Low fingertip temperature rebound measured by digital thermal monitoring strongly correlates with the presence and extent of coronary artery disease diagnosed by 64-slice multi-detector computed tomography
verfasst von:
Naser Ahmadi, Vahid Nabavi, Vivek Nuguri, Fereshteh Hajsadeghi, Ferdinand Flores, Mohammad Akhtar, Stanley Kleis, Harvey Hecht, Morteza Naghavi, Matthew Budoff
Previous studies showed strong correlations between low fingertip temperature rebound measured by digital thermal monitoring (DTM) during a 5 min arm-cuff induced reactive hyperemia and both the Framingham Risk Score (FRS), and coronary artery calcification (CAC) in asymptomatic populations. This study evaluates the correlation between DTM and coronary artery disease (CAD) measured by CT angiography (CTA) in symptomatic patients. It also investigates the correlation between CTA and a new index of neurovascular reactivity measured by DTM. 129 patients, age 63 ± 9 years, 68% male, underwent DTM, CAC and CTA. Adjusted DTM indices in the occluded arm were calculated: temperature rebound: aTR and area under the temperature curve aTMP-AUC. DTM neurovascular reactivity (NVR) index was measured based on increased fingertip temperature in the non-occluded arm. Obstructive CAD was defined as ≥50% luminal stenosis, and normal as no stenosis and CAC = 0. Baseline fingertip temperature was not different across the groups. However, all DTM indices of vascular and neurovascular reactivity significantly decreased from normal to non-obstructive to obstructive CAD [(aTR 1.77 ± 1.18 to 1.24 ± 1.14 to 0.94 ± 0.92) (P = 0.009), (aTMP-AUC: 355.6 ± 242.4 to 277.4 ± 182.4 to 184.4 ± 171.2) (P = 0.001), (NVR: 161.5 ± 147.4 to 77.6 ± 88.2 to 48.8 ± 63.8) (P = 0.015)]. After adjusting for risk factors, the odds ratio for obstructive CAD compared to normal in the lowest versus two upper tertiles of FRS, aTR, aTMP-AUC, and NVR were 2.41 (1.02–5.93), P = 0.05, 8.67 (2.6–9.4), P = 0.001, 11.62 (5.1–28.7), P = 0.001, and 3.58 (1.09–11.69), P = 0.01, respectively. DTM indices and FRS combined resulted in a ROC curve area of 0.88 for the prediction of obstructive CAD. In patients suspected of CAD, low fingertip temperature rebound measured by DTM significantly predicted CTA-diagnosed obstructive disease.
Introduction
Despite major advances in the treatment of coronary artery disease (CAD), a large number of apparently healthy people die suddenly of a heart attack without prior symptoms and do not benefit from existing preventive therapies. Therefore, early detection and treatment of at risk individuals for primary prevention of CAD is of grave importance. Traditional cardiovascular assessment methods such as the Framingham Risk Score (FRS), which rely solely on risk factor measurement, are useful for long term prediction of risk at population levels, but are grossly inaccurate and insufficient for individualized assessment of risk [1‐3]. Measurement of risk factors such as high cholesterol does not show the vascular health of an individual. Therefore, non-invasive, individualized, direct assessment of vascular health that is superior to the FRS is needed. Multiple noninvasive imaging modalities (ultrasound, computed tomography, magnetic resonance imaging) can aid in cardiovascular risk assessment but are not feasible (due to high cost and potential adverse effects) for screening healthy populations and need for repeated uses in primary prevention settings. A low-cost and easy-to-perform test capable of direct measurement of vascular function that would provide additive value to FRS is, therefore, needed. Such a test may also complement vascular structural imaging tests such as coronary artery calcium (CAC) score and carotid intima-media thickness [4‐6].
Vascular dysfunction is generally considered a key initial event in the atherosclerotic process which is a systemic disorder local manifestation. Numerous studies have shown that functional changes in arteries precede the development of structural changes and also reverse more quickly in response to therapies [7, 8]. Fingertip Digital Thermal Monitoring (DTM) of vascular reactivity is a new non-invasive, operator-independent test based on changes in fingertip temperature during and after arm cuff occlusion. DTM has been shown to correlate with the burden of subclinical coronary atherosclerosis in asymptomatic patients, measured by coronary artery calcium and nuclear perfusion imaging [9‐12]. The present study was designed to evaluate whether vascular dysfunction measured by DTM correlates with the presence and extent of CAD diagnosed by computed tomography angiography (CTA) in patients with suspected coronary artery disease (CAD).
Anzeige
Methods
Subjects and study design
The study population includes 129 consecutive patients with suspected CAD who were referred to the CTA laboratory: 68 with typical angina, 39 with atypical angina, 15 with equivocal exercise stress tests, and seven with shortness of breath. All subjects underwent coronary artery calcium (CAC) scanning, CTA and DTM. Subjects over 35 years were eligible to participate. Patients with established cardiovascular disease, stroke, diabetic retinopathy, end‐stage renal disease, Raynaud’s syndrome, infection, cancer, immunosuppression, systemic inflammation, and end-stage renal or liver disease were excluded. Body mass index, waist circumference, blood pressure, fasting blood glucose, and lipid profile were obtained by standard techniques. Risk factors were determined and Framingham risk score (FRS) calculated [13].
Study protocols
Digital thermal monitoring of vascular reactivity
All DTM measurements were performed in the morning in a quiet, dimmed room at a controlled ambient temperature between 23.5 and 25.0°C. Female participants were examined during the follicular phase of their menstrual cycle. Studies were conducted after an overnight fast of at least 10 h (water was permitted) and abstinence from tobacco, alcohol, caffeine, vasoactive medications, exercise, high-fat foods and vitamin C. The measurements were obtained with the subjects supine and after 30 min of rest. Each patient’s blood pressure in the control arm was recorded in a sitting position 5 min before the DTM test (IntelliSense® Professional Digital Blood Pressure Monitor, HEM-907XL, Omron Inc, Illinois). DTM of both hands was obtained during 5 min stabilization, 5 min cuff inflation to 50 mmHg greater than systolic blood pressure, and 5 min deflation using an automated, operator-independent protocol (VENDYS, Endothelix Inc., Houston, TX). Thermal changes during a 5 min arm-cuff induced reactive hyperemia test were monitored continuously in the fingertip of both the occluded and non-occluded arms using VENDYS software. The device consists of a computer based thermometry system (0.006°C thermal resolution) with two fingertip RTD (Resistance Temperature Detector) fast response probes designed to minimize the skin-probe contact area and fingertip pressure, attached to the pulp of the index finger on both hands. The system includes a common automated sphygmomanometer cuff, cuff-inflation pump, and release valve to permit noninvasive measurement of arterial pressure and the control of occlusive hyperemia. Dual channel temperature data are simultaneously acquired at a 1 Hz sampling rate.
DTM indices
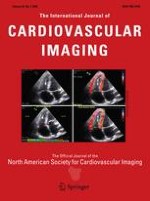
Figure 1a shows DTM indices of vascular reactivity measured based on the amount of temperature rebound (TR) and area under the temperature curve (TMP-AUC) in the fingertip of the occluded arm. Neurovascular reactivity (NVR), thermal changes in non-occluded arm during and after reactive hyperemia, was similar in the arm and finger cuff occlusive reactive hyperemia procedure (r = 0.96, P = 0.0001). Infrared Imaging shows the changes in new DTM index of neurovascular reactivity (NVR) measured based on the area under the fingertip temperature curve in the non-occluded arm during reactive hyperemia procedure. The fingertip temperature changes in the occluded arm are shown in red line and the blue line shows temperature changes in the non-occluded arm. Figure 1b illustrated a good vascular reactivity, TR and TMP-AUC, (Top) and good neurovascular reactivity, NVR (Bottom).
Fig. 1
Skin temperature changes during cuff-reactive hyperemia, as shown by infrared imaging and digital thermal monitoring (DTM). Infrared imaging reconfirms increase in non-occluded arm fingertip temperature during reactive hyperemia procedure. Both arm and finger cuff reactive hyperemia had similar neurovascular reactivity (r = 0.96, P = 0.0001)
×
Adjustment of DTM indices
aTR and aTMP-AUC were computed to account for variations in both test site conditions, such as ambient temperature and air velocity [14], and variable patient features, such as finger size, finger thermal physical properties and temperature drop from inlet arteries to venous return [15‐19]. A lumped capacity energy balance for a finger in a room with air movement shows that the finger temperature under steady state conditions depends upon the size and orientation of the finger, the ambient temperature and air flow conditions, and the finger blood flow rate and temperature drop from inlet arteries to venous return. In addition, the fall of finger surface temperature during complete occlusion of the arteries supplying blood flow depends upon the size and thermal physical properties of the finger.
From measurements of the steady state finger surface temperature and the transient response of surface temperature to occlusion, the finger thermal time constant and the heat loss characteristics to the surrounding room can be determined. This information can be used to predict the finger temperature recovery after release of occlusion for the case of zero vascular reactivity in response to the occlusion. That is, the solution to the temperature recovery assuming a step change in blood perfusion rate back to the original steady state value before occlusion can be computed. By using this solution as a baseline for comparison, the temperature increase above the zero reactivity case can be computed and used as an indication of the amount of reactive hyperemia present after release of occlusion.
One of the advantages of this approach is that the ambient temperature and ambient air flow conditions are accounted for in the zero reactivity predictions and, thus, their effects on the final results are reduced. Also, the resulting signal has a well defined maximum and area under the curve, since the difference signal starts and ends at zero temperature difference. aTR and aTMP-AUC provide indicators of the amount of reactive hyperemia present during the recovery from occlusion.
Coronary artery calcium scanning
The studies were performed with an E-Speed electron beam scanner (EBCT) (GE-Imatron, South San Francisco, CA, USA). The coronary arteries were imaged with 30–40 contiguous 3 mm slices during end-diastole using ECG-triggering during a 35 s breath hold. CAC was considered present in a coronary artery when a density of >130 Hounsfield units (HU) was detected in ≥3 contiguous pixels (>1 mm2) overlying that coronary artery; it was quantified using the previously described Agatston scoring method [20].
Computed tomography angiography
Beta blockers were administered for heart rates greater than 65 bpm. Using a dual-head power injector (Stellant, Medrad, Indianola, PA), cardiac CTA was performed with a tri-phasic consecutive injection sequence beginning with 50 ml nonionic IV contrast material (Omnipaque, Amersham Health) injected at a rate of 5 ml/s followed by 50 ml of a mixture of 60% contrast and normal saline and ending with a 50 ml flush of normal saline. Contrast was injected through an 18- to 20-gauge angiocatheter in an antecubital vein. All studies were performed by a 64 multi-detector computed tomography (MDCT) scanner (Lightspeed VCT, General Electric Healthcare Technologies, Milwaukee, WI). The following imaging and reconstruction parameters were applied: data acquisition collimation 0.625 mm × 64 = 4 cm; 140 kVp; 300–600 mAs; pitch 0.18–0.24; rotation time 0.35 s; slice width 0.625 mm; field of view 50 cm; matrix 512 × 512. Cardiac data were reconstructed retrospectively at 0–90% of the R–R interval at 0.625 mm. Coronary vessels were reviewed on the workstation using commercial cardiac volume models (AW Volume Share™, GE Medical Systems, Milwaukee, WI). Two skilled cardiologists blinded to the clinical data assessed the coronary arteries separately. Discrepancies in interpretation between the reviewers were resolved by consensus (three cases). The coronary arteries were segmented according to American Heart Association guidelines, based on 16-segment classifications for evaluation of coronary artery stenosis. Each vessel segment was assessed as normal: no stenosis and CAC score = 0, mild CAD: 1–30% stenosis, moderate CAD: 31–69% stenosis, or severe CAD: ≥70% stenosis. Each segment was also classified as normal, non-obstructive CAD: luminal stenosis <50%, and obstructive CAD: luminal stenosis ≥50%.
Statistical analysis
Mean ± SD and proportions were used to summarize the characteristics of the study sample. Continuous variables were compared by ANOVA, and categorical variables were compared by the Kruskal-Wallis non-parametric ANOVA. Multivariate linear and logistic regression analyses were employed to assess the relationship of extent of CTA-diagnosed CAD and DTM indices, with and without adjustment for conventional cardiovascular risk factors, as well as for left ventricular ejection fraction. ROC curves were constructed and the area under the ROC curve (AUC) was calculated to predict the ability of each model to detect obstructive CAD. All statistical analyses were performed with SAS version 9.1 (SAS Institute Inc, Cary, NC, http://www.sas.com). The level of significance was set at P < 0.05 (two-tailed). The study protocol and consent form were approved by IRB Committee Board of Los Angeles Biomedical Research Institute at Harbor UCLA Medical Center, Torrance, CA.
Results
Characteristics of the study population are highlighted in Table 1 according to the extent of CAD among the 129 consecutive participants (age 63 ± 9 years, 68% male). One hundred and one (78.3%) had CTA-diagnosed CAD (27 with obstructive CAD and 74 with non-obstructive CAD). There were no significant statistical differences between normal, non-obstructive and obstructive CAD cohorts in age, gender, hypertension, hypercholesterolemia, diabetes, smoking status, family history of premature CHD, left ventricular ejection fraction (LVEF), total cholesterol, HDL-C, LDL-C and triglyceride. FRS and CAC score increased significantly with increasing extent of CAD (Table 1).
Table 1
Cardiovascular risk factors, DTM indices of vascular function, and the extent of CTA-diagnosed coronary artery disease
Normal
N = 28
Non-obstructive CAD
N = 74
Obstructive CAD
N = 27
P value
Age (years)
61 ± 9
64 ± 9
65 ± 10
0.15
Male gender
68% (19)
65% (48)
67% (18)
0.8
Current smoker
18% (5)
16% (12)
18% (5)
0.8
SBP (mm Hg)
134 ± 21
134 ± 20
135 ± 21
0.9
DBP (mm Hg)
75 ± 11
75 ± 12
76 ± 11
0.6
Hypertensiona
82% (23)
84% (62)
89% (24)
0.23
Anti-hypertensive medication
87% (20)
87% (54)
91% (22)
0.57
Total cholesterol (mg/dl)
170 ± 28
172 ± 26
180 ± 26
0.19
HDL-C (mg/dl)
60 ± 16
58.4 ± 15.3
55.1 ± 15.4
0.66
LDL-C (mg/dl)
93.1 ± 28.5
98.9 ± 36.8
91.6 ± 31.4
0.37
Triglycerides (mg/dl)
91 ± 43
85 ± 39
118 ± 37
0.09
Hypercholesterolemiab
43% (12)
45% (33)
59% (16)
0.06
Cholesterol-lowering medication
83% (10)
85% (28)
81% (13)
0.61
Diabetes mellitusc
18% (5)
24% (18)
30% (8)
0.13
Family history of CHDd
32% (9)
34% (25)
37% (10)
0.8
Body mass index (kg/m2)
29.7 ± 4.1
30.3 ± 4.6
30.4 ± 3.9
0.96
Framingham risk score (%)
11.2 ± 5.9
13.7 ± 6.8
15.1 ± 7.2
0.01
LVEF
63.9 ± 4.9
64.2 ± 3.6
63.5 ± 4.6
0.77
CAC score
0
241 ± 42
720 ± 124
0.0001
Baseline fingertip temperature (°C)
29.2 ± 1.8
29.1 ± 1.9
28.1 ± 2.3
0.39
TR
1.05 ± 1.26
0.52 ± 0.85
0.16 ± 0.73
0.01
aTR
1.77 ± 1.18
1.24 ± 1.14
0.94 ± 0.92
0.009
TMP-AUC
272.6 ± 139.2
225.5 ± 152.6
144.9 ± 119.9
0.009
aTMP-AUC
355.6 ± 242.4
277.4 ± 182.4
184.4 ± 171.2
0.001
NVR
161.5 ± 147.4
77.6 ± 88.2
48.8 ± 63.8
0.015
Values presented as mean ± SD or %
NS = Non-significant (P > 0.05)
LVEF = Left ventricular ejection fraction on CTA
CAC = Coronary artery calcium score
TR = Temperature rebound in the fingertip of the occluded arm
aTR = Adjusted TR
TMP-AUC = Area under the fingertip temperature curve in the occluded arm
aTMP-AUC = Adjusted TMP-AUC
NVR = Area under the fingertip temperature curve in non-occluded arm (neurovascular reactivity)
aSelf-reported diagnosis of hypertension, prescribed medication for hypertension, or current blood pressure >140 mmHg systolic or >90 mmHg diastolic (>130/80 mmHg if diabetic)
bSelf-reported diagnosis of high cholesterol, prescribed medication for high cholesterol, or current total cholesterol > 200 mg/dl
cSelf-reported diagnosis of diabetes (type 1 or 2) or prescribed medication for diabetes
dFirst degree relative; female <65 years, male <55 years
Vascular function and coronary artery disease
Baseline fingertip temperature was not significantly different among the three groups (P = 0.39) (Table 1; Fig. 2a). Unadjusted DTM indices, TR and AUC, progressively decreased as the extent of CAD increased. Similarly, adjusted DTM indices, aTR and aTMP-AUC, significantly decreased from normal to non-obstructive CAD to obstructive CAD. Finally, the new DTM index of neurovascular reactivity, NVR, also decreased with a greater extent of CAD (Table 1; Fig. 2b–d).
Fig. 2
Baseline fingertip temperature was not significantly different among the three CAD groups (a). aTR (b) and aTMP-AUC (c), DTM indices of vascular function proportionally with the extent of CAD. NVR (d), DTM index of neurovascular reactivity, decreased from mild to moderate to severe CAD among CTA diagnosed CAD patients
×
Coronary artery calcium increased in each FRS category as vascular dysfunction increased; similarly, in each vascular function category as FRS increased. The maximum CAC was noted with the combination of the highest vascular dysfunction and CAC groups (Fig. 3a).
Fig. 3
a Coronary artery calcium increased by increasing Framingham risk score and vascular dysfunction, b extent of CTA diagnosed CAD increased with increasing coronary artery calcium and vascular dysfunction
×
Anzeige
Extent of CAD increased with increasing CAC and vascular dysfunction. The most extensive CAD was observed in the group with maximum CAC and vascular dysfunction (Fig. 3b).
In linear regression analysis of single variables, FRS, DTM indices, and CAC were all independent predictors of obstructive CAD (Table 2a). As shown in Table 2b, various combination variables of DTM, FRS, and CAC resulted in higher predictive power for obstructive CAD. Maximum predictive power was observed (R-square of 0.52) with the combination of aTMP-AUC, NVR, CAC and FRS (Table 2b).
Table 2
Linear regression analysis of the relationship between the extent of coronary artery disease diagnosed by CTA and cardiovascular risk factors (β, 95% CI)
Models
R
R2
β
95% CI
P value
a: Single variables
II
CAC
0.48
0.24
0.49
0.01 to 0.55
0.0001
III
TR
0.29
0.11
−0.34
−0.05 to −0.42
0.001
IV
aTR
0.32
0.12
−0.39
−0.02 to −0.51
0.001
IV
TMP-AUC
0.38
0.14
−0.38
−0.02 to −0.46
0.0001
V
aTMP-AUC
0.43
0.18
−0.43
−0.01 to −0.66
0.0001
VI
NVR
0.28
0.08
−0.28
−0.001 to −0.46
0.009
b: Combination variables
VII
NVR
0.40
0.17
−0.17
−0.001 to −0.45
0.01
+
aTR
−0.41
−0.003 to −0.62
0.009
VIII
NVR
0.53
0.28
−0.19
−0.001 to −0.43
0.006
+
TMP-AUC
−0.45
−0.02 to −0.64
0.0001
IX
NVR
0.71
0.51
−0.11
−0.001 to −0.19
0.03
+
aTMP-AUC
−0.46
−0.02 to −0.59
0.0001
+
0.0002
CAC
0.36
0.02 to 0.48
X
NVR
0.72
0.52
−0.14
0.001 to 0.41
0.03
+
aTMP-AUC
−0.47
−0.02 to −0.51
0.0001
+
CAC
0.35
−0.003 to −0.22
0.003
+
FRS
0.12
−0.001 to 0.21
0.2
Dependent variable: CTA diagnosed CAD
FRS = Framingham risk score
CAC = Coronary artery calcium score
TR = Temperature rebound in the fingertip of the occluded arm
aTR = Adjusted TR
TMP-AUC = Area under the fingertip temperature curve in the occluded arm
aTMP-AUC = Adjusted TMP-AUC
NVR = Area under the fingertip temperature curve in non-occluded arm (neurovascular reactivity)
Multivariate logistic regression analysis showed that DTM indices and CAC were each independent predictors of the extent of CAD (Table 3). Of note, FRS was not an independent predictor (P = 0.08). After adjustment for age, gender and conventional cardiovascular risk factors, the odds ratio of lowest versus two upper tertiles of aTMP-AUC and NVR were 5.75 and 1.46 for non-obstructive CAD and 11.62 and 3.58 for obstructive CAD compared to normal cohorts, respectively (Table 3).
Table 3
Multivariate logistic regression analysis of the relationship between obstructive coronary artery disease, increased vascular dysfunction, coronary artery calcification and Framingham risk score (odds ratio, 95% CI)
Model
Normal
Non-obstructive CAD
Obstructive CAD
Unadjusted
Odds of TR
1 (ref)
4.10 (1.8–12.7), P = 0.005
8.90 (1.9–14.6), P = 0.002
Odds of aTR
1 (ref)
4.23 (1.8–9.5), P = 0.001
10.78 (2.9–24.7), P = 0.001
Odds of TMP-AUC
1 (ref)
5.35 (2.1–9.4), P = 0.0001
10.31 (3.5–17.65), P = 0.0001
Odds of aTMP-AUC
1 (ref)
6.19 (2.4–15.9), P = 0.0001
12.14 (5.5–25.4), P = 0.0001
Odds of NVR
1 (ref)
1.59 (1.05–3.2), P = 0.04
4.69 (1.63–13.5), P = 0.004
Odds of CAC
1 (ref)
6.04 (1.3–18.6), P = 0.0001
11.87 (2.4–20.2), P = 0.0001
Odds of FRS
1 (ref)
1.09 (0.7–1.7), P = 0.74
1.72 (1.0–3.1), P = 0.08
Adjusted for age, gender, diabetes mellitus, hypertension, hypercholesterolemia, family history of CHD, smoking status
Odds of TR
1 (ref)
3.82 (1.1–14.2), P = 0.007
8.51 (1.8–19.6), P = 0.005
Odds of aTR
1 (ref)
3.90 (1.7–7.6), P = 0.001
8.69 (2.6–9.2), P = 0.001
Odds of TMP-AUC
1 (ref)
4.37 (1.7–16.1), P = 0.003
9.61 (3.1–18.1), P = 0.002
Odds of aTMP-AUC
1 (ref)
5.76 (2.1–19.6), P = 0.002
11.63 (5.1–28.5), P = 0.001
Odds of NVR
1 (ref)
1.49 (1.01–3.4), P = 0.05
3.61 (1.1–11.6), P = 0.009
Odds of CAC
1 (ref)
5.62 (1.4–12.8), P = 0.006
10.53 (2.3–25.1), P = 0.002
Odds of FRS
1 (ref)
1.04 (0.6–1.5), P = 0.85
1.69 (0.9–2.9), P = 0.21
Odds of lowest tertile versus two upper tertiles for TR, aTR, TMP-AUC, aTMP-AUC, and NVR; Odds of FRS ≥20 versus FRS <20; Odds of CAC ≥100 versus CAC <100
FRS = Framingham risk score
CAC = Coronary artery calcium score
TR = Temperature rebound in the fingertip of the occluded arm
aTR = Adjusted TR
TMP-AUC = Area under the fingertip temperature curve in the occluded arm
aTMP-AUC = Adjusted TMP-AUC
NVR = Area under the fingertip temperature curve in non-occluded arm (neurovascular reactivity)
ROC curves were constructed to assess the independent as well as incremental diagnostic value of study variables to predict obstructive CAD. As shown in Fig. 4, FRS exhibited the lowest area under the ROC curve (ROC-AUC = 0.65 ± 0.05, 95% CI 0.54–0.76). The addition of DTM indices of vascular and neurovascular reactivity to FRS progressively increased the ROC-AUC (aTMP-AUC + FRS: ROC-AUC = 0.83 ± 0.03, 95% CI 0.76–0.86) (aTMP-AUC + NVR + FRS: ROC-AUC = 0.88 ± 0.03, 95% CI 0.80–0.95), P = 0.0001 for all. Maximum predictive value was observed with the combination of FRS, aTMP-AUC, NVR, and CAC (ROC-AUC = 0.94 ± 0.03, 95% CI 0.85–0.98), P = 0.001 compared to FRS alone.
Fig. 4
ROC curves to assess the diagnostic accuracy of DTM of vascular reactivity and clinical variables for the detection of obstructive coronary artery disease
×
Discussion
The data clearly indicates a strong correlation between low fingertip temperature rebound measured by DTM and the presence and extent of CAD measured by CTA in this symptomatic population, independent of age, gender, and traditional risk factors. These results parallel our previous observations in asymptomatic populations that showed low fingertip temperature rebound measured by DTM was associated with both risk factors as measured by FRS and subclinical coronary atherosclerosis as measured by CAC [10‐12]. Our study also corroborates an earlier study by Tarjen et al. which reported that in patients with chest pain, low fingertip temperature rebound was strongly associated with myocardial infarction [9]. Parallel to this CTA study, our group has also evaluated DTM in symptomatic patients undergoing myocardial perfusion imaging (MPI) using single photon emission computed tomography (SPECT) and found a strong inverse correlation between fingertip temperature rebound (TR) and abnormal myocardial perfusion, as measured by summed stress score (SSS) [11].
Vascular reactivity: a vital component of the circulatory system
Vascular reactivity is a vital component of vascular function that enables the circulatory system to respond to physiologic and pharmacologic stimuli that require adjustments of blood flow and alterations of vessel tone and diameter [21]. Vascular reactivity can be exhibited at both the macro-vascular and micro-vascular levels. “Macro-vascular” pertains to large, conduit arteries, and “micro-vascular” refers to small, resistance vessels. Micro-vascular reactivity causes reactive hyperemia, whereas macro-vascular reactivity (flow-mediated dilatation or FMD) results from reactive hyperemia. Both macro- and micro-vascular reactivity are governed by multiple physiologic (endothelium-dependent and -independent) regulatory mechanisms and are mediated by a number of biochemical agents, such as nitric oxide (NO), endothelium-derived hyperpolarizing factor (EDHF), prostaglandins, adenosine, bradykinin, histamine, and other vasoactive substances [21‐23]. It is believed that macro-vascular reactivity is predominantly mediated by endothelium-derived NO, whereas micro-vascular reactivity is only partially mediated by NO [21, 24]. Traditionally, assessment of macro-vascular reactivity (FMD) at the brachial artery level by high resolution ultrasound imaging has been described as an endothelial function test [25, 26]. However, some believe that “endothelial function” is a misnomer because endothelial cells have numerous functions. Indeed, endothelial cells exist in all vascular beds, explaining the common root of vascular disease in various organs (such as heart, brain, kidney, eyes, legs, and urogenital) and the close correlation reported between peripheral and coronary vascular reactivity [27‐29].
Impaired vascular reactivity and atherosclerotic cardiovascular disease
Previous studies have demonstrated the relationship between impaired micro- and macro-vascular reactivity and atherosclerotic cardiovascular disease [29‐38]. Similarly, several studies have demonstrated strong correlations between endothelial-dependent and independent vascular dysfunction and cardiovascular risk factors [33]. Nevertheless, there is a considerable heterogeneity in the magnitude of vascular dysfunction in individuals with similar risk factor profiles [29, 39] In this regard, vascular dysfunction may be seen as an important “integrative factor” of the inherent atherosclerotic risk of an individual, taking into account the cumulative effect of various risk and protective factors [36]. In addition to risk assessment for prediction of outcomes, another important aspect of using vascular function is to evaluate response to therapies [40‐45].
In our recent studies of patients receiving treatments, improved vascular function measured by DTM correlated strongly with the slowed progression of CAC (r2 = 0.90, P < 0.001) and increased clearance of oxidized phospholipids (Ox-phospholipid/apoB) (r2 = 0.81, P < 0.001) [46].
Anzeige
Skin vascular and neurovascular reactivity
Skin vascular response is believed to be primarily due to micro-vascular reactivity; however, it is also mediated by neurovascular interactions. Numerous studies have shed light on the pathophysiology of skin vascular reactivity and its significance in patients with vascular disease [23, 47‐51]. Nabel et al. [52] and Prior et al. [53] have shown that the response of myocardial blood flow and epicardial coronary arteries to sympathetic stimulation with cold pressor test is significantly different in patients with and without CAD. Jzerman et al. [54] have found that individuals at high risk of CAD exhibit impaired micro-vascular function in skin. Moreover, recent studies have shown that skin vascular reactivity was significantly improved after statin therapy [44, 45, 55].
In our DTM studies, we unexpectedly found increased fingertip temperature during and after cuff occlusion in the contra-lateral (non-occluded) arm. We further confirmed our DTM findings using infrared thermal imaging of both hands (see Fig. 1a) and verified that increasing fingertip temperature in the contra-lateral hand during and after cuff occlusion was indeed due to a cutaneous vasodilative response, not from artifactual drifts in temperature probes. Although observations need additional investigations to elucidate the underlying molecular and cellular mechanism involved in this phenomenon, we believe that it is a neurovascular response and may involve endothelial- or neuronal-nitric oxide synthase (eNOS and nNOS) activity [56]. Surprisingly, in our multivariate analysis, we found that changes in fingertip temperature of the non-occluded arm (NVR) was significantly and independently correlated with both non-obstructive CAD (odd ratio 1.49 (95% CI 1.01–3.4), P = 0.05) and obstructive CAD (odds ratio 3.61 (95% CI 1.1–11.6), P = 0.009) (Table 3). The higher the NVR, the likelihood of CAD will be lower.
Vascular dysfunction and CAD in symptomatic patients
Previous studies showed that impaired vascular reactivity measured at the macro-vascular level (brachial artery flow mediated dilation) correlates with adverse outcomes in patients with chest pain but without prior CAD [57, 58]. Our study provides new evidence in addition to those reported by Tarjen et al. [9] that impaired vascular reactivity measured by DTM at the skin level (predominantly micro-vascular) correlates strongly with the presence and extent of CTA-diagnosed CAD in symptomatic patients without prior history of cardiovascular disease.
Clinical implications
The appreciation for new screening tests and better cardiovascular risk assessment of asymptomatic population who have normal cholesterol has just increased in light of the JUPITER trial [59]. In this trial of apparently healthy individuals without hypercholesterolemia but with elevated high-sensitivity C-reactive protein (Hs-CRP) levels, rosuvastatin significantly reduced the incidence of major cardiovascular events. Furthermore, the incidence of major cardiovascular events increased significantly in apparently healthy subjects with elevated Hs-CRP in the control group [52]. Although high-sensitive C reactive protein (hs-CRP) and other markers of systemic inflammation may partly reflect the effect of risk factors on vascular wall, they do not measure the status of the vascular function. Therefore, direct assessment of the vascular system is needed. Such a test must be noninvasive, easy to use and widely available in order to make a difference in the primary prevention of atherosclerotic cardiovascular disease. The strong association between vascular and neurovascular dysfunction measured by DTM shown in this study reconfirms previous findings by our group and others [9‐11, 60] and suggests a potential role for this simple noninvasive test in evaluation of at risk individuals in addition to risk factor measurements.
Anzeige
Limitation
The present study has several limitations. Tobacco, alcohol, caffeine, vasoactive medications, exercise, high-fat foods, vitamin C, and uncontrolled ambient temperature can affect vascular function assessment; however, these were taken into consideration in this study. Beta blockers which are vasoactive medications, were administered for heart rates greater than 65 bpm. However, recent studies demonstrated that concomitant therapy with non-nitrate vasoactive drugs has no significant effect on vascular function assessment [61]. Because of the cross-sectional design, we cannot establish causal relationships between CAD and DTM of vascular reactivity; however, our findings support the possibility of a link between the extent of CAD and the degree of vascular dysfunction measured by DTM. It is widely known that even severe vascular dysfunction may be present even in the absence of flow-limiting epicardial coronary lesions. However, our study demonstrated that patients with combined severe vascular dysfunction and increased FRS had a higher likelihood of non-obstructive and obstructive CAD.
Conclusion
Vascular and neurovascular dysfunction measured by DTM is associated with the presence and extent of coronary artery disease measured by CTA, independent of age, gender and traditional cardiovascular risk factors. The addition of vascular dysfunction measured by DTM to the FRS provided incremental value for the detection of obstructive and non-obstructive CAD on CTA. Prospective studies are needed to determine the clinical utility and cost effectiveness of incorporating DTM in coronary risk assessment.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Open AccessThis is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Mit e.Med Innere Medizin erhalten Sie Zugang zu CME-Fortbildungen des Fachgebietes Innere Medizin, den Premium-Inhalten der internistischen Fachzeitschriften, inklusive einer gedruckten internistischen Zeitschrift Ihrer Wahl.
Low fingertip temperature rebound measured by digital thermal monitoring strongly correlates with the presence and extent of coronary artery disease diagnosed by 64-slice multi-detector computed tomography
verfasst von
Naser Ahmadi Vahid Nabavi Vivek Nuguri Fereshteh Hajsadeghi Ferdinand Flores Mohammad Akhtar Stanley Kleis Harvey Hecht Morteza Naghavi Matthew Budoff
Wenn Eingriffe wie eine Koronarangiografie oder eine Koronarangioplastie anstehen, wird häufig empfohlen, in den Stunden zuvor nüchtern zu bleiben. Ein französisches Forscherteam hat diese Maßnahme hinterfragt.
Der Nachweis aktiver Plaques mittels 18F-Natriumfluorid-PET hilft nicht nur, infarktgefährdete Patienten, sondern auch infarktgefährdete Koronararterien zu erkennen. Von einer gezielten Behandlung vulnerabler Plaques ist man trotzdem weit entfernt.
Der GLP-1-Agonist Semaglutid hat in der FLOW-Studie bewiesen, dass sich damit die Progression chronischer Nierenerkrankungen bei Patienten mit Typ-2-Diabetes bremsen lässt. Auch in kardiovaskulärer Hinsicht war die Therapie erfolgreich.
Bei Menschen mit Typ-2-Diabetes sind die Chancen, einen Myokardinfarkt zu überleben, in den letzten 15 Jahren deutlich gestiegen – nicht jedoch bei Betroffenen mit Typ 1.
Update Kardiologie
Bestellen Sie unseren Fach-Newsletter und bleiben Sie gut informiert.