Objective. To assess the growth and control of adrenal androgen secretion in children with virilizing congenital adrenal hyperplasia (CAH) treated with dexamethasone. Method. We examined doses used, control of adrenal androgen secretion, and growth and skeletal maturation of 8 children with CAH treated with dexamethasone beginning in infancy. Results. 3 boys and 5 girls with classical CAH (17-hydroxyprogesterone at diagnosis >20,000 ng/dL) were treated with dexamethasone beginning at diagnosis (<10 days of age). Patients were also treated with fludrocortisone and sodium chloride. The average initial medication dose was 0.1 mg (); all doses were given in the morning using a dosing syringe to administer a 0.1 mg/mL elixir. The children were treated for years over which time the change in bone age to chronological age ratio (BA/CA) was . Most recent height Z' scores were , and body mass index (BMI) scores were . Late afternoon levels of 17-hydroxyprogesterone, androstenedione, and testosterone were ng/dL ( nmol/L), ng/dL ( nmol/L), and ng/dL; ( nmol/L), respectively. Conclusions. These observations show that low doses of dexamethasone can be used to effectively treat CAH beginning in infancy.
1. Introduction
Congenital adrenal hyperplasia (CAH) is characterized by the inability to produce adequate amounts of glucocorticoids and mineralocorticoids, and reciprocal excessive production of androgens [1‐3]. Untreated, CAH can result in adrenal crisis attended by circulatory collapse and hypoglycemia [1‐3]. Excessive androgen production can result in a prenatal and postnatal virilization [1‐3]. As result, treatment of CAH is essential for the well being of the child.
Mainstays of CAH therapy include treatment with glucocorticoids and mineralocorticoids. To date, the majority of patients with CAH have been treated with hydrocortisone, which is a compound with a short circulating half-life [4, 5]. The use of longer acting glucocorticoids including prednisone and dexamethasone has also been reported [6‐8]. Caution, though, has been recommended in using prednisone and dexamethasone due to the high potency of these compounds [4, 5].
Anzeige
When applied in the treatment of CAH, the relative potency of prednisone to hydrocortisone of 4 to 5 to 1 has been used by some groups [6]. The potency of dexamethasone relative to hydrocortisone has been regarded to be approximately 30 to 1 [9]. However, these are anti-inflammatory, not anti-adrenal potencies [10]. Rather, prednisone is approximately 15 times more potent than hydrocortisone [8] and dexamethasone is 80 to 100 fold more potent [7] than hydrocortisone in suppressing adrenal androgen production.
The use of dexamethasone in the treatment of CAH was introduced in 1971 [11]. Subsequent studies have shown that dexamethasone can control excessive adrenal androgen production used once a day, making this form of treatment convenient for families [7].
In 2000 we reported our experience using dexamethasone for the treatment of 26 boys and girls with CAH [7]. The average dose used to treat these patients was 0.27 mg/m2/day, with doses given in the morning [7]. On this regimen, there was comparable maturation of linear and skeletal growth [7]. That population of children included individuals who had treatment onset at 2.8 years of age [7]. Those studies did not report our experience of dexamethasone used in infants treated from infancy onward. We now report the outcome of children with CAH treated with dexamethasone beginning at birth.
2. Methods
This analysis was approved by the Yale Human Investigation Committee. The medical records of all patients with a diagnosis of CAH were evaluated. Patients were included for analysis if they were treated continuously with dexamethasone from infancy onward.
Anzeige
Dexamethasone was administered at initial dose of 0.1 mg each morning. A 0.1 mg/mL elixir of generic dexamethasone was used. Doses were administered between 7:00 and 9:00 a.m. using a dosing syringe. When the patients were ill, parents were instructed to give a double dose in the morning, and the same double dose in the evening for the duration of illness plus one day.
Patients were evaluated clinically every three to four months at which time height, weight, and blood pressure were assessed. Laboratory tests were obtained between 3:00 and 5:00 p.m. for determination of circulating concentrations of 17-hydroxyprogesterone, androstenedione, testosterone, renin, and electrolytes. All hormonal determinations were performed at commercial diagnostic laboratories (Esoterix Life Sciences or Quest Laboratories). Every six months, after the age of one year, radiographs of the left hand and wrist were obtained for bone age determination using the Greulich and Pyle atlas [12]. Radiographs were interpreted by pediatric radiologists who were unaware of the clinical condition of the children.
Doses were increased when the 17-hydroxyprogesterone levels were above 1,000 ng/dL and the androstenedione and testosterone levels were more than 2-fold above normal. Doses were decreased when the 17-hydroxyprogesterone levels were less than 250 ng/dL and the androstenedione and testosterone levels were normal or below normal, or there was excessive weight gain assessed at home (0.5 kg in 2 weeks). When dose adjustments were made, doses were generally changed by 10%. Laboratory testing was repeated 2 months after dose changes.
All data pertaining to height, weight, drug doses, and laboratory test results were extracted from medical records and were recorded in an Excel data spread sheet. Height and body mass index (BMI) scores were determined using United States National Center for Health Statistics (NCHS) reference charts. Data are presented as mean SEM.
3. Results
Three boys and five girls were identified as having CAH by newborn screening and treated with dexamethasone from birth. The average 17-hydroxyprogesterone levels were 58,400 12,000 ng/dL at 48 hours of age. In all patients, the diagnosis of congenital adrenal hyperplasia was confirmed by repeat measurement of 17-hydroxyprogesterone levels and/or ACTH stimulation testing using standard criteria [13]. The average age at diagnosis and treatment onset was 8 2 days.
Seven infants were diagnosed with 21-hydroxylase deficiency; one infant had 11-hydrolase deficiency. The average Prader score of girls was 3.2 0.3. The individual with 11-hydroxylase deficiency was Prader stage 4 at diagnosis. All patients were also treated with 0.1 mg of fludrocortisone once daily, plus 1.5 mL, three or four times a day, of 23% sodium chloride solution orally.
For the patients with 21-hydroxylase deficiency, average late-afternoon 17-hydroxyprogesterone levels were 780 238 ng/dL (23.4 7 nmol/L) (Table 1). Androstenedione levels were 42 10 ng/dL (1.4 0.3 nmol/L). Testosterone levels were 11.5 3 ng/dL (0.4 0.1 nmol/L). [Normal levels for prepubertal individuals: 17-hydroxyprogesterone 40 ng/dL, range 3 to 100; (1.4 nmol/L, range 0.09 to 3); androstenedione, 25 ng/dL, range of 8 to 50 (1 nmol/L, range 0.32 to 2); testosterone, 5 ng/dL, range of 3 to 10 (0.17 nmol/L; range 0.1 to 0.3)].
Table 1
Circulating adrenal hormone levels for infants treated with dexamethasone for CAH.
Hormone
Normal prepubertal levels*
Infants with CAH
Fold increase
17-OHP
(ng/dL)
40 (3–100)
780 238
20-fold
(nmol/L)
1.4 (0.09–3)
23.4 7
Androstenedione
(ng/dL)
25 (8–50)
42 10
1.7-fold
(nmol/L)
1 (0.32–2)
1.4 0.3
Testosterone
(ng/dL)
5 (3–10)
11.5 3
2.2-fold
(nmol/L)
0.17 (0.1–0.3)
0.4 0.1
From Esoterix Laboratory Services, Inc.
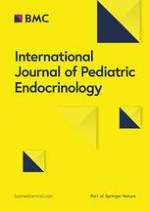
When the linear growth was evaluated, growth rate scores were 1.1 0.1 (Table 2). At an average of 6.5 years of age, height scores were 0.5 0.2 and the average body mass index (BMI) was 18.2 1.5. The mean bone age was 5.1 1.5 years, with a bone age to chronologic age ratio of 0.9 0.6 years (Figure 1).
Table 2
Clinical Characteristics of patients at end of observation period.
Age (yrs)
6.5 2
Height score
0.5 0.2
Growth velocity score
1.1 0.1
BMI
18.2 1.5
Bone age (yrs)
5.1 1.5
BA/CA
0.9 0.6
Dexamethasone dose
0.18 0.2 mg/m2/d
Figure 1
Bone age (BA) versus chronological age (CA) in individual children treated with dexamethasone for CAH. Dashed line is the line of unity.
×
Anzeige
When begun on a dose of 0.1 mg of dexamethasone each morning, seven patients did not require a change in the dexamethasone dose until 1.5 years of age. In one child, the dexamethasone dose was reduced at six months of age, as the child developed excessive weight gain. In one patient, only one dose change was made in the 5-year follow-up period; in three patients, two dose changes were made in six years; in three patients, three dose changes were made in six years; in one patient seven dose changes were made in eight years. At an average of 6.5 years of age, the average daily dose of dexamethasone was 0.18 0.5 mg/m2/d.
No patients required hospitalization for treatment of adrenal insufficiency. One child was hospitalized for treatment of gastroenteritis at 3 years of age for 24 hours. When restorative surgery was performed, patients were placed on stress dosing for 48 hours post operatively.
4. Discussion
Our results show that infants with CAH can be managed with once a day, low-doses of dexamethasone. We show that infants treated with low doses of dexamethasone for CAH have normal linear growth, skeletal maturation, and weight gain.
The use of long-acting glucocorticoids in the treatment of individuals with CAH has been greeted with controversy [4, 5]. A large part of this controversy rests on the mistaken assumption that prednisone is 5 times more potent than hydrocortisone, and that dexamethasone is 30 times more potent than hydrocortisone in suppressing adrenal androgen production. These literature entrenched equivalencies are based on anti-inflammatory properties [9]. However, as observed more than 40 years ago by Wilkins and coworkers [10], prednisone and dexamethasone are 10- and 80-fold more potent than hydrocortisone, in suppressing adrenal androgen production, respectively. When prednisone and hydrocortisone are used at 5- and 30-fold potencies relative to hydrocortisone, children will be over treated, as reflected in a recent report detailing the use of prednisone during adolescence [9].
Anzeige
The average dose initially used for treating the infants with dexamethasone was 0.25 mg/m2/day. (In comparison, most infants treated with hydrocortisone during infancy are treated with 20 mg/m2/day [14‐16].) As the infants became older, most remained on a dexamethasone dose within 30% of the dose started in infancy. Thus, at the end of the follow-up period, the average daily dose of dexamethasone was 0.18 mg/m2/day. For children treated with hydrocortisone for CAH, typical doses are 15–20 mg/m2/day [5]. Thus, compared with standard hydrocortisone doses, dexamethasone is 80–100 fold more potent than hydrocortisone.
On low doses of dexamethasone, linear growth was normal in all children. Body mass index scores were normal in all children, indicating that the children gained weight normally.
When circulatory androgen levels were assessed, they were measured at the end of the day. Testing was performed at this time, as over the years we assessed circulating hormone levels at different times of the day, and we found that late afternoon levels correlated best with dose adjustments that allowed us to optimize growth and normal weight gain. At late afternoon, circulating testosterone and androstenedione levels were close to, or 2-fold above the normal range. The 17-hydroxyprogesterone levels were 10- to 20-fold above normal.
Previous studies have evaluated long-term linear growth in individuals treated with the short-acting glucocorticoid hydrocortisone [16]. In general, these studies reveal final adult heights are 1 to 2 standard deviations below that expected [16]. In our previous studies of older children treated with dexamethasone for CAH, we observed final or projected final height standard deviations scores of 0.2 [7]. In the current study, the bone ages were slightly less than the chronological ages. Thus, based on growth and skeletal maturation parameters, the linear growth in dexamethasone-treated children appears normal. Long-term follow-up of these children will be needed to ascertain long-term outcomes more than one decade from now.
Anzeige
Although we show that dexamethasone can be used to effectively treat CAH, it is important to emphasis that dexamethasone is a very potent glucocorticoid and overtreatment can occur. To avoid overtreatment, it is imperative that the dilute elixir (0.1 mg/mL) be used, and the dose should be administered with a syringe. Although it is tempting to give the dose at night to suppress morning adrenal androgen production, nighttime dosing of dexamethasone is associated with overtreatment [17]. Thus, the morning is the favored time for administration. When dose changes are made, changes are by 10% to 20%, and we instruct families to monitor the child's weight with a scale at home. If the weight increases by 0.5 kg over two weeks, the dose is empirically reduced.
In summary, we show that treatment of virilizing CAH from infancy onward with low-dose dexamethasone is effective. Children treated with low doses of dexamethasone for CAH have normal linear growth, weight gain, and appropriate skeletal maturation. The convenience of once a day dosing, and the relatively few dose changes that are needed over the first several years of life contribute to a favorable regimen for the treatment of infants. Further studies involving larger numbers of children are indicated to assess the utility for this approach before it is broadly applied.
Open AccessThis article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution 2.0 International License (https://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

























 0.5 kg in 2 weeks). When dose adjustments were made, doses were generally changed by 10%. Laboratory testing was repeated 2 months after dose changes.
0.5 kg in 2 weeks). When dose adjustments were made, doses were generally changed by 10%. Laboratory testing was repeated 2 months after dose changes. scores were determined using United States National Center for Health Statistics (NCHS) reference charts. Data are presented as mean
scores were determined using United States National Center for Health Statistics (NCHS) reference charts. Data are presented as mean
 SEM.
SEM. 12,000 ng/dL at 48 hours of age. In all patients, the diagnosis of congenital adrenal hyperplasia was confirmed by repeat measurement of 17-hydroxyprogesterone levels and/or ACTH stimulation testing using standard criteria [13]. The average age at diagnosis and treatment onset was 8
12,000 ng/dL at 48 hours of age. In all patients, the diagnosis of congenital adrenal hyperplasia was confirmed by repeat measurement of 17-hydroxyprogesterone levels and/or ACTH stimulation testing using standard criteria [13]. The average age at diagnosis and treatment onset was 8
 2 days.
2 days. 0.3. The individual with 11-hydroxylase deficiency was Prader stage 4 at diagnosis. All patients were also treated with 0.1 mg of fludrocortisone once daily, plus 1.5 mL, three or four times a day, of 23% sodium chloride solution orally.
0.3. The individual with 11-hydroxylase deficiency was Prader stage 4 at diagnosis. All patients were also treated with 0.1 mg of fludrocortisone once daily, plus 1.5 mL, three or four times a day, of 23% sodium chloride solution orally. 238 ng/dL (23.4
238 ng/dL (23.4
 7 nmol/L) (Table 1). Androstenedione levels were 42
7 nmol/L) (Table 1). Androstenedione levels were 42
 10 ng/dL (1.4
10 ng/dL (1.4
 0.3 nmol/L). Testosterone levels were 11.5
0.3 nmol/L). Testosterone levels were 11.5
 3 ng/dL (0.4
3 ng/dL (0.4
 0.1 nmol/L). [Normal levels for prepubertal individuals: 17-hydroxyprogesterone 40 ng/dL, range 3 to 100; (1.4 nmol/L, range 0.09 to 3); androstenedione, 25 ng/dL, range of 8 to 50 (1 nmol/L, range 0.32 to 2); testosterone, 5 ng/dL, range of 3 to 10 (0.17 nmol/L; range 0.1 to 0.3)].
0.1 nmol/L). [Normal levels for prepubertal individuals: 17-hydroxyprogesterone 40 ng/dL, range 3 to 100; (1.4 nmol/L, range 0.09 to 3); androstenedione, 25 ng/dL, range of 8 to 50 (1 nmol/L, range 0.32 to 2); testosterone, 5 ng/dL, range of 3 to 10 (0.17 nmol/L; range 0.1 to 0.3)].  From Esoterix Laboratory Services, Inc.
From Esoterix Laboratory Services, Inc.
 238
238 7
7 10
10 0.3
0.3 3
3 0.1
0.1 scores were 1.1
scores were 1.1
 0.1 (Table 2). At an average of 6.5 years of age, height
0.1 (Table 2). At an average of 6.5 years of age, height
 scores were 0.5
scores were 0.5
 0.2 and the average body mass index (BMI) was 18.2
0.2 and the average body mass index (BMI) was 18.2
 1.5. The mean bone age was 5.1
1.5. The mean bone age was 5.1
 1.5 years, with a bone age to chronologic age ratio of 0.9
1.5 years, with a bone age to chronologic age ratio of 0.9
 0.6 years (Figure 1).
0.6 years (Figure 1).  2
2 score
score 0.2
0.2 score
score 0.1
0.1 1.5
1.5 1.5
1.5 0.6
0.6 0.2 mg/m2/d
0.2 mg/m2/d 0.5 mg/m2/d.
0.5 mg/m2/d.