Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Introduction
Obturator neuralgia following mid-urethral sling is rare and most commonly associated with transobturator tapes [1]. Prior reports of obturator nerve injury from retropubic midurethral tape (or tension-free vaginal tape, TVT) have described leaving the portion of tape attached to the nerve in situ [2, 3]. We present a case of obturator neuralgia secondary to lateral retropubic tape misplacement. A multi-disciplinary approach resulted in complete tape removal.
Case study
A 53-year-old woman had been referred to Urogynecology with right groin pain following TVT insertion 18 months earlier. She had had a previous diagnosis of fibromyalgia. She reported sharp right-sided groin pain, starting immediately on waking post-operatively. The pain radiated down her medial thigh and was exacerbated by walking. She was initially managed locally by orthopaedic and pain clinics, with neuropathic pain medications, CT-guided steroid injection to the obturator nerve and psychology input. MRI failed to show scarring in a location that might suggest tape misplacement. Following tertiary centre referral for unsuccessful conservative management of persistent pain (with no improvement in stress incontinence), her case was discussed at our multi-disciplinary team meeting and the patient offered laparoscopic TVT removal. Following dissection and division of the vaginal portion of the tape, the left intra-abdominal arm was found and removed; the right arm was not easily identified. Traction on the proximal portion of the mesh revealed that it passed through the internal obturator muscle, attached to the obturator nerve posteriorly and ended close to the external iliac vessels (Fig. 1). The mesh was carefully dissected from the epineurium of the obturator nerve (Fig. 2) with guidance from a plastic surgeon. Fascicular integrity was confirmed intra-operatively. The mesh was then completely removed (Fig. 3). At 2 months post-operatively, the patient had complete resolution of right-sided groin pain, no muscle weakness and an overall improvement in stress incontinence. The tape was an Ethicon polypropylene standard type 1 TVT mesh.
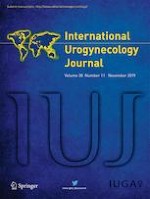
Fig. 1
Intra-operative laparoscopic image following initial dissection. Tension-free vaginal tape (TVT) had been divided vaginally and the vaginal portion passed into the peritoneal cavity (A); traction on this portion demonstrated the path of the mesh. Proximity and attachment to the obturator nerve and neurovascular bundle (B) were noted and a plastic surgeon gave advice. The distal portion of the right TVT was adherent to the pelvic side wall (C) in close proximity to the external iliac vessels (D)
Fig. 2
Cautious sharp and blunt dissection in close proximity to the TVT allowed the tape to be removed from the a posterior and b, c lateral surfaces of the obturator nerve
Fig. 3
a, b Following direct dissection from the obturator nerve, the final portion of the mesh was completely removed from the internal obturator muscle and pelvic side wall. c Obturator nerve integrity was confirmed intra-operatively by a plastic surgeon
×
×
×
Anzeige
Conclusion
During retropubic mid-urethral sling insertion, care should be taken not to advance the mesh laterally. In patients suffering from post-operative obturator neuralgia, malpositioning of the tape should be considered, although it is challenging to diagnose pre-operatively.
Compliance with ethical standards
Conflicts of interest
None.
Consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Mit e.Med Gynäkologie erhalten Sie Zugang zu CME-Fortbildungen der beiden Fachgebiete, den Premium-Inhalten der Fachzeitschriften, inklusive einer gedruckten gynäkologischen oder urologischen Zeitschrift Ihrer Wahl.
Die Hybrid-DRG-Verordnung soll dazu führen, dass mehr chirurgische Eingriffe ambulant durchgeführt werden, wie es in anderen Ländern schon länger üblich ist. Die gleiche Vergütung im ambulanten und stationären Sektor hatten Niedergelassene schon lange gefordert. Aber die Umsetzung bereitet ihnen doch Kopfzerbrechen.
Patienten, die von Ärztinnen behandelt werden, dürfen offenbar auf bessere Therapieergebnisse hoffen als Patienten von Ärzten. Besonders gilt das offenbar für weibliche Kranke, wie eine Studie zeigt.
Frauen mit Belastungsinkontinenz oder Organprolaps sind nach einer Netz-Operation keineswegs beschwerdefrei. Vielmehr scheint die Krankheitslast weiterhin hoch zu sein, sogar höher als von harninkontinenten Frauen, die sich nicht haben operieren lassen.
Die Autorinnen und Autoren einer aktuellen Studie aus Griechenland sind sich einig, dass Bewegungstherapie, einschließlich Übungen zur Stärkung der Bauchmuskulatur und zur Stabilisierung des Rumpfes, eine Diastase recti abdominis postpartum wirksam reduzieren kann. Doch vieles ist noch nicht eindeutig belegt.
Update Gynäkologie
Bestellen Sie unseren Fach-Newsletter und bleiben Sie gut informiert – ganz bequem per eMail.