
The Efficiency and Its Determinants for China’s Medical Care System: Some Policy Implications for Northeast Asia

Abstract
:1. Introduction
- i.
- What are the technical efficiency scores and the dynamics for the hospitals in different provinces of China during the period of 2002–2013?
- ii.
- How the external environmental factors affect the technical efficiency of Chinese hospitals? Have the medical reform improve the technical efficiency of Chinese hospitals?
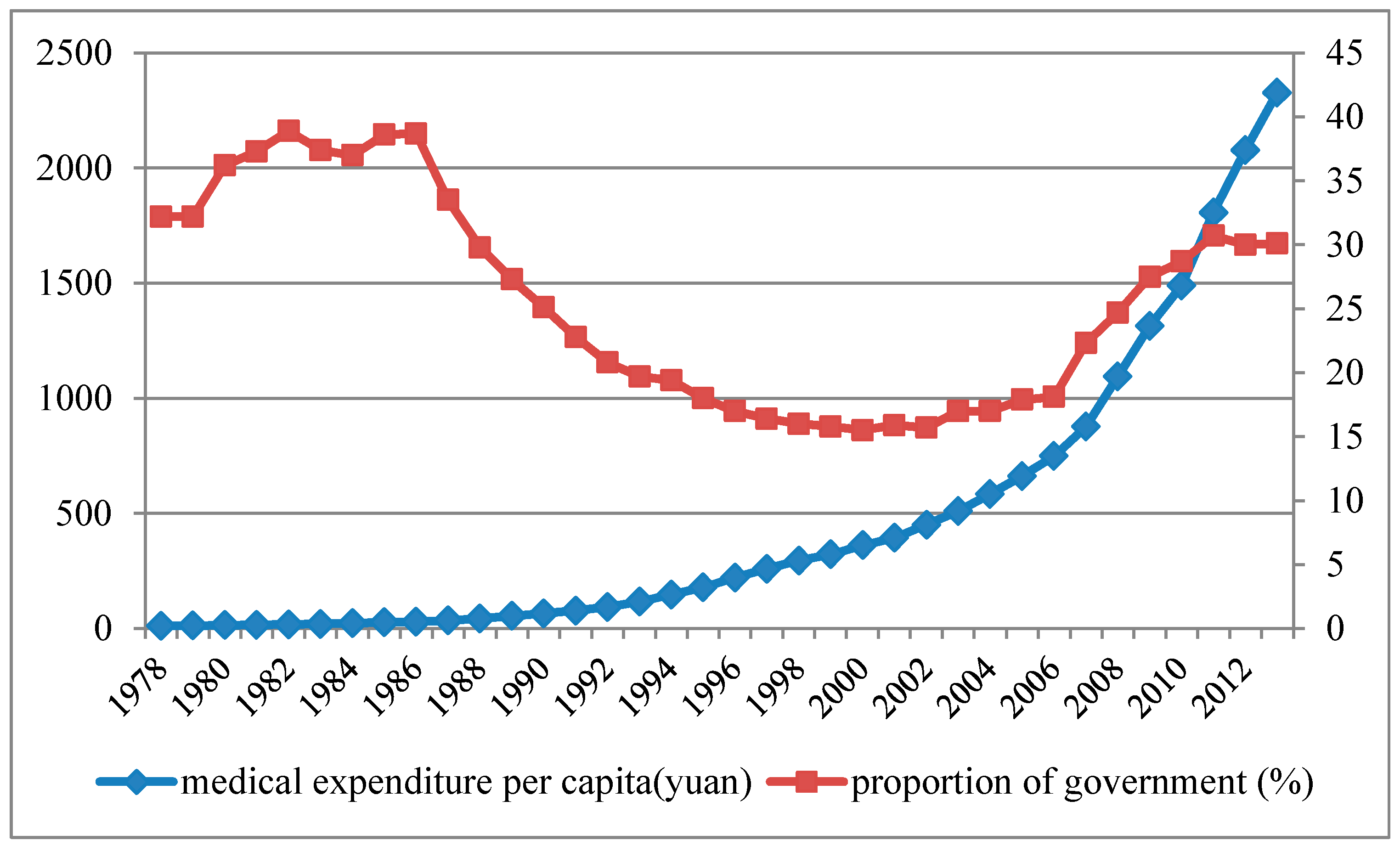
2. The Medical Care System of China

3. Methodology
3.1. Global Generalized Directional Distance Function
3.2. Tobit Model
3.3. Background Literature and Descriptive Data

{kind=link}
{kind=link}
{kind=link}
| Variable | Definition | Observation | Mean | Std. Dev. | Min | Max |
|---|---|---|---|---|---|---|
| total staff | the number of total staff in the hospitals | 372 | 207,046.2 | 130,728.4 | 10,058 | 684,976 |
| total assets | the total assets of hospitals (million yuan) | 372 | 43,800.00 | 39,800.00 | 717.00 | 216,000.00 |
| beds | the number of beds in the hospitals | 372 | 100,245.90 | 79,129.75 | 4238.00 | 1,027,919.00 |
| total revenue | the total revenue of hospitals (million yuan) | 372 | 34,200.00 | 34,500.00 | 588.00 | 214,000.00 |
| surgery | the total number of surgeries | 372 | 748,730.00 | 997,765.20 | 6230.00 | 16,000,000.00 |
| mortality | the mortality ratio in different provinces | 372 | 5.96 | 0.67 | 4.21 | 7.30 |
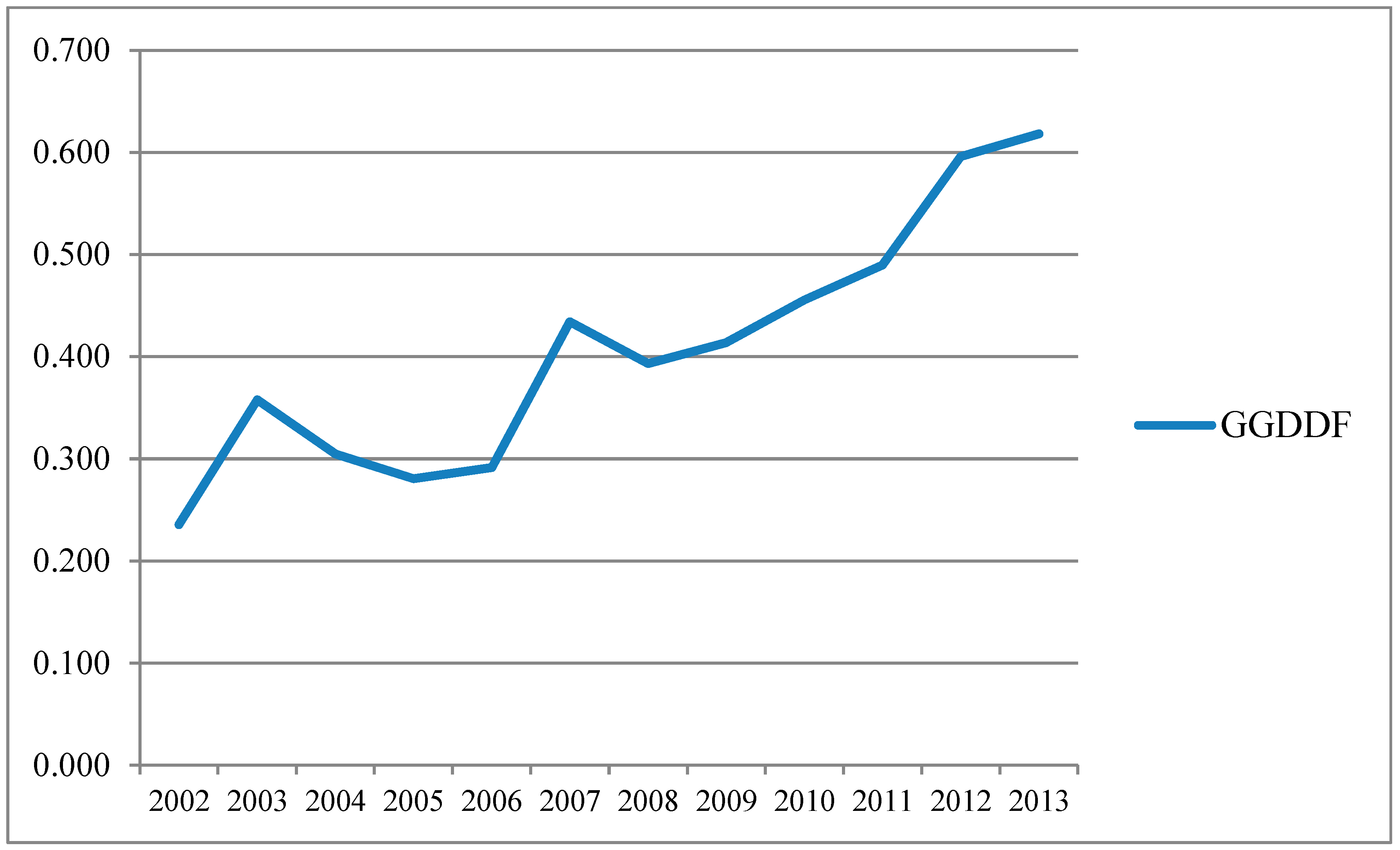
4. Technical Efficiency Estimation
| Province | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Anhui | 0.181 | 0.166 | 0.358 | 0.285 | 0.271 | 0.519 | 0.354 | 0.402 | 0.415 | 0.444 | 0.512 | 0.522 |
| Beijing | 0.368 | 1.000 | 0.393 | 0.396 | 0.518 | 0.451 | 0.547 | 0.594 | 0.644 | 0.730 | 0.968 | 1.000 |
| Chongqing | 0.196 | 0.315 | 0.222 | 0.246 | 0.254 | 0.323 | 0.626 | 0.404 | 0.424 | 0.443 | 0.549 | 0.574 |
| Fujian | 0.267 | 0.344 | 0.306 | 0.320 | 0.326 | 0.934 | 0.364 | 0.332 | 0.418 | 0.389 | 0.579 | 0.602 |
| Gansu | 0.159 | 0.196 | 0.181 | 0.164 | 0.164 | 0.500 | 0.241 | 0.200 | 0.359 | 0.370 | 0.425 | 0.460 |
| Guangdong | 0.337 | 0.249 | 0.497 | 0.463 | 0.450 | 0.492 | 0.569 | 0.625 | 0.690 | 0.807 | 0.952 | 1.000 |
| Guangxi | 0.146 | 0.183 | 0.261 | 0.275 | 0.280 | 0.339 | 0.354 | 0.406 | 0.446 | 0.492 | 0.599 | 0.636 |
| Guizhou | 0.177 | 0.264 | 0.203 | 0.237 | 0.274 | 0.412 | 0.347 | 0.446 | 0.452 | 0.478 | 0.536 | 0.565 |
| Hainan | 0.213 | 1.000 | 0.166 | 0.197 | 0.189 | 0.252 | 0.270 | 0.316 | 0.360 | 0.381 | 0.450 | 0.473 |
| Hebei | 0.534 | 0.118 | 0.278 | 0.291 | 0.289 | 0.374 | 0.405 | 0.486 | 0.487 | 0.468 | 0.606 | 0.595 |
| Heilongjiang | 0.167 | 0.190 | 0.275 | 0.299 | 0.300 | 0.407 | 0.414 | 0.477 | 0.438 | 0.463 | 0.533 | 0.544 |
| Henan | 0.217 | 0.092 | 0.284 | 0.311 | 0.310 | 0.363 | 0.415 | 0.472 | 0.496 | 0.514 | 0.622 | 0.618 |
| Hubei | 0.242 | 0.180 | 0.353 | 0.307 | 0.308 | 0.386 | 0.512 | 0.455 | 0.462 | 0.472 | 0.566 | 0.573 |
| Hunan | 0.233 | 0.155 | 0.289 | 0.282 | 0.295 | 0.616 | 0.379 | 0.320 | 0.458 | 0.479 | 0.589 | 0.641 |
| Inner Mongolia | 0.141 | 0.158 | 0.207 | 0.210 | 0.238 | 0.289 | 0.298 | 0.279 | 0.390 | 0.424 | 0.491 | 0.490 |
| Jiangsu | 0.357 | 0.232 | 0.589 | 0.394 | 0.405 | 0.445 | 0.460 | 0.495 | 0.521 | 0.555 | 0.690 | 0.726 |
| Jiangxi | 0.223 | 0.172 | 0.321 | 0.260 | 0.264 | 0.627 | 0.342 | 0.340 | 0.442 | 0.467 | 0.546 | 0.550 |
| Jilin | 0.221 | 0.196 | 0.271 | 0.226 | 0.244 | 0.323 | 0.416 | 0.449 | 0.420 | 0.420 | 0.524 | 0.575 |
| Liaoning | 0.073 | 0.135 | 0.285 | 0.295 | 0.314 | 0.471 | 0.407 | 0.449 | 0.476 | 0.502 | 0.637 | 0.652 |
| Ningxia | 0.070 | 1.000 | 0.172 | 0.191 | 0.185 | 0.222 | 0.265 | 0.303 | 0.337 | 0.359 | 0.419 | 0.461 |
| Qinghai | 0.072 | 0.984 | 0.129 | 0.141 | 0.152 | 0.283 | 0.212 | 0.267 | 0.296 | 0.346 | 0.432 | 0.477 |
| Shaanxi | 0.352 | 0.179 | 0.212 | 0.207 | 0.225 | 0.270 | 0.320 | 0.354 | 0.412 | 0.454 | 0.553 | 0.564 |
| Shandong | 0.417 | 0.113 | 0.383 | 0.317 | 0.342 | 0.429 | 0.448 | 0.485 | 0.511 | 0.552 | 0.661 | 0.681 |
| Shanghai | 0.419 | 0.578 | 0.576 | 0.490 | 0.492 | 0.522 | 0.613 | 0.640 | 0.675 | 0.801 | 0.966 | 1.000 |
| Shanxi | 0.221 | 0.146 | 0.327 | 0.213 | 0.249 | 0.630 | 0.283 | 0.255 | 0.383 | 0.398 | 0.522 | 0.561 |
| Sichuan | 0.250 | 0.140 | 0.277 | 0.308 | 0.299 | 0.448 | 0.417 | 0.495 | 0.510 | 0.535 | 0.636 | 0.653 |
| Tianjin | 0.310 | 0.864 | 0.338 | 0.351 | 0.338 | 0.453 | 0.410 | 0.490 | 0.525 | 0.598 | 0.659 | 0.732 |
| Tibet | 0.097 | 1.000 | 0.243 | 0.088 | 0.121 | 0.473 | 0.201 | 0.263 | 0.207 | 0.259 | 0.349 | 0.300 |
| Xinjiang | 0.209 | 0.213 | 0.274 | 0.280 | 0.246 | 0.392 | 0.323 | 0.351 | 0.429 | 0.463 | 0.547 | 0.550 |
| Yunnan | 0.077 | 0.217 | 0.226 | 0.236 | 0.255 | 0.299 | 0.394 | 0.396 | 0.418 | 0.451 | 0.517 | 0.513 |
| Zhejiang | 0.357 | 0.316 | 0.544 | 0.419 | 0.440 | 0.520 | 0.584 | 0.579 | 0.620 | 0.657 | 0.839 | 0.878 |


5. Determinants of Technical Efficiency for Chinese Hospitals
5.1. Model and Variables Specification
| Variable | Description | Observations | Mean | Std. Dev. | Min | Max |
|---|---|---|---|---|---|---|
| gdpp | GDP per capita | 372 | 9.766 | 0.648 | 8.089 | 11.228 |
| popd | population density | 372 | 0.413 | 0.598 | 0.002 | 3.833 |
| suby | government subsidy | 372 | 14.937 | 8.122 | 3.037 | 59.232 |
| best | ratio of 3A hospitals | 372 | 4.180 | 2.431 | 0.792 | 13.143 |
| reform1 | NRCMS reform | 372 | 0.833 | 0.373 | 0 | 1 |
| reform2 | BSMIS reform | 372 | 0.500 | 0.501 | 0 | 1 |
| area | location | 372 | 0.935 | 0.841 | 0 | 2 |
| TE | gdpp | popd | suby | best | reform1 | reform2 | |
|---|---|---|---|---|---|---|---|
| TE | 1 | ||||||
| gdpp | 0.663 *** | 1 | |||||
| popd | 0.401 *** | 0.529 *** | 1 | ||||
| suby | −0.304 *** | −0.172 *** | −0.272 *** | 1 | |||
| best | 0.370 *** | 0.499 *** | 0.588 *** | −0.303 *** | 1 | ||
| reform1 | 0.260 *** | 0.433 *** | 0.026 | −0.049 | 0.05 | 1 | |
| reform2 | 0.472 *** | 0.554 *** | 0.039 | 0.069 | 0.06 | 0.447 *** | 1 |
5.2. Empirical Results
| (1) | (2) | (3) | (4) | (5) | |
|---|---|---|---|---|---|
| gdpp | 0.100 *** | 0.075 *** | 0.073 *** | 0.073 *** | 0.083 *** |
| (5.79) | (4.54) | (4.74) | (4.74) | (4.50) | |
| popd | 0.066 *** | 0.052 *** | 0.050 *** | 0.050 *** | 0.049 *** |
| (5.16) | (4.01) | (3.65) | (3.65) | (3.48) | |
| suby | −0.007 *** | −0.007 *** | −0.007 *** | −0.007 *** | |
| (−5.47) | (−5.39) | (−5.39) | (−4.96) | ||
| best | 0.001 | 0.001 | 0.002 | ||
| (0.34) | (0.34) | (0.53) | |||
| reform1 | 0.173 *** | 0.168 *** | |||
| (5.06) | (4.84) | ||||
| reform2 | 0.137 *** | 0.131 *** | |||
| (3.81) | (3.57) | ||||
| area | 0.010 | ||||
| (0.75) | |||||
| _cons | −0.694 *** | −0.370 ** | −0.359 ** | −0.359 ** | −0.452 *** |
| (−4.51) | (−2.43) | (−2.49) | (−2.49) | (−2.64) | |
| sigma | |||||
| _cons | 0.126 *** | 0.113 *** | 0.113 *** | 0.113 *** | 0.113 *** |
| (10.61) | (11.63) | (11.63) | (11.63) | (11.78) | |
| Year effects | Yes | Yes | Yes | Yes | Yes |
| Log pseudolikelihood | 265.97 | 265.53 | 265.53 | 265.49 | 227.14 |
| F | 55.09 | 59.66 | 59.65 | 63.51 | 58.61 |
| N | 372 | 372 | 372 | 372 | 372 |
6. Discussion
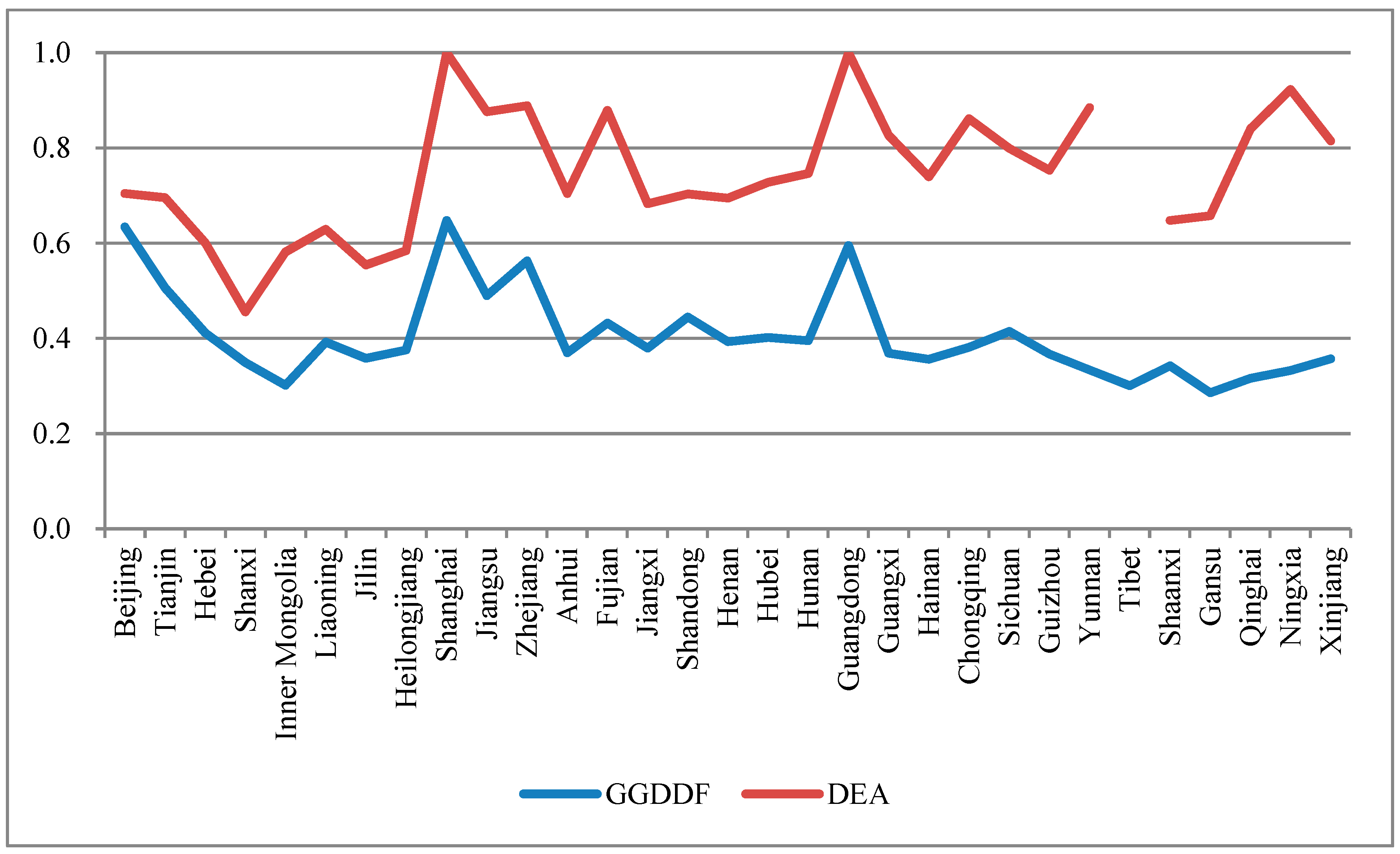
6.1. Technical Efficiency Estimation Compared with Other Research
6.2. Discussion on Determinants of Sustainability Technical Efficiency for Chinese Hospitals
7. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- State Council DRC Research Project. Assessment of China’s medical and health system reform and suggestions. China Health Policy 2005, 9, 4–7. [Google Scholar]
- Flaherty, J.H.; Liu, M.L.; Ding, L.; Dong, B.; Ding, Q.; Li, X.; Xiao, S. China: The aging giant. J. Am. Geriatr. Soc. 2007, 55, 1295–1300. [Google Scholar] [CrossRef] [PubMed]
- World Bank. World Development Report 2007: Development and the Next Generation; World Bank Publications: Washington, DC, USA, 2006. [Google Scholar]
- Arah, O.A.; Klazinga, N.S.; Delnoij, D.M.J.; Ten Asbroek, A.H.A.; Custers, T. Conceptual frameworks for health systems performance: A quest for effectiveness, quality, and improvement. Int. J. Qual. Health Care 2003, 15, 377–398. [Google Scholar] [CrossRef] [PubMed]
- Fukuyama, H.; Shiraz, R.K. Cost-effectiveness measures on convex and nonconvex technologies. Eur. J. Oper. Res. 2015, 246, 307–319. [Google Scholar] [CrossRef]
- Jacobs, R. Alternative methods to examine hospital efficiency: Data envelopment analysis and stochastic frontier analysis. Health Care Manag. Sci. 2001, 4, 103–115. [Google Scholar] [CrossRef] [PubMed]
- Docherty, P.; Kira, M.; Shani, A.R. Creating Sustainable Work Systems (2nd Ed): Developing Social Sustainability; Routledge: London, UK, 2008. [Google Scholar]
- Rosenberg-Yunger, Z.R.; Daar, A.S.; Singer, P.A.; Martin, D.K. Healthcare sustainability and the challenges of innovation to biopharmaceuticals in Canada. Health Policy 2008, 87, 359–368. [Google Scholar] [CrossRef] [PubMed]
- Magnussen, J. Efficiency measurement and the operationalization of hospital production. Health Serv. Res. 1996, 31, 21–37. [Google Scholar] [PubMed]
- Li, H.; Dong, S.; Liu, T. Relative efficiency and productivity: A preliminary exploration of public hospitals in Beijing, China. BMC Health Serv. Res. 2014. [Google Scholar] [CrossRef] [PubMed]
- Hollingsworth, B. The measurement of efficiency and productivity of health care delivery. Health Econ. 2008, 17, 1107–1128. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.; Akdede, S.H. The influence of governance on public sector efficiency: A cross-country analysis. Soc. Sci. J. 2011, 48, 735–738. [Google Scholar] [CrossRef]
- Ng, Y.C. The productive efficiency of Chinese hospitals. China Econ. Rev. 2011, 22, 428–439. [Google Scholar] [CrossRef]
- Hu, H.H.; Qi, Q.; Yang, C.H. Analysis of hospital technical efficiency in China: Effect of health insurance reform. China Econ. Rev. 2012, 23, 865–877. [Google Scholar] [CrossRef]
- Barros, C.P.; de Menezes, A.G.; Vieira, J.C. Measurement of hospital efficiency, using a latent class stochastic frontier model. Appl. Econ. 2013, 45, 47–54. [Google Scholar] [CrossRef]
- Barros, C.P.; de Menezes, A.G.; Peypoch, N.; Solonandrasana, B.; Vieira, J.C. An analysis of hospital efficiency and productivity growth using the Luenberger indicator. Health Care Manag. Sci. 2008, 11, 373–381. [Google Scholar] [CrossRef] [PubMed]
- Hsu, Y.C. The efficiency of government spending on health: Evidence from Europe and Central Asia. Soc. Sci. J. 2013, 50, 665–673. [Google Scholar] [CrossRef]
- Zhang, N.; Choi, Y. A note on the evolution of directional distance function and its development in energy and environmental studies 1997–2013. Renew. Sustain. Energy Rev. 2014, 33, 50–59. [Google Scholar] [CrossRef]
- Yu, Y.; Choi, Y.; Zhang, N. Strategic corporate sustainability performance of Chinese state-owned listed firms: A meta-frontier generalized directional distance function approach. Soc. Sci. J. 2014, 52, 300–310. [Google Scholar] [CrossRef]
- Zhang, N.; Kong, F.; Choi, Y. Measuring sustainability performance for China: A sequential generalized directional distance function approach. Econ. Model. 2014, 41, 392–397. [Google Scholar] [CrossRef]
- Chung, Y.H.; Färe, R.; Grosskopf, S. Productivity and undesirable outputs: A directional distance function approach. J. Environ. Manag. 1997, 51, 229–240. [Google Scholar] [CrossRef]
- Chambers, R.G.; Chung, Y.; Färe, R. Benefit and distance functions. J. Econ. Theory 1996, 70, 407–419. [Google Scholar] [CrossRef]
- Chambers, R.G.; Chung, Y.; Färe, R. Profit, directional distance functions, and Nerlovian efficiency. J. Optimiz. Theory Appl. 1998, 98, 351–364. [Google Scholar] [CrossRef]
- Fukuyama, H.; Weber, W.L. A directional slacks-based measure of technical inefficiency. Socio-Econ. Plan. Sci. 2009, 43, 274–287. [Google Scholar] [CrossRef]
- Färe, R.; Grosskopf, S. Directional distance functions and slacks-based measures of efficiency. Eur. J. Oper. Res. 2010, 200, 320–322. [Google Scholar] [CrossRef]
- Färe, R.; Grosskopf, S. Directional distance functions and slacks-based measures of efficiency: Some clarifications. Eur. J. Oper. Res. 2010, 206, 702. [Google Scholar] [CrossRef]
- Zhang, N.; Zhou, P.; Choi, Y. Energy efficiency, CO2 emission performance and technology gaps in fossil fuel electricity generation in Korea: A meta-frontier non-radial directional distance functionanalysis. Energy Policy 2013, 56, 653–662. [Google Scholar] [CrossRef]
- Mei, G.; Gan, J.; Zhang, N. Metafrontier environmental efficiency for China’s regions: A slack-based efficiency measure. Sustainability 2015, 7, 4004–4021. [Google Scholar] [CrossRef]
- Zhou, P.; Ang, B.W.; Wang, H. Energy and CO2 emission performance in electricity generation: A non-radial directional distance function approach. Eur. J. Oper. Res. 2012, 221, 625–635. [Google Scholar] [CrossRef]
- Oh, D.H. A global Malmquist-Luenberger productivity index. J. Product. Anal. 2010, 34, 183–197. [Google Scholar] [CrossRef]
- Eggleston, K.; Ling, L.; Qingyue, M.; Lindelow, M.; Wagstaff, A. Health service delivery in China: A literature review. Health Econ. 2008, 17, 149–165. [Google Scholar] [CrossRef] [PubMed]
- Wagstaff, A.; Yip, W.; Lindelow, M.; Hsiao, W.C. China’s health system and its reform: A review of recent studies. Health Econ. 2009, 18, 7–23. [Google Scholar] [CrossRef] [PubMed]
- Hsiao, W.C. The Chinese health care system: Lessons for other nations. Soc. Sci. Med. 1995, 41, 1047–1055. [Google Scholar] [CrossRef]
- Dong, W. Health Care Reform in Urban China. Available online: Munkschool.utoronto.ca/cphs/wp-content/uploads/2012/03/Weizhen_Dong-2001-02.pdf (accessed on 8 June 2015).
- Audibert, M.; Mathonnat, J.; Pelissier, A.; Huang, X.X.; Ma, A. Health insurance reform and efficiency of township hospitals in rural China: An analysis from survey data. China Econ. Rev. 2013, 27, 326–338. [Google Scholar] [CrossRef]
- Dong, K. Medical insurance system evolution in China. China Econ. Rev. 2009, 20, 591–597. [Google Scholar] [CrossRef]
- Yip, W.; Hsiao, W. China’s health care reform: A tentative assessment. China Econ. Rev. 2009, 20, 613–619. [Google Scholar] [CrossRef]
- World Bank. Fixing the Public Hospital System in China: China Health Policy Notes No.2; World Bank Publications: Washington, DC, USA, 2010. [Google Scholar]
- Gu, E.; Zhang, J. Health care regime change in urban China: Unmanaged marketization and reluctant privatization. Pac. Aff. 2006, 79, 49–71. [Google Scholar] [CrossRef]
- National Health and Family Planning Commission of the People’s Republic of China. China’s Health and Family Planning Yearbook 2014; Peking Union Medical College Press: Beijing, China, 2015. [Google Scholar]
- Koop, G.; Osiewalski, J.; Steel, M.F. Bayesian efficiency analysis through individual effects: Hospital cost frontiers. J. Econom. 1997, 76, 77–105. [Google Scholar] [CrossRef]
- Rosko, M.D.; Mutter, R.L. Stochastic frontier analysis of hospital inefficiency: A review of empirical issues and an assessment of robustness. Med. Care Res. Rev. 2008, 65, 131–166. [Google Scholar] [CrossRef] [PubMed]
- Varabyova, Y.; Schreyögg, J. International comparisons of the technical efficiency of the hospital sector: Panel data analysis of OECD countries using parametric and non-parametric approaches. Health Policy 2013, 112, 70–79. [Google Scholar] [CrossRef] [PubMed]
- Biørn, E.; Hagen, T.P.; Iversen, T.; Magnussen, J. The effect of activity-based financing on hospital efficiency: A panel data analysis of DEA efficiency scores 1992–2000. Health Care Manag. Sci. 2003, 6, 271–283. [Google Scholar] [CrossRef] [PubMed]
- Ozcan, Y.A. Sensitivity analysis of hospital efficiency under alternative output/input and peer groups: A review. Knowl. Technol. Policy 1992, 5, 1–29. [Google Scholar] [CrossRef]
- Zuckerman, S.; Hadley, J.; Iezzoni, L. Measuring hospital efficiency with frontier cost functions. J. Health Econ. 1994, 13, 255–280. [Google Scholar] [CrossRef]
- Xue, Y.; Liang, H.; Wu, X.; Gong, H.; Li, B.; Zhang, Y. Effects of electronic medical record in a Chinese hospital: A time series study. Int. J. Med. Inform. 2012, 81, 683–689. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health of the People’s Republic of China. China’s Health Statistical Yearbook 2003; Peking Union Medical College Press: Beijing, China, 2004.
- Ministry of Health of the People’s Republic of China. China’s Health Statistical Yearbook 2004; Peking Union Medical College Press: Beijing, China, 2005.
- Ministry of Health of the People’s Republic of China. China’s Health Statistical Yearbook 2005; Peking Union Medical College Press: Beijing, China, 2006.
- Ministry of Health of the People’s Republic of China. China’s Health Statistical Yearbook 2006; Peking Union Medical College Press: Beijing, China, 2007.
- Ministry of Health of the People’s Republic of China. China’s Health Statistical Yearbook 2007; Peking Union Medical College Press: Beijing, China, 2008.
- Ministry of Health of the People’s Republic of China. China’s Health Statistical Yearbook 2008; Peking Union Medical College Press: Beijing, China, 2009.
- Ministry of Health of the People’s Republic of China. China’s Health Statistical Yearbook 2009; Peking Union Medical College Press: Beijing, China, 2010.
- Ministry of Health of the People’s Republic of China. China’s Health Statistical Yearbook 2010; Peking Union Medical College Press: Beijing, China, 2011.
- Ministry of Health of the People’s Republic of China. China’s Health Statistical Yearbook 2011; Peking Union Medical College Press: Beijing, China, 2012.
- Ministry of Health of the People’s Republic of China. China’s Health Statistical Yearbook 2012; Peking Union Medical College Press: Beijing, China, 2013.
- Ministry of Health of the People’s Republic of China. China’s Health Statistical Yearbook 2013; Peking Union Medical College Press: Beijing, China, 2014.
- Araújo, C.; Barros, C.P.; Wanke, P. Efficiency determinants and capacity issues in Brazilian for-profit hospitals. Health Care Manag. Sci. 2014, 17, 126–138. [Google Scholar] [CrossRef] [PubMed]
- Dutta, A.; Bandyopadhyay, S.; Ghose, A. Measurement and determinants of public hospital efficiency in West Bengal, India. J. Asian Public Policy 2014, 7, 231–244. [Google Scholar] [CrossRef]
- Wagstaff, A.; Lindelow, M. Can insurance increase financial risk? The curious case of health insurance in China. J. Health Econ. 2008, 27, 990–1005. [Google Scholar] [CrossRef] [PubMed]
- Wagstaff, A.; Lindelow, M.; Jun, G.; Ling, X.; Juncheng, Q. Extending health insurance to the rural population: An impact evaluation of China’s new cooperative medical scheme. J. Health Econ. 2009, 28, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Jian, T.; Sachs, J.D.; Warner, A.M. Trends in regional inequality in China. China Econ. Rev. 1996, 7, 1–21. [Google Scholar] [CrossRef]
- Simar, L.; Wilson, P.W. Estimation and inference in two-stage, semi-parametric models of production processes. J. Econom. 2007, 136, 31–64. [Google Scholar] [CrossRef]
- Bădin, L.; Daraio, C.; Simar, L. Optimal bandwidth selection for conditional efficiency measures: A data-driven approach. Eur. J. Oper. Res. 2010, 201, 633–640. [Google Scholar] [CrossRef]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chu, K.; Zhang, N.; Chen, Z. The Efficiency and Its Determinants for China’s Medical Care System: Some Policy Implications for Northeast Asia. Sustainability 2015, 7, 14092-14111. https://doi.org/10.3390/su71014092
Chu K, Zhang N, Chen Z. The Efficiency and Its Determinants for China’s Medical Care System: Some Policy Implications for Northeast Asia. Sustainability. 2015; 7(10):14092-14111. https://doi.org/10.3390/su71014092
Chicago/Turabian StyleChu, Kejia, Ning Zhang, and Zhongfei Chen. 2015. "The Efficiency and Its Determinants for China’s Medical Care System: Some Policy Implications for Northeast Asia" Sustainability 7, no. 10: 14092-14111. https://doi.org/10.3390/su71014092