. Sensors 2017, 17, 2067. [Google Scholar] [CrossRef] [PubMed]
- Hughes, A.J.; Daniel, S.E.; Blankson, S.; Lees, A.J. A clinicopathologic study of 100 cases of Parkinson’s disease. Arch. Neurol. 1993, 50, 140–148. [Google Scholar] [CrossRef] [PubMed]
- Rawassizadeh, R.; Pierson, T.J.; Peterson, R.; Kotz, D. NoCloud: Exploring Network Disconnection through On-Device Data Analysis. IEEE Pervasive Comput. 2018, 17, 64–74. [Google Scholar] [CrossRef]
- Chang, Y.F.; Ding, J.J.; Hu, H.; Yang, W.C.; Lin, K.H.; Wu, P.H. A real-time detection algorithm for freezing of gait in Parkinson’s disease. In Proceedings of the 2014 IEEE International Symposium on Circuits and Systems (ISCAS), Melbourne, Australia, 1–5 June 2014; pp. 1312–1315. [Google Scholar]
- Hollman, J.H.; McDade, E.M.; Petersen, R.C. Normative spatiotemporal gait parameters in older adults. Gait Posture 2011, 34, 111–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alcock, L.; Galna, B.; Perkins, R.; Lord, S.; Rochester, L. Step length determines minimum toe clearance in older adults and people with Parkinson’s disease. J. Biomech. 2018, 71, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Del Din, S.; Godfrey, A.; Rochester, L. Validation of an accelerometer to quantify a comprehensive battery of gait characteristics in healthy older adults and Parkinson’s disease: Toward clinical and at home use. IEEE J. Biomed. Health Inform. 2016, 20, 838–847. [Google Scholar] [CrossRef] [PubMed]
- Del Din, S.; Hickey, A.; Ladha, C.; Stuart, S.; Bourke, A.K.; Esser, P.; Rochester, L.; Godfrey, A. Instrumented gait assessment with a single wearable: An introductory tutorial. F1000Research 2016, 5, 2323. [Google Scholar] [CrossRef]
- Millecamps, A.; Lowry, K.A.; Brach, J.S.; Perera, S.; Redfern, M.S.; Sejdić, E. Understanding the effects of pre-processing on extracted signal features from gait accelerometry signals. Comput. Boil. Med. 2015, 62, 164–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kobsar, D.; Ferber, R. Wearable Sensor Data to Track Subject-Specific Movement Patterns Related to Clinical Outcomes Using a Machine Learning Approach. Sensors 2018, 18, 2828. [Google Scholar] [CrossRef] [PubMed]
- Saad, A. Detection of Freezing of Gait in Parkinson’s Disease; Automatic Control Engineering, Université du Havre: Le Havre, France, 2016. [Google Scholar]
- Rawassizadeh, R.; Tomitsch, M.; Nourizadeh, M.; Momeni, E.; Peery, A.; Ulanova, L.; Pazzani, M. Energy-efficient integration of continuous context sensing and prediction into smartwatches. Sensors 2015, 15, 22616–22645. [Google Scholar] [CrossRef] [PubMed]
- Rehman, M.; Liew, C.; Wah, T.; Shuja, J.; Daghighi, B. Mining personal data using smartphones and wearable devices: A survey. Sensors 2015, 15, 4430–4469. [Google Scholar] [CrossRef] [PubMed]
- Banaee, H.; Ahmed, M.U.; Loutfi, A. Data mining for wearable sensors in health monitoring systems: A review of recent trends and challenges. Sensors 2013, 13, 17472–17500. [Google Scholar] [CrossRef] [PubMed]
- Howcroft, J.; Lemaire, E.D.; Kofman, J. Wearable-sensor-based classification models of faller status in older adults. PLoS ONE 2016, 11, e0153240. [Google Scholar] [CrossRef] [PubMed]
- Castro, D.; Coral, W.; Rodriguez, C.; Cabra, J.; Colorado, J. Wearable-Based Human Activity Recognition Using an IoT Approach. J. Sens. Actuator Netw. 2017, 6, 28. [Google Scholar] [CrossRef]
- Sijobert, B.; Benoussaad, M.; Denys, J.; Pissard-Gibollet, R.; Geny, C.; Coste, C.A. Implementation and Validation of a Stride Length Estimation Algorithm, Using a Single Basic Inertial Sensor on Healthy Subjects and Patients Suffering from Parkinson’s Disease. Electron. Healthc. 2015, 7, 704–714. [Google Scholar] [CrossRef]
- Handojoseno, A.A.; Shine, J.M.; Nguyen, T.N.; Tran, Y.; Lewis, S.J.; Nguyen, H.T. The detection of Freezing of Gait in Parkinson’s disease patients using EEG signals based on Wavelet decomposition. In Proceedings of the 2012 Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), San Diego, CA, USA, 28 August–1 September 2012; pp. 69–72. [Google Scholar]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Feature Variable | Feature Name | Description |
|---|---|---|
| avg_step_time | Average step time | Average time elapsed for each step |
| avg_stride_time | Average stride time | Average time elapsed for each stride |
| avg_step_length | Average step length | Average distance covered in each step |
| avg_stride_length | Average stride length | Average distance covered in each stride |
| walking_speed | Walking speed | Gait velocity or speed of walking |
| sigma_x | Standard deviation of acceleration along x-axis | Measure for signal spreading characterized as mean deviation of the signal compared to the average |
| sigma_y | Standard deviation of acceleration along y-axis | |
| sigma_z | Standard deviation of acceleration along z-axis | |
| S_xy | Zeroth-Lag cross-correlation coefficient between accelerations along x-axis and y-axis | Agreement or similarity between acceleration signals |
| S_xz | Zeroth-Lag cross-correlation coefficient between accelerations along x-axis and z-axis | |
| S_yz | Zeroth-Lag cross-correlation coefficient between accelerations along y-axis and z-axis | |
| harmonic_x | Harmonic ratio for acceleration along x-axis | Harmonic composition of the accelerations for a given stride |
| harmonic_y | Harmonic ratio for acceleration along y-axis | |
| harmonic_z | Harmonic ratio for acceleration along z-axis |
| S. No. | Parameters | Mean Value (3D Motion Capture) | Mean Value (Algorithm) | Mean Error Rate (%) |
|---|---|---|---|---|
| 1 | Step Time (s) | 0.53 | 0.57 | 7.64 ± 2.41 |
| 2 | Stride Time (s) | 1.17 | 1.13 | 5.45 ± 3.57 |
| 3 | Step length (cm) | 0.38 | 0.35 | 6.35 ± 2.45 |
| 4 | Stride Length (cm) | 0.73 | 0.71 | 6.25 ± 2.81 |
| 5 | Walking Speed (cm/s) | 0.68 | 0.65 | 6.52 ± 3.23 |
| (a) SVM | |||||||||||
| Simulation | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | Mean |
| Accuracy (%) | 85.71 | 88.57 | 88.57 | 91.42 | 88.57 | 88.57 | 91.42 | 88.57 | 88.57 | 91.42 | 89.139 |
| Sensitivity (%) | 85.11 | 87.91 | 87.91 | 90.89 | 87.91 | 87.91 | 90.89 | 87.91 | 87.91 | 90.89 | 88.524 |
| Specificity (%) | 85.34 | 88.12 | 88.12 | 91.21 | 88.12 | 88.12 | 91.21 | 88.12 | 88.12 | 91.21 | 88.769 |
| (b) k-NN | |||||||||||
| Simulation | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | Mean |
| Accuracy (%) | 85.29 | 85.29 | 85.29 | 82.35 | 85.29 | 85.29 | 82.35 | 85.29 | 85.29 | 85.29 | 84.702 |
| Sensitivity (%) | 84.97 | 84.98 | 84.97 | 82.11 | 84.98 | 84.98 | 82.12 | 84.98 | 84.98 | 84.98 | 84.405 |
| Specificity (%) | 84.98 | 84.98 | 84.98 | 82.23 | 84.98 | 84.98 | 84.98 | 84.98 | 84.98 | 84.98 | 84.705 |
| (c) Decision Tree | |||||||||||
| Simulation | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | Mean |
| Accuracy (%) | 85.88 | 87.12 | 87.12 | 85.88 | 85.88 | 87.12 | 87.12 | 87.12 | 87.12 | 87.12 | 86.748 |
| Sensitivity (%) | 85.56 | 86.98 | 86.97 | 85.56 | 85.56 | 86.97 | 86.97 | 86.97 | 86.97 | 86.97 | 86.548 |
| Specificity (%) | 85.67 | 86.99 | 86.99 | 85.67 | 85.67 | 86.99 | 86.99 | 86.99 | 86.99 | 86.99 | 86.594 |
| (d) NB | |||||||||||
| Simulation | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | Mean |
| Accuracy (%) | 83.12 | 82.89 | 82.89 | 83.12 | 83.12 | 82.89 | 83.12 | 83.12 | 83.12 | 83.12 | 83.051 |
| Sensitivity (%) | 82.92 | 82.48 | 82.47 | 82.92 | 82.92 | 82.48 | 82.92 | 82.92 | 82.92 | 82.92 | 82.787 |
| Specificity (%) | 82.97 | 82.54 | 82.53 | 82.97 | 82.97 | 82.54 | 82.97 | 82.97 | 82.97 | 82.97 | 82.84 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aich, S.; Pradhan, P.M.; Park, J.; Sethi, N.; Vathsa, V.S.S.; Kim, H.-C. A Validation Study of Freezing of Gait (FoG) Detection and Machine-Learning-Based FoG Prediction Using Estimated Gait Characteristics with a Wearable Accelerometer. Sensors 2018, 18, 3287. https://doi.org/10.3390/s18103287
Aich S, Pradhan PM, Park J, Sethi N, Vathsa VSS, Kim H-C. A Validation Study of Freezing of Gait (FoG) Detection and Machine-Learning-Based FoG Prediction Using Estimated Gait Characteristics with a Wearable Accelerometer. Sensors. 2018; 18(10):3287. https://doi.org/10.3390/s18103287
Chicago/Turabian StyleAich, Satyabrata, Pyari Mohan Pradhan, Jinse Park, Nitin Sethi, Vemula Sai Sri Vathsa, and Hee-Cheol Kim. 2018. "A Validation Study of Freezing of Gait (FoG) Detection and Machine-Learning-Based FoG Prediction Using Estimated Gait Characteristics with a Wearable Accelerometer" Sensors 18, no. 10: 3287. https://doi.org/10.3390/s18103287