Computed tomography (CT) is highly sensitive for the detection of coronary calcification, due to the high attenuation value of calcium. Using this property, it has been shown in multiple large prospective studies that the amount of coronary calcification, expressed as a calcium score [1], is a strong predictor of coronary events [2‐4]. Therefore, the calcium score is considered a promising method to improve cardiovascular risk stratification [5‐7]. Furthermore, the occurrence of coronary heart disease and mortality is extremely unlikely in asymptomatic individuals with a zero or very low calcium score [8, 9].
However, whether the absence of coronary calcium can also exclude the presence of obstructive plaque in patients with symptoms suggesting underlying coronary artery disease (CAD) is a matter of debate. In different studies with differing CT systems, the presence of significant stenosis on CT angiography in case of a zero calcium score ranged from 0 to 7% [10‐14]. Although some authors have suggested that the zero calcium score can reliably exclude the presence of obstructive disease, others advise to be careful with patients with zero calcium score due to the inability to rule out CAD [13‐15]. It should be proven that a zero calcium score on CT indeed means that coronary calcification is absent and that significant CAD can be safely excluded. The inability to detect small and less dense calcifications was shown in a recent phantom study, in which coronary calcification quantifications were compared between multiple 64 multidetector-row CT (MDCT) scanners from two different vendors [16].
Anzeige
The current MDCT technology has limited spatial resolution to detect small calcifications. Therefore, by using a software simulation model, we investigated the smallest calcification which can be detected by current CT technology and the spatial resolution needed to detect significant calcifications based on the commonly accepted HU-based threshold for calcification measurement in non-contrast-enhanced CT.
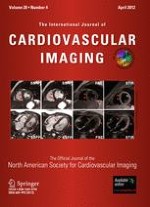
The phantom depicts an axial cross-section of a coronary vessel and was generated at 5 μm resolution to facilitate the smallest size of a single calcium granule, found in histopathology [19]. Realistic morphological features of the vessel and attenuation values of the tissues and materials were used [20‐28]. All three layers (intima, media, and adventitia) of a coronary vessel and the surrounding epicardial fat tissue were incorporated into the design of the phantom. Published attenuation values of carotid plaques were chosen. Although the studies reporting these values used contrast-enhanced CT scans, carotid plaques are generally large enough to be less influenced by partial volume effects, either from the lumen contrast-enhancement or the surrounding fat tissue. The lumen was simulated to be blood-filled, while both the normal and plaque-infested parts of the vessel were fibrous. The plaque was designed to build up in the intima area causing 50% area stenosis with a single calcification inside. The construction and dimension of the phantom is presented in Fig. 1a.
Fig. 1
The vessel phantom (a) with fibrotic plaque and a single calcification was generated at 5 μm resolution. CT scanning simulation was conducted, generating images at MicroCT (b) and 64-MDCT (c) resolution
×
Scanning simulation
X-Ray projections were simulated on the generated phantom and performed with settings based on the technical specifications of a commercially available 64-MDCT scanner (Somatom Sensation 64, Siemens Medical Solution, Forchheim, Germany). This scanner was considered to be an appropriate representative of the current clinical CT systems used in cardiac imaging. The scan settings of 64-MDCT adapted to the simulation were: the scanning voltage, amount of projections to make one image slice, and spatial resolution. The generally used 120 kV voltage setting for coronary CT calcium scoring examinations was not directly simulated by the scanning parameters. Instead, since voltage settings affect the HU values of the scanned materials, it was simulated by taking the HU values for plaque tissues in the phantom construction from studies which used 120 kV scanning voltage setting. Per 180° rotation, 1,151 projections were made, resembling the number of projections made by 64-MDCT at 330 ms rotation time. Due to the limitation of the software, the geometry of the detectors was set to be parallel instead of equiangular (i.e. equal to fan beam geometry) to mimic the configuration of 64-MDCT X-ray source-detector. However, because of the relatively small size of the phantom in comparison to the distance between X-ray source and detector, a fan-beam ray passes through the phantom in a similar way as a parallel beam ray would and thus this will not influence the results. The detector array element size was set to be 0.4 mm, the spatial resolution of a 64-MDCT. The same projections were repeated with similar settings but with the detector array element size changed to 48 μm, the spatial resolution of a MicroCT system (Kristanto et al. European Society of Cardiac Radiology, Porto 2008). Inapplicable scan settings of 64-MDCT were the pitch and scanning time because the phantom was stationery, and the slice width because the phantom was two dimensional.
Anzeige
Two other variables of clinical scans which were indirectly incorporated in the simulation were the scan current and the scanning environment inside a thorax cage. Both are known to be related to noise, affecting image quality. Adhering to this fact, an artificial noise comparable to noise in clinical scans was incorporated at the later stage of the simulation.
Reconstruction parameters
From the resulting sinograms of the X-ray projections, images were reconstructed using the filtered back projection (FBP) method with a Hanning filter and linear interpolation. The Hanning filter was selected because of its smoothing characteristics, comparable to a medium or smooth kernel, usually applied for coronary CT calcium scoring examinations. The reconstructed image pixel size was set to 48 μm and 0.4 mm to match the MicroCT and 64-MDCT spatial resolutions, respectively (Fig. 1b, c).
The parameters used for simulation are summarized in Table 1.
Table 1
Parameters used for simulation
Phantom
Element size: 5 μm
Vessel morphology
Normal wall thickness: 1 mm (intima + media + adventitia); 0.5 mm (adventitia only)a
Normal lumen diameter: 4 mmb
Vessel shape: eccentric thickening with round lumenc
Tissue attenuation value
Air: −1,024 HU
Blood: 50 HUd
Epicardial fat: −100 HUe
Fibrous plaque: 65 HUf
Scanning/X-ray projection
Detector geometry: parallel
Detector size: 48 μm/0.4 mm (MicroCT/64-MDCT)
Number of projections: 1,151
Reconstruction
Type of reconstruction: filtered back projection (FBP)
Type of filter: hanning
Interpolation: linear
Pixel size: 48 μm/0.4 mm (MicroCT/64-MDCT)
aNormal coronary wall layers thickness (for all three layers and for adventitia layer only) [23], and then rounded for simplification
cThe most common plaque-burdened vessel shape [20]
dArbitrarily chosen from the normal range of the reported value for blood. [25]
eArbitrarily chosen from the normal range used for epicardial fat [22, 27]
fAverage of published carotid fibrous plaque values [21, 24, 26, 28], and then rounded for simplification
Analysis
Since a calcification grows as several calcium granules aggregate [29], the calcification was systematically simulated to grow, starting from a single calcium granule, until it was detected by either 64-MDCT or MicroCT. The growth was simulated either by altering the attenuation value (by increasing the HU value) or the size (by increasing the diameter, assuming the granules aggregate in a circular shape), thus changing the physical properties of the calcification in the phantom images. Two parameters were investigated:
1.
Minimal attenuation value of detectable calcification
The diameters of the calcifications were fixed into several predefined sizes: 1-, 2-, 3-, 5-, and 10-pixel (with 1 pixel = 5 μm = 1 calcium granule). At each fixed diameter, the attenuation value was increased from 130 HU until it was detected by either CT system.
2.
Minimal size of detectable calcification
The second simulation assumed that calcium granules have a specific attenuation value. The attenuation value of an area will be the average of the attenuation value of all components in that area. As calcium granules aggregate and fill an entire pixel area, the attenuation value of the area will reflect the attenuation value of a single calcium granule. The attenuation value of this area will also be the highest since calcium is the densest plaque component. The maximum reported coronary calcification attenuation value was found to be approximately 2,000 HU [30]. Therefore, the attenuation value of the calcification was fixed at 2,000 HU, and then the diameter was increased starting from 1 pixel (with 1 pixel increments) until it was detected by either CT system.
The position of the calcification relative to the reconstructed image pixel borders may influence its detectability as a calcification at the center of an image pixel is blurred less than a calcification at the border of two image pixels. Therefore, additional investigation was conducted by varying the position of the calcification relative to the reconstructed image pixel(s), both for 64-MDCT and MicroCT images, into three variations: at the center of an image pixel, at the border between two image pixels, and at the border between four image pixels (see Fig. 2).
Fig. 2
The different positioning of calcification, at the image center (1), at the border between two image pixels (2), and at the border between four image pixels (3)
×
Noise could hamper the image quality and subsequently the calcification’s detectability. Artificial noise was incorporated into the simulation according to the method described in a previous publication [31], by adding Gaussian noise with zero mean and sigma (σ) standard deviation to the sinograms. The σ was set to a certain value so that the noise in the reconstructed image matched the noise in normal clinical CT images used for calcium scoring application. The normal clinical CT image sample was taken from a thorax phantom scan (QRM, Möhrendorf, Germany; see Fig. 3), scanned on a 64-MDCT scanner in sequential mode at 120 kV and 50 mAs; reconstructed using B35f kernel at 3 mm slice thickness. The noise was defined as the standard deviation inside an ROI over a homogenous area with attenuation equivalent to water. To achieve correct noise simulation in the micro CT simulation the noise has to be increased by a factor of \( N\sqrt N \), where N corresponds to the increase in resolution when compared to 64MDCT [32]. The resolution of MicroCT was 8.3 times the 64-MDCT. Therefore, the noise in the MicroCT images is approximately 24 times the noise in the 64-MDCT images.
Fig. 3
The photograph (left) and CT image (right) of the thorax phantom
×
Anzeige
Each time the calcification’s size, attenuation value, or position was changed, a new phantom was generated and a new simulation was conducted. Based on the known plaque area on the phantom image, a region of interest (ROI) was defined on all MicroCT and 64-MDCT images, enclosing the whole plaque area. Two calcification detection criteria were defined according to the clinically accepted threshold of 130 HU for the detection of calcified plaque regions in non-contrast-enhanced 64-MDCT: firstly, when there was 1 pixel and secondly, when there were more than (>) 1 pixel inside the plaque ROI exceeding the 130 HU threshold. The second criterion was based on the generally used suggestion in calcium scoring schemes, that a threshold of more than 1 pixel for calcification is necessary to avoid false calcium detection due to noise [1].
Results
No noise
1.
Minimal attenuation value of detectable calcification
The required attenuation value of 1, 2, 3, 5, and 10 pixel (5, 10, 15, 25, and 50 μm, respectively) diameter calcium granule(s) to be detectable by MicroCT and 64-MDCT is presented in Tables 2 and 3, respectively (fixed diameter Ø rows). From all the detected calcium granule(s), only calcium granules with a diameter of at least 5 pixels (25 μm) which were detected by MicroCT, had an attenuation value within normal CT values range (−1,024 until +3,072 HU). Smaller calcifications required an unrealistically high attenuation value beyond this range to be detected. The simulation was stopped when a calcification with attenuation value >300,000 HU was still not detected.
Table 2
Detection prerequisites for MicroCT with no noise present
Fixed
Detection prerequisites of a calcification located at
Center
Border 2 pixels
Border 4 pixels
as 1 pixel
as >1 pixel
as 1 pixel
as >1 pixel
as 1 pixel
as >1 pixel
Diameter Ø
1 pixel
32,000 HU
65,000 HU
42,000 HU
44,000 HU
50,000 HU
52,000 HU
2 pixels
8,000 HU
16,500 HU
10,500 HU
11,000 HU
12,500 HU
13,500 HU
3 pixels
3,500 HU
7,000 HU
4,700 HU
5,000 HU
5,600 HU
5,900 HU
5 pixels
1,300 HU
2,500 HU
1,800 HU
1,900 HU
2,100 HU
2,200 HU
10 pixels
430 HU
800 HU
500 HU
600 HU
570 HU
600 HU
Attenuation
2,000 HU
4 pixel Ø
6 pixel Ø
N.A.
5 pixel Ø
N.A.
6 pixel Ø
N.A. data were not available since with the 1 pixel increment step, the calcification was directly detected as >1 pixel
Table 3
Detection prerequisites for 64-MDCT with no noise present
Fixed
Detection prerequisites of a calcification located at
Center
Border 2 pixels
Border 4 pixels
as 1 pixel
as >1 pixel
as 1 pixel
as >1 pixel
as 1 pixel
as >1 pixel
Diameter Ø
1 pixel
>300,000 HU
>300,000 HU
>300,000 HU
>300,000 HU
>300,000 HU
>300,000 HU
2 pixels
>300,000 HU
>300,000 HU
>300,000 HU
>300,000 HU
>300,000 HU
>300,000 HU
3 pixels
210,000 HU
>300,000 HU
>300,000 HU
>300,000 HU
>300,000 HU
>300,000 HU
5 pixels
75,000 HU
130,000 HU
125,000 HU
135,000 HU
160,000 HU
170,000 HU
10 pixels
18,000 HU
30,000 HU
32,000 HU
35,000 HU
40,000 HU
41,000 HU
Attenuation
2,000 HU
35 pixel Ø
49 pixel Ø
40 pixel Ø
43 pixel Ø
N.A.
45 pixel Ø
N.A. data were not available since with the 1 pixel increment step, the calcification was directly detected as >1 pixel
2.
Minimal size of detectable calcification
The required size of 2,000 HU calcium granule(s) to be detectable by MicroCT and 64-MDCT is presented in Tables 2 and 3, respectively (fixed attenuation rows). Using 1 pixel threshold, the smallest calcification detected by MicroCT and 64-MDCT were the ones positioned at the image pixel center with 20 and 175 μm diameter, respectively, with area overestimation of 5.8 and 6.7 times, respectively. Using >1 pixel threshold, the smallest calcification detected by MicroCT and 64-MDCT were the ones positioned at the border between two image pixels with 25 and 215 μm diameter, respectively, with area overestimation of 7.7 and 8.8 times, respectively.
Anzeige
The requirement of a calcification to be detected as 1 pixel, either by 64-MDCT or MicroCT, was constantly lower for calcification positioned at the image pixel center than the one positioned at the borders. However, to be detected as >1 pixel, the calcifications positioned at the image pixel center need the highest requirements.
With noise
The noise measured at the clinical 64-MDCT image sample was approximately 10 HU. If the same scan would have been performed at MicroCT spatial resolution without additional radiation dose, the noise level would have been at approximately 240 HU, which is too high for a diagnostic image. Inserting noise of that level to the Micro CT images will practically obscure any details, let alone the visualization of a small calcification. Therefore, the noise insertion was only performed to 64-MDCT images. Introduction of noise in the simulated 64-MDCT images changed the number of the detected calcification pixels, either by reducing the HU value of the detected calcification pixel so it went below the 130 HU threshold or by increasing the HU value of non-calcification pixel so it went above the 130 HU threshold (see Table 4).
Table 4
The change of detected calcification pixels at 64-MDCT with noise present
Fixed
Change in the detected pixels
Center
Border 2 pixels
Border 4 pixels
as 1 pixel
as >1 pixel
as 1 pixel
as >1 pixel
as 1 pixel
as >1 pixel
Diameter Ø
1 pixel
N.A.
N.A.
N.A.
N.A.
N.A.
N.A.
2 pixels
N.A.
N.A.
N.A.
N.A.
N.A.
N.A.
3 pixels
0
N.A.
N.A.
N.A.
N.A.
N.A.
5 pixels
0
0
−1
−1
+1
+1
10 pixels
0
−1
−1
−1
+1
0
Attenuation
2,000 HU
−1
−1
0
0
N.A.
−1
N.A. data were not available since the simulation was not performed at this setting
One way to avoid being eliminated by the noise, the calcification pixel HU value needed to be above the noise level from the current threshold. Thus, the calcification needed to be at least 140 HU. Increasing the detection threshold accordingly, the detection requirements were updated as in Table 5.
Table 5
Detection prerequisites for 64-MDCT with noise present
Fixed
Detection prerequisites of a calcification located at
Center
Border 2 pixels
Border 4 pixels
as 1 pixel
as > 1 pixel
as 1 pixel
as > 1 pixel
as 1 pixel
as > 1 pixel
Diameter Ø
1 pixel
>300,000 HU
>300,000 HU
>300,000 HU
>300,000 HU
>300,000 HU
>300,000 HU
2 pixels
>300,000 HU
>300,000 HU
>300,000 HU
>300,000 HU
>300,000 HU
>300,000 HU
3 pixels
250,000 HU
>300,000 HU
>300,000 HU
>300,000 HU
290,000 HU
>300,000 HU
5 pixels
85,000 HU
150,000 HU
145,000 HU
155,000 HU
185,000 HU
190,000 HU
10 pixels
20,000 HU
35,000 HU
37,000 HU
39,000 HU
46,000 HU
47,000 HU
Attenuation
2,000 HU
38 pixel Ø
53 pixel Ø
43 pixel Ø
46 pixel Ø
45 pixel Ø
48 pixel Ø
Discussion
In this software simulation study, the attenuation value and size requirement of small calcifications necessary to be detectable by current clinical CT systems (represented by 64-MDCT), were systematically investigated. Very small calcifications (≤50 μm diameter) needed an unrealistically high attenuation value, while calcifications of a realistic attenuation value had to have at least a 215 μm (0.215 mm) diameter. Calcifications with a size or attenuation value below these requirements would simply be blurred out due to partial volume effects.
Anzeige
Contrast-enhanced coronary CT angiography examinations have been widely used for coronary artery disease examination, both for coronary lumen and wall assessment [33‐38]. However, coronary calcification quantification based on non-contrast-enhanced coronary CT remains a solid assessment tool for predicting coronary event risk [2‐4]. It has been associated with total plaque burden [39]. Although extensive calcifications are associated with more stable plaques [40‐42], they are frequently found in ruptured plaques according to a histopathology study on victims of sudden coronary death [43]. However, speckled calcifications are more commonly associated with ruptured and vulnerable plaques than diffuse calcification [44]. Above all, mixed plaques with predominantly non-calcifying component are associated with acute coronary syndromes [40]. Some studies have shown that absence of coronary calcium can 100% rule out the presence of significant CAD on CT angiography in symptomatic patients [10, 12]. Other studies have found contradicting results, with significant stenoses in up to 7% of patients with zero or very low calcium score [11, 13, 14]. The sensitivity of the CT technique applied may play an important role. Furthermore, dependency of coronary calcification quantification on acquisition mode, quantification algorithm, and vendor were reported [45]. A study comparing coronary calcification quantifications by multiple 64-MDCT scanners from two different vendors addressed the inability to detect all small and less dense calcifications by all 64-MDCT scanners [16]. One pathological study reported a few missed calcifications by MDCT [46]. Another pathological study supports our findings, describing the limitations of 64-MDCT in detecting small calcifications and also the overestimation of the detected calcifications area [47]. A recent clinical study reported missed small calcifications by contrast-enhanced MDCT and confirmed the limited spatial resolution as the main cause instead of the lumen contrast-enhancement influence [48].
Stary et al. [49] noted that calcifications could be observed at the same time as the plaques reached an advanced stage. However, a recent finding shows that micro-calcifications (sized 1–10 μm) are already present in an early type of atherosclerotic plaque, indicating the possibility of calcium to be a marker for early development hereof atherosclerosis [50]. Vengrenyuk et al. [51] hypothesized that micro-calcifications in the thin fibrous cap covering a lipid pool could destabilize the plaque to the point of becoming rupture-prone. However, for these micro-calcifications to be detectable by 64-MDCT, an unrealistically high attenuation value is needed. A MicroCT is necessary to detect these micro-calcifications, while a macro CT, such as the 64-MDCT, is limited to larger coronary calcifications. Langheinrich et al. [52] showed that MicroCT with 12 μm spatial resolution could visualize small (<100 μm2 or ~10 μm diameter) and very dense iron deposits. However, as the spatial resolution decreased, these iron deposits became blurred out and at a spatial resolution of around 50 μm, they started to be completely blurred out. This concurred with our results in a MicroCT of similar spatial resolution (48 μm), in which calcification of a similar size (2-pixel or 10 μm diameter) and a similar attenuation value as the iron deposits started to be detected (see Table 2).
The presence of noise influenced the detectability of small calcifications, affecting more than half of the detected calcifications by 64-MDCT. The effect of noise may be avoided by setting a higher HU threshold for calcification detection. However, it will also mean that only larger and denser calcification can be detected, while smaller and less dense calcification will be missed. No noise evaluation was performed for the MicroCT images as the increased noise level will severely limit further evaluation.
The current developments in CT, in term of spatial resolution, are marked by the introduction of a new 230 μm-spatial resolution CT system [53] and the emerging technology of a 200 μm-spatial resolution flat panel CT system [47]. Higher spatial resolution may allow CT systems to detect smaller calcifications, but the main challenge lies in dealing with the accompanying higher noise level while keeping the radiation dose comparable to clinical settings [32, 52]. Technological advances such as the iterative reconstruction algorithm may offer a solution to this problem [53]. So far in vivo modalities that may visualize ultrasmall calcifications are invasive modalities such as intravascular ultrasound (IVUS) and optical coherence tomography (OCT) [54]. However, invasive modalities can only be applied in selected high-risk patient groups.
The calcification quantification method used in this study follows the commonly accepted threshold-based calcification quantification method [1]. The method is simple yet effective, as has been shown in many studies. However, the usage of a fixed threshold to quantify coronary calcification may not properly take into account the true volume of calcification. Advanced new image post-processing techniques may improve the current established calcification quantification method.
This study does not simulate different types of vessel remodeling as the type of remodeling should not have any influence on the visualization of small calcifications. However, it is of importance in non-calcified plaque attenuation value measurements as plaque, which causes positive remodeling, had a low attenuation value, which is associated with higher vulnerability [55]. The lack of physical CT scanning properties in this study is compensated by the fact that software simulation can systematically adjust individually influencing factors while mimicking the technical settings of a CT system as closely as possible. Due to the simulation software limitation, however, some parameters, such as the X-ray source-detector geometry, can only be approximated. This also applies to properties such as the reconstruction filter details, since these are not always disclosed by the CT vendor. The analysis is limited to two dimensional (2D) images also because of the limitation of the simulation software. However, since calcification measurement is commonly assessed based on its area [1, 39, 47], our result should sufficiently show 64-MDCT limitations in detecting calcification. Also it should be noted that calcification is a three-dimensional (3D) object and its volume comparison to the image voxel size can play a role in the partial volume effect. Although cardiac motion has been reported to affect the coronary calcium score [56], the effect of motion on the detection of small calcifications was excluded in this current study. However, it is expected that including motion will increase the size and attenuation value requirement of a small calcification to be detectable by 64-MDCT. The ideal noiseless and motionless environment gave us the opportunity to focus our study on the relation between spatial resolution and the detectability of a small calcification. Future work should incorporate all these considerations to provide even more solid proof on how small calcifications may be missed by 64-MDCT or current clinical CT systems in general.
In conclusion, 64-MDCT is only able to detect coronary calcifications with minimal diameter of 215 μm, which is approximately 40 times the smallest reported calcium granule size. Consequently, early onset of calcification in coronary plaque indicating early progression of disease and increased coronary risk to the patient will go undetected when using a clinical CT system; and a zero calcium score can not exclude the presence of coronary calcification.
Acknowledgments
Conflict of interest
None.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Open AccessThis is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Mit e.Med Innere Medizin erhalten Sie Zugang zu CME-Fortbildungen des Fachgebietes Innere Medizin, den Premium-Inhalten der internistischen Fachzeitschriften, inklusive einer gedruckten internistischen Zeitschrift Ihrer Wahl.
Ein signifikanter Anteil der Fälle von plötzlichem Herztod ist genetisch bedingt. Um ihre Verwandten vor diesem Schicksal zu bewahren, sollten jüngere Personen, die plötzlich unerwartet versterben, ausnahmslos einer Autopsie unterzogen werden.
Kommt es zu einer nichttraumatischen Hirnblutung, spielt es keine große Rolle, ob die Betroffenen zuvor direkt wirksame orale Antikoagulanzien oder Marcumar bekommen haben: Die Prognose ist ähnlich schlecht.
Nicht nur ein vergrößerter, sondern auch ein kleiner linker Ventrikel ist bei Vorhofflimmern mit einer erhöhten Komplikationsrate assoziiert. Der Zusammenhang besteht nach Daten aus China unabhängig von anderen Risikofaktoren.
Bei adipösen Patienten mit Herzinsuffizienz des HFpEF-Phänotyps ist Semaglutid von symptomatischem Nutzen. Resultiert dieser Benefit allein aus der Gewichtsreduktion oder auch aus spezifischen Effekten auf die Herzinsuffizienz-Pathogenese? Eine neue Analyse gibt Aufschluss.
Update Kardiologie
Bestellen Sie unseren Fach-Newsletter und bleiben Sie gut informiert.