
Abstract
Background
Although the incidence of gastric cancer has been decreasing, recent reports suggest an increased rate in select populations. We sought to evaluate trends in gastric cancer incidence to identify high-risk populations.
Methods
Gastric cancer incidence rates from 1992 to 2011 were computed with use of the Surveillance, Epidemiology, and End Results (SEER) registry. We evaluated trends in incidence rates by calculating the annual percent change (APC) across three age groups (20–49 years, 50–64 years, and 65 years or older) and four racial/ethnic groups (Hispanics, non-Hispanic whites, blacks, and Asian/Pacific Islanders).
Results
We identified 41,428 patients with gastric cancer. For the entire cohort during the study period, the APC was decreased. When patients were grouped according to sex, the APC was flat or decreased in women regardless of age or race/ethnicity. The APC was also flat or decreased for all men except young Hispanic men (20–49 years), who had an increased APC of nearly 1.6 % (1.55 %, 95 % confidence interval 0.26–2.86 %). Furthermore, young Hispanic men were the only group to have increased incidence of stage IV disease (APC 4.34 %, 95 % confidence interval 2.76–5.94 %) and poorly differentiated tumors (APC 2.08 %, 95 % confidence interval 0.48–3.70 %).
Conclusions
The APC of the incidence of gastric cancer in young Hispanic men places it among the top cancers with rising incidence in the USA. This is concomitant with increased incidence of advanced disease at presentation. This major public health concern warrants additional research to determine the cause of the increasing incidence in this group.
Similar content being viewed by others

Introduction
Gastric cancer remains a leading cause of cancer-related death worldwide [1]. Although incidence rates of gastric cancer are decreasing in the general population [1], reporting these trends fails to identify subpopulations of patients who are at increased risk of developing disease. Although it is well known that certain racial/ethnic [1–3] and age [4] groups have a greater propensity to develop this disease, there are few data pertaining to whether the incidence rates have increased for these susceptible groups. Furthermore, our own anecdotal experience suggested a greater number of young patients with gastric cancer.
Gastric cancer in young (younger than 45 years) individuals typically represents less than 10 % of new cases [5–8]. Although its occurrence in this population is uncommon, the impact is significant in these often productive members of society [9, 10]. Factors that explain the occurrence of the disease specifically in young patients are sparse. Although genetic differences have been strongly implicated [11–13], the cause of this phenomenon is likely to be multifactorial, with contributions from factors such as diet, exposure to toxins and infectious agents [14, 15].
A deeper understanding of trends in gastric cancer incidence in subpopulations, such as the young, may make possible the design of screening programs or other intervention measures to allow the reversal of the effects of potentially modifiable risk factors such as high-salt diet or treatment of Helicobacter pylori. Furthermore, earlier detection may positively impact patient outcomes through potentially curative surgery. To further investigate our anecdotal experience, we sought to evaluate recent trends in gastric cancer incidence to identify high-risk populations.
Patients and methods
Patient selection
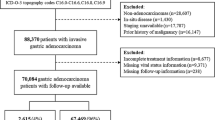
Cancer incidence data were obtained from the US National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) Program. We selected the SEER 13 research dataset as its race/ethnicity information is more specific than the SEER 9 data. The dataset comprises data from 13 SEER sites covering approximately 13.4 % of the US population (based on the 2010 census), and currently contains incidence and population data from 1992 to 2011 [16]. We selected adults aged 20 years or older who had histologically confirmed gastric carcinoma (codes 8000–8152, 8154–8231, 8243–8245, 8247–8248, 8250–8576, 8940–8950, and 8980–8990) as defined by the American Joint Committee on Cancer Collaborative Staging schema version 02.04 [17]. Because of small sample sizes within strata, we excluded the Alaska Natives Registry patients (n = 534) as well as patients with race/ethnicity coded as non-white Hispanics (n = 167) or unknown (n = 94). The stepwise selection criteria are summarized in the electronic supplementary material. Our final dataset consisted of 41,428 patients.
Statistical analysis
Temporal trends in gastric cancer incidence were summarized with use of the annual percent change (APC) statistic, which measures the change in incidence rates over each year of the study period. We calculated APCs by fitting a least squares regression line to the natural logarithm of the rates, using calendar year as the regressor variable [18]. To examine if APCs were significantly increased or decreased over time, Tiwari-modified 95 % confidence intervals (CIs) were estimated [19]. CIs not containing 0 (i.e., no change over time) were considered statistically significant, with a two-sided alpha of 0.05. We also verified temporal trends using joinpoint analyses; however, the main results did not change [20]. In addition to overall trends, trends after stratification of patients by sex, age group (20–49 years, 50–64 years, and 65 years or older), and race/ethnicity (Hispanics, non-Hispanic whites, blacks, and Asian/Pacific Islanders) were assessed. Temporal trends in clinical characteristics, including American Joint Committee on Cancer stage, grade, tumor location, and geographical region were also examined. Patients in the Northern Plains and Southwest areas were excluded from the analysis as there were no cases in some years, which prevented accurate analysis of temporal trends.
All analyses were performed with both SAS (SAS Institute, Cary, NC, USA) and SEER*Stat v8.15 (released March 31, 2014) for internal validation. SEER 13 public use data from 1992 to 2011 were obtained from the SEER website (April 2013 release) and were based on the November 2012 submission [16]. The US population data were also obtained from SEER [21]. Institutional review board approval was not required as this study used publically available deidentified data.
Results
Characteristics of the entire cohort
We identified 41,428 patients with gastric cancer (23,095 men, 55.7 %; 18,333 women, 44.3 %). Patient demographic and disease characteristics are summarized in Table 1. Whites composed the largest group (45.2 %) of the gastric cancer cohort, and gastric cancer was commonest in the older groups (65 years or older, 68.9 %). Most of the patients with gastric cancer were men (55.7 %) and geographically located on the Pacific coast (62.2 %). In general, most of the patients (84.4 %) had no history of cancer, and the greatest proportion of tumors were located distally (31.8 %) and were poorly differentiated (56.1 %). Most patients had advanced disease at presentation (stage III, 22.0 %; stage IV, 31.2 %).
Trends in annual percent change in gastric cancer incidence
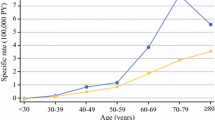
General trends in gastric cancer incidence are illustrated in Fig. 1. For the entire cohort, we observed that the APC in gastric cancer incidence significantly decreased during the study period (APC −2.23 %, 95 % CI −2.43 to −2.04 %) (Fig. 1a). When patients were categorized according to sex, the APC significantly decreased in both men (APC −2.72 %, 95 % CI −2.97 to −2.46 %) and women (APC −1.83 %, 95 % CI −2.07 to −1.58 %) (Fig. 1b). When analyzed by age group, the APC significantly decreased in patients aged 50–64 years (APC −2.28 %, 95 % CI −2.64 to −1.91) and 65 years or older (APC −2.56 %, 95 % CI −2.80 to −2.31) and was not significantly changed in those aged 20–49 years (Fig. 1c). When analyzed by race/ethnicity, all groups demonstrated a significantly decreased APC in gastric cancer incidence during the study period (Fig. 1d).

Trends in gastric cancer incidence from 1992 to 2011 in the entire cohort (a) and categorized by sex (b), age group (c), and race/ethnicity (d). Three asterisks a significant decreasing trend (p < 0.001) compared with the baseline, APC annual percent change, API Asian/Pacific Islanders
Stratification by both race/ethnicity and sex
We then analyzed the cohort according to race and sex (Table 2). In women the APC in gastric cancer incidence was flat or decreased in all racial/ethnic and age groups. The APC was also flat or decreased for men of all racial/ethnic and age groups except for young Hispanic men (age 20–49 years), in which there was a significant increase in the APC of nearly 1.6 % (APC 1.55 %, 95 % CI 0.26–2.86 %).
Trends in demographic and disease-related variables
We then analyzed temporal trends in patient demographic and disease-related variables in all racial/ethnic groups within the young male cohort (Table 3) and also compared young Hispanic men with their older counterparts (Table 4). Young Hispanic men were the only group to have significantly increased incidence of stage IV disease (APC 4.34 %, 95 % CI 2.76–5.94 %) and poorly differentiated tumors (APC 2.08 %, 95 % CI 0.48–3.70 %). Furthermore, a significantly increased incidence was observed in young Hispanic men from the Pacific coast compared with other geographical regions (APC 1.48 %, 95 % CI 0.12–2.86) and also in tumor location that was “not otherwise specified” compared with other tumor locations (APC 5.07 %, 95 % CI 1.04–9.26). Figure 2 illustrates the trends in gastric cancer incidence in young Hispanic men by stage, grade, tumor location, and geographical region.

Trends in gastric cancer incidence from 1992 to 2011 in young Hispanic men by stage (a), grade (b), tumor location (c), and geographical region (d). APC annual percent change, NOS not otherwise specified, Undiff undifferentiated, Unk unknown, three daggers denotes significant increasing trend (p < 0.001), one dagger denotes significant increasing trend (p < 0.05) compared to baseline
Discussion
Marked disparities in gastric cancer incidence exist [1]. A recent study by Lui et al. [2] demonstrated that Asians had the highest incidence of gastric cancer; however, remarkably high rates were also noted in the black and Hispanic populations. Despite the relatively high rates of gastric cancer in select racial/ethnic groups, there has been a general decline in the overall incidence of gastric cancer in the USA during the last several decades. On the basis of clinical suspicion, we examined gastric cancer in younger patients and observed a consistent increase in gastric cancer incidence limited to young Hispanic men. Our results also highlight another worrisome feature of these young Hispanic men frequently presenting with advanced or metastatic disease.
In young Hispanic men, the APC of gastric cancer places it in the top tier of cancers with rising incidence in the USA, including melanoma, liver cancer, and breast cancer [1]. Furthermore, gastric cancer remains common throughout Mexico, Central America, and South America [3] and mortality associated with this cancer is significantly higher in Latin America than it is in North America [22]. The rising incidence of gastric cancer in this population is perplexing and the exact cause is unknown. Several theories are worthy of discussion. First, it is feasible that increased rates of seropositivity of H. pylori infection, an established risk factor for the development of gastric cancer [23], may contribute to the rise in this young population. The rates of H. pylori seropositivity are higher in Mexican Americans than in non-Hispanic whites, and there is an especially high incidence in youth and early adulthood [24]. However, infection prevalence is higher among foreign-born than US-born Hispanics [25], and in our current study we were unable to determine whether the Hispanics with gastric cancer were foreign born. Second, it is possible that increased salt intake [26] may contribute to increased incidence of gastric cancer in this population. Obesity has been associated with the development of various cancers of the gastrointestinal tract, including gastric cancer [27], and with obesity rates rising in the young [28], this may increase the incidence of gastric cancer. Third, genetic susceptibility also merits consideration as a recent case–control study identified the presence of certain single nucleotide polymorphisms as loci for susceptibility to gastric cancer in Hispanic Americans [29]. Finally, differences in tumor biology may also be implicated as Hispanics have previously been shown to have increased incidence of mucinous/signet ring cell histologic type, involvement of the whole stomach, and peritoneal dissemination [30].
The alarming increase in the APC is concomitant with increased incidence of advanced disease at presentation. A number of studies have reported more advanced disease presentation in young populations. For example, Theuer et al. [7] demonstrated that patients with gastric cancer younger than 40 years were likelier to have distant metastases, signet ring cell histologic type, and higher grade. Smith and Stabile [31] also showed that young patients with gastric cancer were likelier to have diffuse histologic type, adjacent organ invasion, and nodal and distant metastases. Interestingly, the advanced disease at presentation may not necessarily result in poorer outcomes. Al-Refaie et al. [5] stratified young and older patients for the stage at presentation and observed that survival outcomes were more favorable in the younger patients.
There may be straightforward explanations for the trend toward more advanced disease in the young Hispanic cohort. Patients and their health care providers may not necessarily consider malignant causes when symptoms arise. Less access to health care as a result of low socioeconomic status may also contribute, although some studies suggest that disparities persist even when socioeconomic status and health care access are similar [32]. With the overall declining incidence of gastric cancer in the USA [1] there is likely little incentive to establish education and screening programs in the younger population,and thus the presentation of advanced disease in this population may continue.
Our study results show that this major public health concern warrants additional research to determine methods of early disease detection in this group. For example, in Japan and Korea, where the incidence of gastric cancer far surpasses that in the USA, a variety of screening strategies have been proposed [33–35], ranging from noninvasive tests to invasive tests [35]. A common strategy in both Korea and Japan involves mass endoscopic screening of men and women aged 40 years or older [35]. Other common strategies include screening for H. pylori and endoscopic surveillance [36]. A strategy based on individual risk and background incidence of gastric cancer may be sensible for young Hispanic men in the USA, including early eradication of H. pylori [37].
Although the incidence of gastric cancer in young Hispanics is low compared with that in other groups, there remains the potential for significant impact. Between 2000 and 2010 the Hispanic population grew by 43 %, thus constituting 16 % of the total population of the USA [38]. This dramatic and continued rise in the Hispanic population paired with the higher incidence of gastric cancer in Hispanics [39, 40] makes gastric cancer a nationwide disparity that warrants further investigation and understanding, particularly in high-risk subsets of the population.
There are several limitations to our study. The data come from a retrospective database and are subject to coding error; furthermore, the registry itself captures only a limited percentage of the population. Hispanic ethnicity is captured primarily on medical record review of the surname, which can be misleading. Because of missing data, we were unable to determine whether the rising incidence of gastric cancer occurred in Hispanic men who were born the in the USA versus elsewhere. One final consideration is that of whether the true Hispanic population is underestimated in US Census data because of the rising numbers of undocumented individuals, which has the potential to overinflate the incidence of gastric cancer in this population.
To our knowledge, this is the first study to demonstrate that the rise in gastric cancer incidence in the Hispanic population is limited to young men, with other groups showing either no change or decreasing incidence. A priority for this major heath concern is the need to promote awareness among the Hispanic population and their health care providers. Heightened awareness and the use of appropriate screening programs may result in the ability to capture disease at an earlier stage, with the potential to better impact disease outcomes.
References
Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA Cancer J Clin. 2014;64(1):9–29.
Lui FH, Tuan B, Swenson SL, Wong RJ. Ethnic disparities in gastric cancer incidence and survival in the USA: an updated analysis of 1992–2009 SEER data. Dig Dis Sci. 2014;59:3027–34.
Siegel RL, Fedewa SA, Miller KD, Goding-Sauer A, Pinheiro PS, Martinez-Tyson D, et al. Cancer statistics for Hispanics/Latinos, 2015. CA Cancer J Clin. 2015;65(6):457–80.
Anderson WF, Camargo MC, Fraumeni JF Jr, Correa P, Rosenberg PS, Rabkin CS. Age-specific trends in incidence of noncardia gastric cancer in US adults. J Am Med Assoc. 2010;303(17):1723–8.
Al-Refaie WB, Hu CY, Pisters PW, Chang GJ. Gastric adenocarcinoma in young patients: a population-based appraisal. Ann Surg Oncol. 2011;18(10):2800–7.
Theuer CP, de Virgilio C, Keese G, French S, Arnell T, Tolmos J, et al. Gastric adenocarcinoma in patients 40 years of age or younger. Am J Surg. 1996;172(5):473–6; discussion 476–7.
Theuer CP, Kurosaki T, Taylor TH, Anton-Culver H. Unique features of gastric carcinoma in the young: a population-based analysis. Cancer. 1998;83(1):25–33.
Kim DY, Ryu SY, Kim YJ, Kim SK. Clinicopathological characteristics of gastric carcinoma in young patients. Langenbecks Arch Surg. 2003;388(4):245–9.
Doukkali EB, Winterling J, Eriksson LE, Lampic C, Hagstrom AS, Wettergren L. Adolescents’ and young adults’ experiences of childhood cancer: descriptions of daily life 5 years after diagnosis. Cancer Nurs. 2013;36(5):400–7.
Hauken MA, Larsen TM, Holsen I. Meeting reality: young adult cancer survivors’ experiences of reentering everyday life after cancer treatment. Cancer Nurs. 2013;36(5):E17–26.
Buffart TE, Carvalho B, Hopmans E, Brehm V, Kranenbarg EK, Schaaij-Visser TB, et al. Gastric cancers in young and elderly patients show different genomic profiles. J Pathol. 2007;211(1):45–51.
Carvalho R, Milne AN, van Rees BP, Caspers E, Cirnes L, Figueiredo C, et al. Early-onset gastric carcinomas display molecular characteristics distinct from gastric carcinomas occurring at a later age. J Pathol. 2004;204(1):75–83.
Schildberg CW, Abba M, Merkel S, Agaimy A, Dimmler A, Schlabrakowski A, et al. Gastric cancer patients less than 50 years of age exhibit significant downregulation of E-cadherin and CDX2 compared to older reference populations. Adv Med Sci. 2014;59(1):142–6.
Pasechnikov V, Chukov S, Fedorov E, Kikuste I, Leja M. Gastric cancer: prevention, screening and early diagnosis. World J Gastroenterol. 2014;20(38):13842–62.
Milne AN, Sitarz R, Carvalho R, Carneiro F, Offerhaus GJ. Early onset gastric cancer: on the road to unraveling gastric carcinogenesis. Curr Mol Med. 2007;7(1):15–28.
Surveillance, Epidemiology, and End Results (SEER) program November 2013:[SEER*Stat Database: Incidence—SEER 13 Regs Research Data, Nov 2013 Sub (1992–2011) <Katrina/rita population adjustment>—linked to county attributes—total US, 1969–2012 counties, National Cancer Institute, DCCPS, Surveillance Research Program, surveillance systems branch, released April 4, based on the November 3 submission]. http://seer.cancer.gov. Accessed 1 Dec 2014.
American Joint Committee on Cancer. Collaborative stage data collection system. https://cancerstaging.org/cstage/schema/Pages/version0204.aspx. Accessed 1 Dec 2014.
Kleinbaum DG, Muller KE. Applied regression analysis and other multivariable methods. 2nd ed. Boston: PWS-Kent; 1988.
Tiwari RC, Clegg LX, Zou Z. Efficient interval estimation for age-adjusted cancer rates. Stat Methods Med Res. 2006;15(6):547–69.
Kim HJ, Fay MP, Feuer EJ, Midthune DN. Permutation tests for joinpoint regression with applications to cancer rates. Stat Med. 2000;19(3):335–51.
Surveillance, Epidemiology, and End Results (SEER) program October 2012: [SEER*Stat Database: Populations—total US (1950–2011) <Katrina/Rita Adjustment>, National Cancer Institute, DCCPS, surveillance research program, surveillance systems branch, released October 2.]. http://seer.cancer.gov. Accessed 1 Dec 2014.
Chatenoud L, Bertuccio P, Bosetti C, Malvezzi M, Levi F, Negri E, et al. Trends in mortality from major cancers in the Americas: 1980–2010. Ann Oncol. 2014;25(9):1843–53.
Loffeld RJ, Willems I, Flendrig JA, Arends JW. Helicobacter pylori and gastric carcinoma. Histopathology. 1990;17(6):537–41.
Grad YH, Lipsitch M, Aiello AE. Secular trends in Helicobacter pylori seroprevalence in adults in the United States: evidence for sustained race/ethnic disparities. Am J Epidemiol. 2012;175(1):54–9.
Tsai CJ, Perry S, Sanchez L, Parsonnet J. Helicobacter pylori infection in different generations of Hispanics in the San Francisco Bay Area. Am J Epidemiol. 2005;162(4):351–7.
Briefel RR, Johnson CL. Secular trends in dietary intake in the United States. Annu Rev Nutr. 2004;24:401–31.
Aleman JO, Eusebi LH, Ricciardiello L, Patidar K, Sanyal AJ, Holt PR. Mechanisms of obesity-induced gastrointestinal neoplasia. Gastroenterology. 2014;146(2):357–73.
Lifshitz F, Lifshitz JZ. Globesity: the root causes of the obesity epidemic in the USA and now worldwide. Pediatr Endocrinol Rev. 2014;12(1):17–34.
Sun Y, Gu J, Ajani JA, Chang DW, Wu X, Stroehlein JR. Genetic and intermediate phenotypic susceptibility markers of gastric cancer in Hispanic Americans: a case-control study. Cancer. 2014;120(19):3040–8.
Yao JC, Tseng JF, Worah S, Hess KR, Mansfield PF, Crane CH, et al. Clinicopathologic behavior of gastric adenocarcinoma in Hispanic patients: analysis of a single institution’s experience over 15 years. J Clin Oncol. 2005;23(13):3094–103.
Smith BR, Stabile BE. Extreme aggressiveness and lethality of gastric adenocarcinoma in the very young. Arch Surg. 2009;144(6):506–10.
Halpern MT, Ward EM, Pavluck AL, Schrag NM, Bian J, Chen AY. Association of insurance status and ethnicity with cancer stage at diagnosis for 12 cancer sites: a retrospective analysis. Lancet Oncol. 2008;9(3):222–31.
Asaka M, Kato M, Graham DY. Strategy for eliminating gastric cancer in Japan. Helicobacter. 2010;15(6):486–90.
Graham DY, Asaka M. Eradication of gastric cancer and more efficient gastric cancer surveillance in Japan: two peas in a pod. J Gastroenterol. 2010;45(1):1–8.
Lin JT. Screening of gastric cancer: who, when, and how. Clin Gastroenterol Hepatol. 2014;12(1):135–8.
Asaka M, Kato M, Sakamoto N. Roadmap to eliminate gastric cancer with Helicobacter pylori eradication and consecutive surveillance in Japan. J Gastroenterol. 2014;49(1):1–8.
Ma JL, Zhang L, Brown LM, Li JY, Shen L, Pan KF, et al. Fifteen-year effects of Helicobacter pylori, garlic, and vitamin treatments on gastric cancer incidence and mortality. J Natl Cancer Inst. 2012;104(6):488–92.
United States Census Bureau. Overview of race and Hispanic origin. 2010. http://www.census.gov/prod/cen2010/briefs/c2010br-02.pdf. Accessed 4 Nov 2014.
Carozza SE, Howe HL. Patterns of cancer incidence among US Hispanics/Latinos, 1995–2000. Cancer Causes Control. 2006;17(8):1067–75.
Pinheiro PS, Sherman RL, Trapido EJ, Fleming LE, Huang Y, Gomez-Marin O, et al. Cancer incidence in first generation U.S. Hispanics: Cubans, Mexicans, Puerto Ricans, and new Latinos. Cancer Epidemiol Biomark Prev. 2009;18(8):2162–9.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical standards
This article does not contain any studies with human or animal subjects performed by any of the authors.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Merchant, S.J., Kim, J., Choi, A.H. et al. A rising trend in the incidence of advanced gastric cancer in young Hispanic men. Gastric Cancer 20, 226–234 (2017). https://doi.org/10.1007/s10120-016-0603-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10120-016-0603-7