Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Dear Editor,
We read with great interest the article by Damian et al. [1], in which the authors presented for the first time the coexistence of osteogenesis imperfecta (OI) and rheumatoid arthritis (RA) [1]. More than 90% of all OI cases are caused by mutations in the alpha-1 type I collagen (COL1A1) and collagen type I alpha 2 (COL1A2) genes, leading to quantitative and/or qualitative defects in type 1 collagen [2, 3]. Despite joint pain, stiffness, and instability related to osteoarthritis have been reported in OI patients, especially affecting weight-bearing joints of the lower extremities [4], the concomitance of OI and symptomatic inflammatory joint disease is very uncommon. In the survey performed by McKiernan et al. [4], nearly half of 111 patients with type 1 OI reported a diagnosis of “non-inflammatory arthritis” (usually osteoarthritis). In contrast, only 4% of patients were affected by inflammatory arthritis (psoriatic and rheumatoid). Only three cases of RA associated with OI have been described so far.
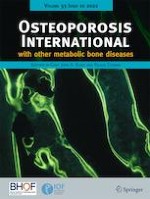
A 43-year-old female was referred to our Clinic with atraumatic joint pain, stiffness, and thirteen fragility fractures occurring from infancy to the date. She was treated with alendronate, zoledronic acid (ZA), and oral cholecalciferol due to a type I OI and adalimumab monotherapy for seropositive RA. Genetic testing to confirm OI was carried out by a t-NGS analysis of a multigene panel composed of > 5000 genes associated with Mendelian diseases. The molecular analysis identified a pathogenic heterozygous missense variant in COL1A1 gene, NM_000088:c.769 G > A, p.(Gly257Arg) (rs72645321; HGMD ID: CM960320). Of note, this variant was predicted to induce a large splicing change [5] by activating a cryptic acceptor splice site, as predicted by the human splicing finder at Genomnis webtool (https://hsf.genomnis.com/home). The impaired splicing was predicted to produce an aberrant mRNA (NM_000088.3:c.751_770del) with a subsequent frameshift at protein level, p.(Gly251Asnfs*29). Of note, COL1A1 mutations that result in premature termination codons not only may reduce type I collagen synthesis, but also may impact chain structure and processing, posttranslational modifications, and extracellular matrix interactions (Fig. 1) [1].
Fig. 1
A Alignment track of next-generation sequencing analysis of the proband showing presence of the NM_000088.3:c.769G > A, p.Gly257Arg variant as heterozygous. Below is the electropherogram confirming the variant identified by NGS. B Schematic representation of predicted activation of a cryptic acceptor site. Below is the predicted alteration of splicing with subsequent production of an aberrant mRNA
×
Anzeige
In Damian’s case, the mutation of COL1A1 gene, c.3399del, p.(Ala1134Profs*105), occurred in the major ligand-binding region (MLBR) 3; in our case, the variant c.769 G > A, p.(Gly257Arg) is located in a protein region between the MLBR 1 and 2, within the putative binding site of interleukin-2 and α2β1-integrin [6]. MLBR regions are crucial for collagen self-assembly, and they are important for interactions of collagen monomers with integrins, matrix metalloproteinases, fibronectin, and cartilage oligomeric matrix protein [7], leading to receptor-mediated signaling impairment. The bond between collagens and integrins plays a key role in the pathogenesis of RA. In addition, endoplasmic reticulum stress has been described in both RA and OI, probably caused by proteins misfolding or excess that can push cells to apoptosis or autoantigen generation, consequently activating inflammation [8]. These findings can make us speculate that systemic inflammation plays a key role in the development of both OI and RA and can modify the clinical presentations of these conditions.
Declarations
Ethics approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Consent to participate
Informed consent was obtained from the patient included in the study for the publication of any potentially identifiable images or data included in this article.
Conflicts of interest
None.
Anzeige
Open AccessThis article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Zur Zementierung einer Knie-TEP wird in Deutschland zu über 98% Knochenzement verwendet, der mit einem Antibiotikum beladen ist. Ob er wirklich besser ist als Zement ohne Antibiotikum, kann laut Registerdaten bezweifelt werden.
In der Notaufnahme wird die Chance, Opfer von häuslicher Gewalt zu identifizieren, von Orthopäden und Orthopädinnen offenbar zu wenig genutzt. Darauf deuten die Ergebnisse einer Fragebogenstudie an der Sahlgrenska-Universität in Schweden hin.
Darüber reden und aus Fehlern lernen, sollte das Motto in der Medizin lauten. Und zwar nicht nur im Sinne der Patientensicherheit. Eine negative Fehlerkultur kann auch die Behandelnden ernsthaft krank machen, warnt Prof. Dr. Reinhard Strametz. Ein Plädoyer und ein Leitfaden für den offenen Umgang mit kritischen Ereignissen in Medizin und Pflege.
Ein Frauenanteil von mindestens einem Drittel im ärztlichen Op.-Team war in einer großen retrospektiven Studie aus Kanada mit einer signifikanten Reduktion der postoperativen Morbidität assoziiert.
Update Orthopädie und Unfallchirurgie
Bestellen Sie unseren Fach-Newsletter und bleiben Sie gut informiert.