

Background
Ketamine has been available for more than fifty years and has been traditionally utilized more commonly in the pediatric population.1–3 It is a frequently used medication in the emergency department for procedural sedation. Ketamine is accepted as a useful alternative to opiates at sub-dissociative doses for analgesia.4 Its use has grown in the adult population for post-operative pain management and refractory depression.5–7
In recent years, ketamine has been gaining attention as a choice for continuous sedation in patients on mechanical ventilation as it possesses both sedative and analgesic properties and minimal effect on respiratory drive.8 The known adverse effects of the more common sedation agents such as propofol, dexmedetomidine, benzodiazepines, and opiates make alternative agents desirable. Both propofol and dexmedetomidine have well-known adverse side effects of hypotension and can be a cause of initiating vasopressor use.9,10 Dexmedetomidine has a higher incidence of both hypotension and bradycardia when compared to midazolam as sedation for prolonged mechanical ventilation.11 Although unclear whether vasopressors are the direct cause of increased mortality or the disease severity requiring vasopressor use, increased vasopressor requirements have been associated with increased mortality.12–14
Ketamine provides a sympathomimetic response that may be beneficial to patients in shock. In a study of 130 volunteer patients, the results suggested that ketamine may increase the blood pressure during the initial use of continuous infusion, mimicking a vasopressor response.15 Similar results were observed in a smaller study of 20 subjects.1 Other studies in ventilated patients have suggested lower vasopressor needs in patients sedated with ketamine. In a retrospective study examining ventilated patients with continuous infusion of ketamine as an adjunct, 70.5% of patients had a decrease or no vasopressor requirement after 24 hours, once ketamine was initiated.16 Another retrospective study showed a decreased vasopressor requirement at 6 hours post-ketamine, but no difference at 24 hours.17 In a study of patients with septic shock, ketamine was associated with a trend to lower vasopressor need and a reduction in other sedation needed.18 Our study seeks to examine the vasopressor response for a more prolonged period of 48 hours after initiation of ketamine.
Since ketamine is often an adjunct to another sedation agent, we hypothesized that mechanically ventilated patients sedated with a continuous ketamine infusion as a second agent will have a lower vasopressor requirement compared to patients sedated with two alternate drugs. In our study, we chose to compare patients on both propofol and fentanyl infusions (PF-G) to this ketamine group (K-G).
Methods
We performed a retrospective cohort study on adult patients admitted to intensive care units (ICU) in two large academic hospitals in Rhode Island between April 2015 and September 2019. Inclusion criteria were patients greater than 18 years of age undergoing mechanical ventilation. The intervention group included patients on continuous ketamine as an adjunct to another sedative. The control group included patients on simultaneous propofol and fentanyl continuous infusions. We allowed for the same patients to be part of the study if they were readmitted and satisfied the inclusion criteria for the same study group. We excluded patients who were readmitted and met criteria for both study groups during the timeframe. We screened a total of 3322 hospital encounters (2972 patients) between April 2015 and September 2019. Those who satisfied the inclusion criteria for both study groups, 410 hospital encounters (372 patients) were examined further. There were 40 hospital encounters (25 patients) that were readmitted and met criteria for both study groups during the timeframe; these encounters were excluded. Of the 370 hospital encounters (347 patients), we randomly selected 291 hospital encounters (274 patients) for analysis. Of 291 hospital encounters, 86 hospital encounters (82 patients) were excluded because these patients did not satisfy inclusion criteria upon chart review (Figure 1). Our study was approved by the Institutional Review Board (1373059-1) and informed consent was waived.

Baseline characteristics obtained were age, gender, weight (kilograms), race (White/Caucasian, Black/African American, others), and primary diagnoses. Height and weight were collected to calculate body mass index (BMI).19 Glasgow coma scale (GCS) assessed for consciousness.20 The Confusion assessment method for intensive care unit (CAM-ICU) score assessed for delirium on arrival to the ICU, as well as before and after sedation.21 The Acute Physiology and Chronic Health Evaluation II (APACHE II score) and Charlson Comorbidity index (CCI) were measured to predict risk of mortality.22,23
Outcome measures
The primary outcome was defined as the dose of norepinephrine up to 12 hours before and 48 hours after the initiation of either ketamine for the intervention group, or the initiation of both propofol and fentanyl for the control group. We defined this initiation point as time 0 hour. The hourly doses of norepinephrine within this timeframe were recorded. An analysis was performed to calculate the average doses in 12-hour blocks, up to 12 hours before and 48 hours after time 0 hour. Blood pressure targets were not protocolized, however a minimum mean arterial pressure (MAP) of 65 mmHg was most often clinically targeted.
Our secondary outcomes include mortality, ICU length-of-stay (LOS), hospital LOS, ventilator-free days within 28 days, and overall concomitant sedative continuous infusions including dexmedetomidine, propofol, fentanyl, and midazolam. Mortality rates were categorized to all-cause, 30-day, ICU, and in-hospital. All-cause mortality was defined as death from any cause up to 6 months after discharge. Proportion of patients on other sedatives, such as dexmedetomidine and midazolam, was calculated within K-G and PF-G groups. Ventilator-free days were defined based on days off the ventilator within 28 days. Patients on the ventilator for more than 28 days were considered to have 0 ventilator-free days.
Statistical Analysis
Study data were collected and managed using REDCap electronic data capture tools.24,25 REDCap (Research Electronic Data Capture) is a secure, web-based software platform designed to support data capture for research studies,
The analysis was conducted in SAS© software (Version 9.4, SAS Institute Inc., Cary, NC), where chi-square and Student’s t-tests were performed for descriptive analyses to report and compare the study groups on demographics, norepinephrine dose (12 hours before, and up to 48 hours after time 0), average norepinephrine dose usage by hour, mortality, concomitant sedative medications, LOS, and ventilator-free days.26
Results
The final analytical sample had 205 hospital encounters (200 patients), 102 (49.8%) hospital encounters (100 patients) in the intervention group, 103 (50.2%) hospital encounters (100 patients) in the control group.
The intervention group had fewer Black/African American patients (6.3%) compared to the control group (19.6%) (p-value= 0.0155). The average age for the intervention group was 48.6 years (with standard deviation (SD)=16.1) and the control group was 48.5 years (SD=15.5) (p-value=0.9910). The average APACHE II score (16.9 and SD=7.1) and CCI (1.0 and SD=1.3) were comparable between the two groups (p-value=0.9853 and 0.2057, respectively). The weight and the BMI were similar between the two study groups, with the averages of 83.1 kg (SD=27.5) and 29.2 kg/m2 (SD=9.5) (p-value= 0.1024 and 0.2744, respectively). The proportion of patients with positive CAM-ICU on arrival to ICU was similar in the two study groups, with an overall proportion of 90.5 (p-value=0.8629) (Table 1). For the primary diagnosis of trauma or surgery, ketamine was not utilized in any patients in the K-G (p-values= <0.0001 and 0.0016, respectively). For patients with the primary diagnosis of asthma, there were 6.9% in the K-G compared to 0% in the PF-G (p-value=0.0068) (Table 1).
There was no statistically significant difference with the incidence of midazolam (32.4% compared to 42.7%, p-value=0.1255) or dexmedetomidine use (66.7% compared to 57.3%, p-value=0.1664) between the intervention and control group, respectively (Table 2).
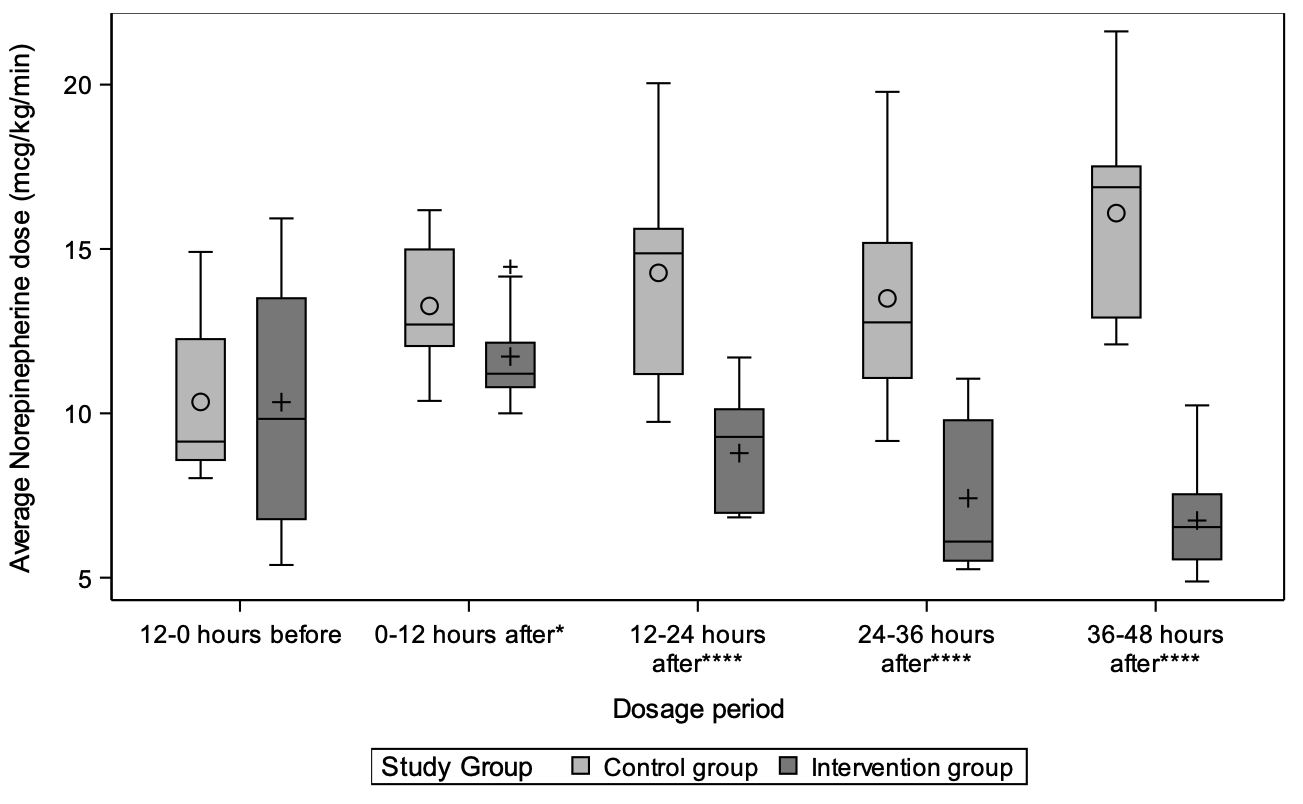
For the primary outcome, there were reduced vasopressor requirements as measured by norepinephrine doses in K-G versus PF-G after ketamine initiation. Up to 12 hours prior to time 0 hour, the average norepinephrine dose was similar between K-G and PF-G, 10.3 mcg/kg/min vs 10.3 mcg/kg/min (p-value=0.9962). The average dose of norepinephrine was lower up to 48 hours after the initiation of ketamine (K-G) compared to PF-G, 8.7 mcg/kg/min vs 14.2 mcg/kg/min (p-value=<0.0001) (Table 3). This associated reduction in average norepinephrine dose was consistent when looking at the time intervals of 12 hours (11.7 mcg/kg/min vs 13.3 mcg/kg/min, p-value=0.0267), 13-24 hours (8.8 mcg/kg/min vs 14.3 mcg/kg/min, p-value=<0.0001), 25-36 hours (7.4 mcg/kg/min vs 13.5 mcg/kg/min, p-value=<0.0001), and 37-48 hours (6.7 mcg/kg/min vs 16.1 mcg/kg/min, p-value=<0.001) (Table 3, Figure 2) after time 0 hour. Figure 3 shows the average dose of norepinephrine hourly, starting 12 hours before and 48 hours after the initiation of ketamine or propofol/fentanyl.

There was no associated difference in all-cause mortality, 30-day mortality, in-hospital mortality, ICU mortality, ICU LOS, and ventilator-free days between the K-G and PF-G (Table 4). The all-cause, 30-day, ICU, and in-hospital mortality rates were similar in both groups (with overall rates of 32.2%, 21.5%, 22%, 23.9%, p-value=0.8019, 0.9709, 0.8952, 0.8392, respectively). Overall average ICU and hospital LOS were 8.8 days (p-value=0.5174) and 16.6 days (p-value=0.9280), respectively. The average ventilator free days was 23.0 (SD=5.3) (p-value=0.5667).

Discussion
Ketamine has a long history of clinical use and its application is steadily widening due to ongoing challenges with sedation in patients that do not respond to conventional therapy or have side effects with standard drug regimens. As a drug with sedative and analgesic properties and a favorable hemodynamic profile, the potential physiological benefits of ketamine in critically-ill patients undergoing mechanical ventilation may be under-appreciated. According to animal studies, the mechanism of increased sympathetic response of ketamine may be related to the tissue release of catecholamine stores. Chang et al. demonstrated in rats that the increased blood pressure effect by ketamine was blunted by pretreatment with reserpine, which depletes tissues catecholamines.27
We observed a persistent decrease in average norepinephrine doses up to 48 hours after the initiation of ketamine as compared to patients who received fentanyl and propofol. We categorized the average doses based on different time intervals and the reduction in average doses was consistent. Previous studies reported effects of this vasopressor response up to 24 hours, our findings show a longer effect up to 48 hours.16,17 This prolonged effect suggests there may be additional mechanisms to this vasopressor response besides release of tissue catecholamines. There may be a direct vasoconstrictive effect increasing systemic vascular resistance (SVR).
The benefits of ketamine in mechanically-ventilated patients may extend beyond the sympathomimetic properties. Although not yet studied in a randomized trial, the bronchodilatory properties and improvement of dynamic compliance have led many clinicians to consider and use ketamine infusions in asthmatic patients.28 To our knowledge, no clear dose or duration of ketamine-related bronchodilation have been published. A study by Heshmati et al. examined asthmatic patients who did not respond to traditional therapy and on mechanical ventilation after 24 hours, the addition of continuous ketamine infusion for two hours demonstrated a decreased mean peak airway pressure and arterial CO2.29 This perceived benefit may have affected the use of ketamine in our patient groups as we found that all patients with the primary diagnosis of asthma were observed to be managed with continuous ketamine infusion.
However, ketamine may not be suitable for all intubated patients and especially those with heart failure. Animal models have shown dose-related myocardial depression, with higher doses correlating with lower cardiac output.27 A randomized study revealed a decrease in cardiac index with ketamine in patients with reduced left ventricular function in the first 24 hours. Pulmonary capillary wedge pressure and mean pulmonary artery pressure were elevated as well. The SVR was higher in the ketamine group. It remains unclear if this is the effect of direct suppression of the myocardium or the result of the increased afterload.30
There are several limitations to our study. The first is the nature of its retrospective design. We found an associated decrease in vasopressor use, however this does not prove that the reduced vasopressor dose was caused by the ketamine use. These results should be considered hypothesis-generating. Second, finding a control group to match the study group was a challenge, as ketamine can be used with any number or combination of sedation agents. We chose two sedation agents that were commonly used clinically, however the 2 groups were likely managed quite differently from one another. We also did not specifically examine the sedating agents used during intubation which may have affected the initial blood pressures and vasopressor needs.
As stated earlier, asthmatic patients had markedly more use of ketamine and it can also be observed that ketamine was not used at all in the trauma and surgical patients in this study. The perceived cardiopulmonary benefits of ketamine on asthma patients likely led to more asthma patients receiving ketamine and may have skewed the overall results to favor the ketamine group. While a MAP of 65 mmHg was most often used in our institutions, there was no standardized blood pressure target in this study adding provider-related variation with this. Also, multiple vasopressors may have been used but we examined norepinephrine specifically as it is the predominant vasopressor used at our institution. Use of other vasopressors was not accounted for in this study.
Conclusion
In our retrospective study, we demonstrated the use of ketamine as an adjunct for sedation in mechanically ventilated patients was associated with decreased vasopressor requirements when compared to a common sedation regimen of propofol and fentanyl. Further research with multicenter, randomized, placebo-controlled trials are required to better define the role of ketamine as an adjunct sedation agent for critically-ill patients on mechanical ventilation.
Funding Information
The authors declare that they have no competing interests or source of funding.
Acknowledgement
N/A
Corresponding author
Gerardo Carino MD, PhD
Associate Professor of Medicine, Clinician Educator
Division of Pulmonary, Critical Care and Sleep Medicine
Warren Alpert Medical School at Brown University,
164 Summit Avenue, Providence, RI, 02906, USA
Tel: 401-793-4501
Fax: 401-793-4511
Email: Gerardo_Carino@brown.edu