Background
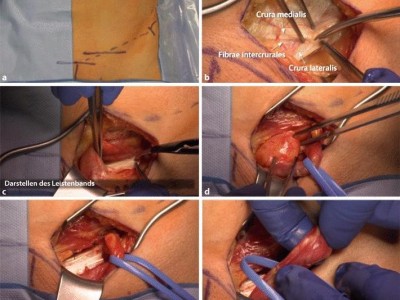
The extralevator abdominoperineal excision (ELAPE) procedure creates an extensive soft tissue defect of the pelvic floor. It has been suggested that primary reconstruction reduces the risk of wound infection and delayed wound healing in this high-risk area. Use of myocutaneous flaps or omentoplasty are associated with functional limitations and complications. We performed the perineal variant of the lotus petal flap, which was originally described for vulvar reconstruction. We aimed to verify if application of the lotus petal flap in pelvic floor reconstruction after ELAPE meets the goals of an ideal reconstruction.
Methods
We performed a retrospective study of 28 patients who underwent the lotus petal flap procedure for pelvic floor reconstruction after ELAPE between January 2011 and March 2014.
Results
Median age was 62.1 years and 78.6 % of patients were female. In most patients the tumor was preoperatively irradiated (89.3 %) and in 28.6 % of the reconstructions a biological mesh was applied. No total flap loss occurred. Six (21.4 %) patients had no complications, while 13 (46.4 %) patients had minor complications (Clavien–Dindo grade I–II). Reoperation (Clavien–Dindo grade IIIb) was performed in nine patients (32.1 %), three of whom required a second lotus petal flap reconstruction. Median time until wound healing was 14 weeks. No additional surgery was performed for aesthetic problems.
Conclusions
Reconstruction of the pelvic floor after ELAPE using the fasciocutaneous lotus petal flap has limited major complications, but still with a high incidence of minor wound complications. This retrospective cohort study shows limited consequences on form and function.